
Abstract
Purpose:
Due to improved survival rates of adolescent cancers, increasing attention is paid to addressing patients' future quality of life after treatment. A salient quality of life issue for adolescent survivors is reproductive capacity. Discussing oncofertility, that is, cancer treatment's possible effects on fertility and fertility preservation (FP) options, is a means to address this concern by informing patients and parents regarding options available to them to prevent future struggles with infertility. This systematic literature review aggregates and summarizes the attitudes, beliefs, and patterns of behavior of all stakeholders (i.e., patients, parents, and healthcare providers) in oncofertility discussions when the patient is an adolescent (12–17 years old).
Methods:
English, French, and German literature was systematically identified according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, via four databases, using several combinations of search terms. Book chapters, dissertations, and peer-reviewed qualitative and quantitative studies are included in this review.
Results:
Adolescents and parents have similar informational and counseling needs. Both seek to be fully informed about cancer treatment's effects on fertility and FP options. Adolescents have varying experiences of oncofertility discussions and decision making due to sex and/or age differences. Parents and healthcare professionals alike sometimes underestimate the importance of fertility for adolescent cancer patients. Healthcare professionals hold various beliefs and practices with respect to adolescent oncofertility discussions. Many are cognizant of the various barriers that impede successful discussion and strive to overcome them.
Conclusion:
In order to overcome discussion barriers and meet adolescent patients and their parents' informational needs, it is essential to create and implement practice guidelines, as well as properly educate and train healthcare professionals about oncofertility issues.
W
Although there are literature reviews about adolescent FP,5,6 which is an essential component of oncofertility, none exist on the discussions that take place among the healthcare provider, the adolescent patient, and his or her parents regarding the topic. To help inform recommendations and guidelines for healthcare professionals (e.g., pediatric oncologists, hematologists, surgeons, pediatricians, gynecologists, urologists, reproductive endocrinologists, nurses, psychologists, and social workers) and identify gaps in the research, this systematic literature review aims to aggregate and summarize attitudes, beliefs, and patterns of behavior of all parties involved in oncofertility discussions when the patient is an adolescent. For the purposes of this review, oncofertility discussions are those that include discussions about cancer- and/or treatment-related effects to fertility and/or FP options. This review defines adolescents as those roughly between the ages of 12 and 17 years, who are undergoing or have undergone puberty. Although legally minors, adolescents are deemed to have the capacity, or cognitive maturity, to weigh their values against the advantages and disadvantages of medical procedures, but legally lack the chronological age to provide informed consent. Therefore, in order to respect the autonomous decision making of involved parties, healthcare professionals often seek adolescents' assent (or dissent) as well as their parents' consent to perform medical procedures.7,8 Adolescents also have the physical maturity to undergo established FP techniques that collect and cryopreserve gametes.
Methods
This systematic literature review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 It includes articles identified via four databases (Web of Science, PubMed, CINAHL, and PsycInfo), published until December 31, 2014. Since FP in oncology is a relatively recent phenomenon, the search was not limited by a start date. A combination of search terms such as “pediatric/paediatric oncology,” “fertility preservation,” “adolescent,” “decision making,” “discussion,” and “oncofertility” were used (see Table 1). Three authors reviewed all resulting article abstracts in English, French, and German—the languages in which at least one author is fluent. Literature—including book chapters, dissertations, and peer-reviewed quantitative and qualitative studies—was excluded if it did not specifically address adolescent cancer patients or if it solely addressed pre-pubertal populations and/or techniques. Conference abstracts were also excluded due to their scant information. After systematic removal of duplicates and articles that met the above exclusion criteria, relevant cited references in the retrieved papers and relevant articles familiar to the authors were added. All articles were then read and summarized. Thematic analysis was then applied to these summaries to arrive at repeating themes that were then grouped into larger thematic categories.
Results
A total number of 96 articles are included in this review (see Fig. 1). The findings are grouped into four main thematic categories: the adolescent patient's perspective, the parent's perspective, the healthcare professional's perspective, and recommendations. Sixty articles touch upon the first three categories and are explored in this review (see Table 2). Three-fourths of those articles (45/60) also overlap with the thematic category of recommendations. All 80 articles that address recommendations for improving adolescent oncofertility discussions are detailed and analyzed in a forthcoming manuscript.
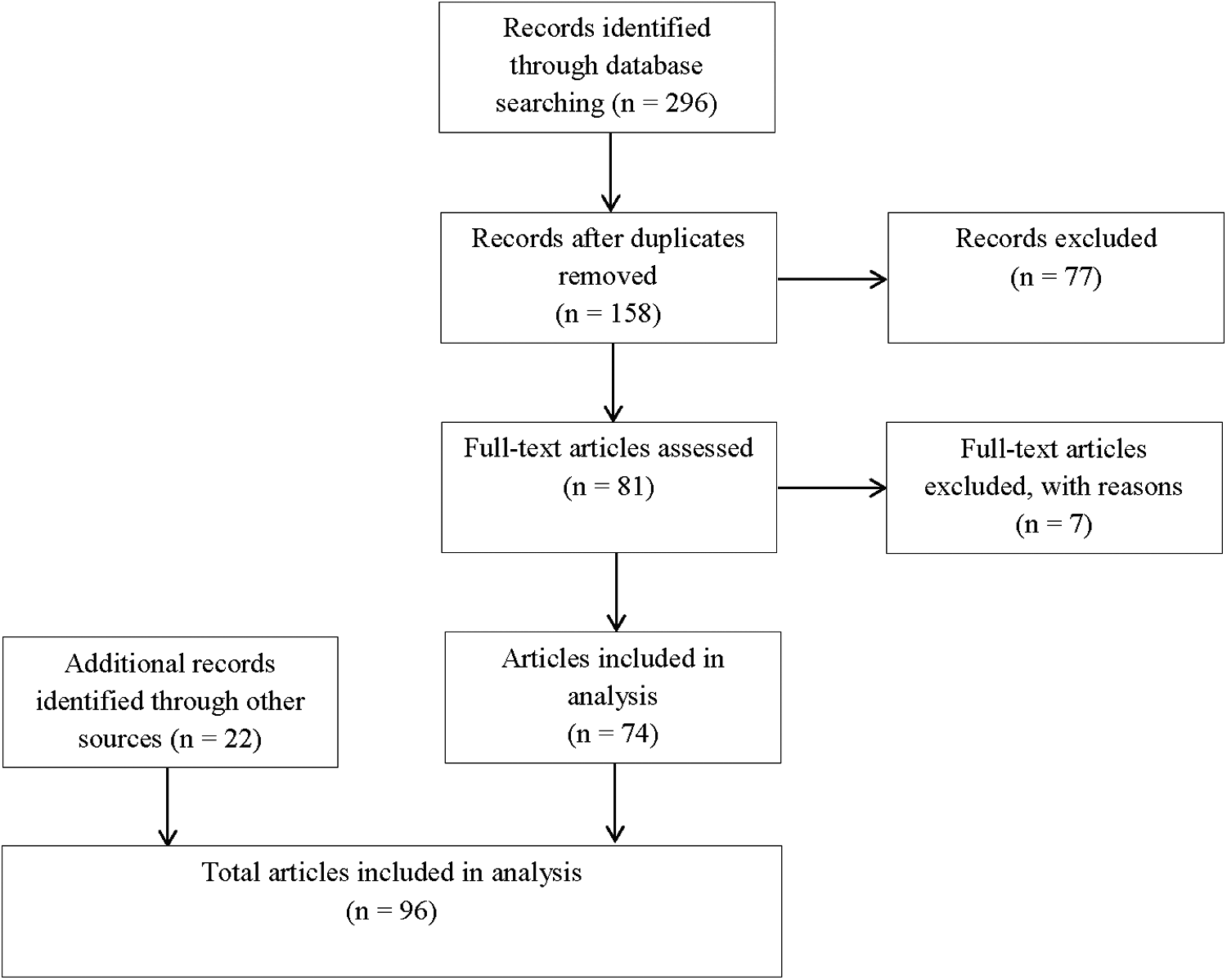
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Adolescent patients
Informational and counseling needs
Most adolescent cancer patients desire to have children,10,11 harboring existing expectations of becoming parents. 12 Regardless of whether adolescents actively contemplate parenthood, fertility may form a part of their personal and social identities. 13 Thus, adolescent cancer patients wish to be informed about treatment-related fertility issues and FP options.6,14,15 Though many would like assistance in accessing information about treatment-related fertility issues and FP options via the internet16,17 or brochures,18,19 neither can replace discussions with healthcare providers. 20
Patients greatly value having access to fertility information or when hospital staff take the time to talk to them about fertility threats 21 and listen to their wishes and feelings. 16 Adolescents support having fertility matters raised at the time of their diagnosis. 13 One grounded theory study notes strong consensus among British adolescents that professionals should talk directly to them about these matters rather than to or through parents. 13 Though many value parental support, adolescents clearly desire to have a choice in who should be included in these discussions. 13 Since adolescent patients want to talk to their peers during all stages of their illness, 16 having opportunities to meet and talk with other adolescent cancer patients can be beneficial. Regardless of acceptance or refusal of FP, adolescent patients appreciate having the option offered to them. 22 For those males who choose to bank sperm, the prompt return of sperm analysis results is a source of comfort. 22 None of the studies included in this review report similar findings for females (e.g., a specific desire to know oocyte analysis results soon after procurement).
Causes of distress
Oncofertility discussions and decisions do not always go smoothly for adolescents. Many feel rushed into making a decision about FP at a time when they feel overburdened with information and shocked by the cancer diagnosis. 23 Some find these discussions difficult either because of disagreement with parents or due to strong pre-formed desires to become a parent. 13 A cause of distress for some adolescents is professionals' misperception of their interest in fertility as less important than it actually is. 13 For those who choose to undergo FP, discontent arises when professionals do not clarify that questions about posthumous use of banked samples are routine for all (including non-cancer) patients, since adolescents could interpret such questioning to insinuate poor prognosis. 22 Some male adolescents do not appreciate having their parents accompany them to the assisted conception unit (e.g., sperm bank). 24 Many male adolescents become anxious on the way to the sperm bank and are distressed if they are not warned that attempts to masturbate might fail or that accompanying persons are seated near the semen collection room. 22 Reviewed literature did not note any female anxiety with respect to oocyte cryopreservation procedures, such as vaginal ultrasounds or taking hormones for hyperstimulation. At the conclusion of cancer treatment, adolescent survivors can experience psychological distress with respect to their uncertain fertility status.25,26
Sex differences
In one American online needs assessment of young adult cancer patients and survivors (aged 18–40 years; diagnosed 15–35 years), female patients rank the need for fertility information and services significantly higher than males do. 27 While none of the literature included in this review discusses how this differential need might be socially constructed, a German cross-sectional study of cancer patients aged 18–45 years notes females' greater desire prior to diagnosis to have children. 10 However, more males recall discussions regarding fertility and FP than females do,20,28 and in a British cohort study of survivors (aged 14–23 years; diagnosed 13–21 years), significantly more males than females recall having them before the start of treatment. 26 As healthcare professionals and female patients become more aware of fertility issues in recent years, this gendered disparity in timing of discussions becomes less apparent, whereby female survivors that recall discussions report them occurring more often before the start of treatment. 26 Regarding FP informational pamphlets, the majority of female adolescents prefer reading them with their parents, while males prefer reading them on their own.18,29
Gendered differences in adolescent survivor satisfaction with information provided during oncofertility discussions reveal relatively high satisfaction for male adolescent survivors and comparatively low levels for their female counterparts. 26 This discontent could be due to: (1) lack of established FP options for females (at the time of the study), (2) female survivors' frustration with professionals' inability to accurately assess fertility reserve at the conclusion of treatment, and/or (3) some female survivors' regular reminder of their impaired fertility status after treatment (e.g., for those that experience amenorrhea), whereas males lack such obvious indicators of sub-fertility. 26 An exploratory qualitative study carried out in England highlights the fact that uncertainty over fertility status appears to affect females more than it does males, possibly because female survivors could be more anxious over the fact that pregnancy for them can lead to obstetric complications or a risk of cancer relapse. 21
Female and male adolescent cancer patients differ in their willingness to postpone cancer treatment for FP. A delay for female patients is usually between 2 and 6 weeks, while a delay for male patients is between 24 and 72 hours. Though both might be interested in FP, the decision for female adolescents is quite complex, considering that the procedure involves a significant delay in cancer treatment of up to several weeks.15,30 On the other hand, in a survey of male patients who were approached to bank sperm at one American hospital, all perceive sperm banking as important enough to warrant postponing cancer treatment for a few days. 31
Age differences
In a study of cancer patients and off-treatment survivors between the ages of 18 and 39 years and diagnosed between 15 and 35 years, younger respondents and those diagnosed at younger ages report significantly higher needs for fertility information and services at the time of their diagnosis. 27 Another study of 55 male patients between the ages of 13 and 21 years possibly explains that this differential need could be due to the fact that younger patients experience greater levels of anxiety at the time of diagnosis and have more difficulty in talking about fertility than older adolescents. 24 Adolescent patients who attempt to bank their sperm but are unsuccessful also tend to be significantly younger than those who succeed at producing a semen sample. 24
Age might explain differences in recall or receipt of treatment-related infertility counseling. * One large-scale national German survey reports that pediatric cancer survivors diagnosed at 13 years of age or above are able to recall such counseling significantly more often than those diagnosed before puberty. 32 It is unclear whether these age differences are solely applicable to recall or also receipt of counseling because the study lacks data on actual provision of information.
Age can also influence information processing. In focus groups with healthy adolescents about their perceptions of cancer and fertility, age does not affect their predictions of eventual acceptance of fertility status, whatever it would be. 12 However, prior to such a phase of acceptance, in an attempt to search for areas of control in their life, some older adolescents (15–18 years old) speculate that they would blame or associate their infertility with cancer or its treatment. 12 In contrast, younger adolescents (12–14 years old) do not seem to place blame anywhere because they do not believe they have control over their fertility. 12
For other themes within the category of adolescent patient perspectives, please refer to Table 3.
FP, fertility preservation.
Parents
Informational and counseling needs
Like their children, parents want information about treatment-related infertility issues. 14 Even if parents are informed, not all recall such discussions. 33 Child's age at diagnosis and treatment intensity seem to affect parental recall. Parents of pubertal patients and those receiving treatment that is more likely to endanger fertility have the best recall. 33 While most parents in a British postal survey of 303 families report that fertility issues are discussed with them in a sensitive manner, they still feel that their informational needs at the time of diagnosis are unmet. 16 Parents wish for fertility specialists to be involved in such discussions, 34 and want FP to be presented as part of their child's treatment “package.” 35 Some parents desire hospital staff to provide more written and verbal information about oncofertility issues to patient's siblings. 16
Parents also need information on when and how their child's fertility can be tested, as well as guidance in how to communicate with their child about the issue as s/he matures. 17 Parents want information brochures to include testimonials from other childhood cancer survivors' experiences with fertility29,35 and information on financial assistance for FP, as well as examples of counselors and adoption agencies specializing in cancer survivors. 18
Parental information and brochure design preferences can vary according to cultural background. English-speaking American parents feel advanced terminology should be modified for their children, while Spanish-speaking American parents believe it is important to include advanced terminology because these are the terms that are used in practice. 29
Parents' understanding of adolescents' needs and concerns
A pilot study carried out at two pediatric oncology centers in the United States reports that parents often underestimated their daughters' concerns about future fertility when impacted by a cancer diagnosis. 36 (The current review does not include any similar studies with sons.) Reasons for this underestimation include parental focus on survival overshadowing adolescent normative developmental experiences and communication patterns between both parties regarding the topics of sex and reproduction. 36 Parents' culture might affect concordance between parental and child preferences and concerns. For example, in one American qualitative study, Spanish-speaking American parents more frequently express their openness to discuss fertility issues with their adolescent child compared with their English-speaking counterparts. 29 The latter group often misperceives their child's preferences with respect to content, quality, and desire for oncofertility information, while the former group tends to hold similar views to those of their child. 29 Education level may be another factor, since the above American quantitative pilot study indicates that most parents who accurately predict their child's concerns have a bachelor's degree. 36
For other themes within the category of parent perspectives, please refer to Table 4.
Healthcare professionals
Varying beliefs regarding oncofertility
A few studies investigate how important oncofertility issues are to physicians. One American online survey of pediatric oncology specialists finds that fertility threats to adolescent patients are a major concern to physicians. 37 Due to the survey's low response rate of 15%, the authors note that the results may suffer from a strong voluntary reporting bias. A couple of qualitative studies report physicians' varying beliefs regarding the importance of infertility, with some feeling it to be a serious quality of life issue, and others prioritizing disease assessment and treatment planning.38,39 Additionally, though most U.S. pediatric oncologists in the aforementioned online survey agree that pubertal patients should be told about the potential effects treatment can have on their fertility, only 79% think pubertal patients should be referred to a FP specialist prior to treatment. 37
One qualitative study notes disagreement among British fertility and pediatric oncology professionals as to whether patients or professionals ought to initiate oncofertility discussions. 40 Furthermore, when healthcare professionals believe that they should initiate these discussions, they have multiple opinions as to which specific professional should be responsible for doing so. Some oncologists believe that the responsibility should fall on other professionals, 25 particularly oncology nurses who are in an ideal position to discuss such quality of life issues because of their multiple interactions with patients prior to the start of treatment.41,42 The majority of nurses and nurse practitioners believe FP discussions to be their responsibility,41,43 and only a small number feel social workers and/or child-life specialists ought to have this responsibility. 43 In a cross-sectional survey of 58% of all Dutch pediatric oncologists, almost all believe that it is their responsibility to discuss infertility with patients or parents, while only three-fourths feel they also have the responsibility to discuss FP options. 44 Although the majority of 24 American pediatric oncologists in a qualitative study report they feel comfortable having oncofertility discussions with patients and families, some would like nurses and social workers to have follow-up discussions with the patients. 39
A few studies indicate healthcare professionals' opinions that go counter to conventional clinical ethical norms. Many healthcare professionals in an American cross-sectional survey think that adolescent patients should be told about FP and involved in such decision making, regardless of parental knowledge or consent. 41 A Dutch multicenter qualitative study of 14 physicians present similar findings. 45 Physicians maintain this attitude specifically with respect to sperm banking, arguing that parents unreliably predict their son's sexual maturity. 45 Furthermore, some healthcare professionals in a Scottish qualitative study acknowledge feeling justified in swaying patients toward making what they perceive as the “right” decisions. 20
Variation in practice
The literature is inconclusive as to whether most healthcare professionals discuss oncofertility issues. Some surveys report that a majority of pediatric oncologists talk about fertility issues with patients and their families.39,44,46,47 Other studies indicate that pediatric oncologists and nurses infrequently or inconsistently hold such discussions.25,42,48–51
Variation not only exists in professional discussion patterns, but also in referral patterns. Healthcare providers acknowledge that they discuss FP options and make referrals far more for boys than for girls.46,52 (This trend might be attributable to the fact that at the time of these studies' publication, oocyte cryopreservation was considered an experimental technique.) Surveyed healthcare professionals at one pediatric hematology/oncology department in the United States deem the success rates for female FP to be too low to justify pursuing it. 53 Disparate referral rates could also reflect the fact that most medical centers are more likely to have sperm-banking services on offer than female FP options.51,54,55 However, even within the realm of FP services for males, there seems to be great variation. 56
There is little consensus among North American pediatric cancer centers regarding standard practice for FP, such as clinical indications for offering suitable techniques. 54 As the literature notes, in the absence of clear guidelines, inconsistencies in fertility counseling endure, including who is an appropriate candidate for FP 57 or whether to approach the adolescent first, the parents first, or both together.14,39,40,58 Some interviewed physicians suggest that assessing a patient's maturity can help determine whether discussions should be had with the patient and parents together or individually. 38
Input on how to have successful oncofertility discussions
Healthcare professionals report numerous elements that help facilitate oncofertility discussions. Many in qualitative studies feel that it is vital to approach the issue in a professional manner, providing information in a clear, open, honest, and developmentally appropriate way.38,40 Some endorse an individualized rather than standard approach, based upon assessment of the patient's maturity.38,59 The availability of educational materials for patients and parents increases the likelihood of oncofertility discussion.42,43,50,60 Standardizing the process for offering FP makes conversations easier, more streamlined, and more matter-of-fact because healthcare providers become comfortable with the topic and expert in the specific skills needed to facilitate fertility referrals. 60 Protocol use can also help facilitate timely FP, preventing cancer treatment delay. 59
Regarding the content of the discussion, some interviewed physicians acknowledge the importance of specifying that preserving gametes does not guarantee that the patient will be able to later conceive a biological child. 38 Some also believe that despite the difficulty in discussing it, addressing post-mortem ownership rights over preserved gametes is essential.38,40
Barriers to oncofertility discussions
a) Systemic barriers
Among the many systemic barriers, the most cited one deals with professionals' lack of familiarity with the topic of oncofertility.25,43,48,57,61–64 Although one prospective observational study reports on British pediatric oncologists' high awareness of cancer treatments' adverse effects on fertility, 46 several studies indicate professionals' deficient knowledge in current clinical research findings with respect to treatment-related infertility risks and FP options, 53 especially concerning female options.38,44 Pediatric oncologists receive little or no formal education about FP options and their respective outcomes. 61 Additionally, they lack proper training in how to approach patients and their families regarding this sensitive topic.25,64 However, some interviewed physicians who conduct such discussions model them after those they have observed by attending physicians during fellowships. 39 Healthcare professionals also acknowledge lacking information on FP resources and costs.43,64 A lack of established relationships with professionals in other disciplines, such as endocrinology, who are more knowledgeable in these matters, contributes to this phenomenon. 39
Another oft-cited barrier for professionals to broach the subject of oncofertility with adolescent patients and their parents is inadequate funding of FP procedures and subsequent need of assisted reproductive technologies.39,58,62,63 Associated costs of FP can be prohibitive for many families, particularly when insurance policies narrowly define infertility so that iatrogenic conditions are excluded. 63
b) Professionals' attitudes or misperceptions
Numerous studies note professionals' discomfort with the topic as the key barrier to having oncofertility discussions.19,25,38,48,60,61,63–66 Such discomfort is partially due to language and cultural differences between professionals and patients/parents. 64 Some interviewed professionals feel embarrassed discussing masturbation with male adolescents, 38 especially when parents are present. 48 Lakhani suggests that physicians specifically feel uncomfortable when their medical advisory role shifts to a more psychosocial one, for which they have not necessarily been trained. 38
Another barrier to oncofertility discussions is professionals' biases. 67 Professionals may not recognize how important fertility can be for patients and parents. Adolescent shyness or embarrassment over discussing it in front of parents can be easily misconstrued as disinterest or embarrassment over discussing the topic in general,47,49,65 when it may be just initial unwillingness. 63 Moreover, while patients and their parents do not usually cite cost as a factor in FP decision making, 49 some professionals assume that families are unable to pay for FP.49,50,60,64,65,67 The aforementioned Dutch cross-sectional study also highlights professionals' lack of confidence in the effectiveness of FP techniques. 44 Some professionals consider adolescent patients, especially those in early puberty, to be too young to consider such issues.20,46,60,61 Others are biased against offering FP options to HIV positive42,43,50 or openly homosexual patients.42,50
c) Patient or family characteristics
The barrier that professionals claim most likely hampers their attempts to discuss oncofertility routinely with adolescent patients and their families is poor prognosis.25,37,41,42,44,46,47,50,64,65,67 Professionals feel that it is inappropriate to bring up such considerations in these cases, believing that doing so “adds insult to injury” for these distraught families. Furthermore, professionals consider it moot to discuss oncofertility when risk of treatment-related infertility is not significant 46 or initial prognosis is good. 20
Urgency to start treatment due to aggressiveness of cancer can be a barrier to oncofertility discussions and may leave little time to make fully informed decisions about FP.20,37,38,40,42,47,50,58 The authors of one American qualitative study report that because pediatric cancers have rapid onset and quick progression, sometimes pediatric oncologists will discuss treatment's possible effects on fertility but not FP options. 39
For other subthemes with the broader theme of barriers to oncofertility discussions, please refer to Table 5.
QoL, quality of life.
Discussion
Regardless of age or sex, adolescents want to feel that they have some degree of control during the destabilizing time of a cancer diagnosis, which is developmentally appropriate considering their evolving process of individuation. 38 Several studies of adolescent cancer patients and survivors indicate their explicit desire to access or receive oncofertility information.6,13,15–19,21,22 To meet this specific need, parents and healthcare professionals can involve adolescents in oncofertility discussions and decision making by enabling them to decide who participates in these discussions with them 17 and to what extent they want to participate in FP decision making. 68
Several studies also report on the problems that adolescents perceive in current oncofertility discussions and processes.13,22–26 It would be in patients' best interests if professional guidelines address these reported causes of adolescent distress in order to prevent and reduce it as much as possible. For example, professionals could explain to patients that while it is difficult to predict accurately the likelihood of and to what extent an individual's fertility will be affected by cancer and/or treatment, they can regularly monitor their gonadal function at the completion of treatment.11,26,62,69–71
The multiple studies that report on adolescent differential preferences or needs,10,12,18,24,27,29 as well as discrepancies in healthcare provision,15,20,26,28,30–32 warrant two responses. First, healthcare professionals could tailor their discussions or website and pamphlet designers could alter information depending upon specific age and sex preferences or needs. Second, the principle of justice underlines that professional guidelines and technological developments strive to combat discrepancies in healthcare provision based upon age and sex. The two case studies on implementing institutional protocols included in this review59,60 note successful consistency in offering FP to all eligible patients. This approach respects patient autonomy and best supports families in making informed FP decisions. Furthermore, technological advancements directed at reducing the time required for egg collection so that it is comparable to sperm collection could be a means to making FP equitable among all patients, regardless of sex.26,35
Parents, like their adolescent children, want more information about oncofertility.14,16,17 Specific input from parents and adolescent patients about their informational preferences and needs can help in developing websites and information brochures on oncofertility.17,18,29,35 When distraught parents seem overly concerned about survival, 36 it is helpful if professionals remind them that their child will likely survive treatment and that his/her future quality of life requires attention. This includes a frank discussion about all available family-building options for the patient.10,56,65,70,72–77 Holding such discussions with all stakeholders (together or separately) helps to achieve the ultimate goal of shared medical decision making, which demonstrates respect for the autonomy of all parties. 68
Aside from highlighting healthcare professionals' various beliefs and practices regarding oncofertility, the above literature review notes that many healthcare professionals are aware of both the barriers to and best practices in having oncofertility discussions. Properly educating professionals about oncofertility issues and FP options is essential to overcome many of the discussion barriers noted by healthcare professionals. Adequate education and training not only prepares professionals to discuss these topics,25,38,43,44,48,53,57,61–64 but can also help remove professionals' biases and misconceptions.19,20,25,38,44,46,48–50,60,61,63–67
Research gaps
Despite the breadth of literature on the topic of adolescent oncofertility discussions, several gaps persist. First, many of the present findings come from cross-sectional qualitative or small-sample quantitative studies. There is a dearth of longitudinal studies pertaining to these discussions and subsequent decision making. To prevent future harm to patients and parents, it is important to understand if and how their perceptions and decision making change over time. Additionally, longitudinal studies on professional beliefs and practices can measure if and how these change over time, especially in light of any training, professional guidelines, and/or institutional policy development and implementation.
The literature could also benefit from studies that incorporate multiple sites and/or that use methodologies that would allow generalizability. The majority of articles included in this review are single-site studies. For the limited number of multi-site studies included in this review, the sample size is small, and sites are always within the same country. International comparative studies could shed light on how contextual differences influence stakeholders' perspectives and professionals' practices. Such studies can assist in developing culturally specific guidelines. Furthermore, research on adolescent oncofertility discussions must expand beyond English-speaking countries and Western Europe. The vast majority of included articles focus on these discussions in the United States and United Kingdom. Including French and German articles in this review resulted in only one additional empirical study.
Finally, aside from differences with respect to patient age and sex, no included studies report on differences due to diagnosis. It is unclear whether this is due to diagnosis being an irrelevant factor or that included study designs simply do not address it. Therefore, future studies should include purposive sampling of diagnosis as part of their designs. These studies could determine whether it is necessary to develop oncofertility counseling guidelines that are diagnosis-specific.
Limitations
The results of this systematic literature review are limited by the specified combination of search phrases. The inclusion of search phrases such as “teen,” “young adult,” and “cancer” could have resulted in additional literature, detailing other perspectives not present in this review. The search was also limited by the fact that MeSH terms were not used. Restricting the search to articles in English, French, and German additionally limited the results to Western perspectives.
The recommendations put forth in this review are based on various studies with their own limitations. As previously noted, some studies are pilots, several are small-sample quantitative surveys, and many are qualitative in nature. A few studies also suffer from poor response rate. Thus, their results are specific to the studied population and not necessarily generalizable. Despite these limitations, patterns exist across the literature, which are important to highlight for the specific aim of improving oncofertility discussions for the benefit of all involved parties.
Furthermore, “adolescent” is not specifically or uniformly defined across the included literature. Some articles present adolescents as part of pediatric populations, some with young adult populations, and some as a separate population on its own. Using the aforementioned definition of “adolescent” as a pubertal individual roughly between the ages of 12 and 17 years, this review includes literature from diverse viewpoints on adolescence.
Lastly, the American Society of Reproductive Medicine's 2013 guidelines on mature oocyte cryopreservation changed the procedure's designation from experimental to an established method of female FP. This could have implications on practices and beliefs that are not captured in the studies included in this review.
Conclusion
Oncofertility discussions can lead to a multitude of experiences for all stakeholders. Some patterns of adolescent experience seem to exist along sex and age lines. Adolescent patients and parents often have similar informational and emotional needs and desires for oncofertility discussions. Unfortunately, sometimes parents and/or professionals are not fully aware of how important fertility is to adolescents. Parents and healthcare professionals can differ in their opinions over adolescent involvement in oncofertility discussions and decision making. To attain the desirable goal of shared medical decision making within the patient–parent–professional triad, it is advisable to include adolescents in oncofertility discussions and decisions to the extent that they themselves wish to be involved.
This literature review reveals that despite various barriers, when armed with adequate education as well as an informed approach and practice guidelines/standards, healthcare professionals can properly meet patient and parent needs in oncofertility discussions. However, in order to continue to meet family needs regarding oncofertility discussions, more research must be conducted to understand the needs and preferences of both patients and families, as well as their decision making processes regarding FP. Designing studies that use random sampling to ensure generalizability, that are longitudinal in nature, and that are carried out in many sites as well as in international sites is crucial to improve the quality of life of adolescents with cancer.
Footnotes
Acknowledgments
The authors would like to thank the Botnar Foundation of the University of Basel for funding this study.
Author Disclosure Statement
No competing financial interests exist.