
Abstract
Purpose:
Health literacy is important for health outcomes in adults. However, little is known about the health literacy of adolescents and young adults (AYAs). The purpose of this study was to provide an updated systematic review examining health literacy among AYAs with and without chronic illness. Specifically, the review considered (1) what sources of health information AYAs use; (2) how well AYAs are able to understand, communicate, and critically evaluate health-related information; and (3) whether health literacy is associated with health behaviors and outcomes.
Methods:
A systematic search was conducted for literature published in peer-reviewed journals using Medline, Embase, and PsycINFO databases.
Results:
Of 603 articles reviewed, 14 studies met the inclusion criteria, six of which examined health literacy in a chronic illness population. Studies reported high usage for information sources, though no clear links between source type and health literacy emerged. Adequate health literacy was reported in at least 60% of participants, though poor functional literacy was reported. Few studies explored communicative or critical health literacy; those that did indicated that AYAs experience challenges in these domains. Poorer health literacy was associated with some adverse health outcomes, such as obesity and smoking. For AYAs with a chronic illness, there were mixed findings between health literacy and medication adherence.
Conclusion:
Understanding the challenges AYAs face with regards to complex developing communicative and critical health literacy skills is crucial. Due to the paucity of research in this field, addressing health literacy across all AYAs will provide a valuable step in guiding research in AYAs with cancer.
H
Health literacy is known to be associated with important healthcare and medical outcomes among adults, 6 as well as child outcomes based on caregivers' health literacy. 7 Beyond its impact on patients' abilities to understand health information, low health literacy influences important behavioral and public health outcomes, including increased hospital admissions, health expenditure, and mortality rates.8–10 In cancer populations specifically, health literacy has been shown to be positively related to health-related quality of life. 11 Low health literacy may lead to misconceptions about their disease and prognosis, which can lead to poor adherence, dissatisfaction with care, and greater anxiety. 12 The high incidence of poor health literacy make it an increasingly important public health concern.4,13
Little is known, however, about the health literacy of AYAs. One earlier review estimated that at least one in three AYAs had low health literacy skills. 7 Similarly, Australian population data have indicated that only a third of 15–29 year olds had adequate or better health literacy. 5 AYA years are developmentally critical, as young people move toward attaining autonomy and develop important adult social, emotional, and cognitive skills, 14 including assuming responsibility for their own healthcare. One implication of these unique features is that AYAs may be vulnerable to having underdeveloped health literacy skills relative to older adults. 15 AYAs' emerging socio-emotional and communicative skills may make effectively managing interactions with the healthcare system challenging.15,16 At the same time, it is during this period that AYAs begin to assume the role previously held by their parents, and take primary responsibility for their own healthcare.15,17 This shift is consistent with AYAs' documented desire to be “in control” of health-related interactions.18–20
There is increasing acknowledgement of the need to equip those AYAs with a chronic illness with the skills to transition successfully from pediatric to adult services.12,21 Across Western nations, approximately 20–30% of AYAs live with chronic illnesses (defined as those lasting longer than 6 months; e.g., cancer, diabetes, and asthma). 22 Of these, 10–13% live with potentially life-limiting or life-altering conditions requiring regular medical intervention that significantly impacts their daily life. 22 Medical advances in the treatment of once life-threatening conditions, such as cancer, has meant that increasing numbers of AYAs live with the ongoing aftereffects of their diagnosis.23,24 Health literacy skills are therefore especially critical for young people managing the demands of chronic illness. 25
Relative to healthy peers, AYAs with chronic illness are often expected to show a greater degree of healthcare autonomy at an earlier stage. 19 Despite this, whether AYAs with chronic illness possess adequate health literacy skills remains unknown. Other aspects of AYAs' engagement with their healthcare have been documented, however. AYAs with chronic conditions, including cancer, often show a decrease in self-care and treatment adherence.16,26 Some AYAs also engage in risky health behaviors (e.g., alcohol use, unsafe sex) that, while developmentally normative, can exacerbate their conditions. 27 Health behavior in adolescence predicts health behavior and chronic disease risk in later adulthood,28,29 Although the association between health literacy and AYAs' health behaviors is unclear, research suggests that young people with low literacy skills are more prone to engage in risky behaviors related to substance use and sexually transmitted diseases. 7
The AYA years may be a pivotal stage for intervention, at a time when young people are developmentally poised to attain and apply the necessary skills to engage effectively with their health. 30 Given that Nutbeam's conceptual model of health literacy notes that health literacy existing along a continuum, preventative health education may provide a valuable role in facilitating the development of health literacy. 31 Despite a wealth of knowledge about adult health literacy, little is known about AYA health literacy and how it impacts their care and outcomes. Sanders et al. 7 reported the prevalence of health literacy difficulties among AYAs. However, no studies examining health literacy among AYAs living with chronic illness were available for analysis at that time. Understanding what forms of health information AYAs use, and how well they are able to use them, is critical to develop evidence-based intervention strategies, and to inform research in areas such as AYA oncology. The recent focus on AYA populations within several health settings, 32 combined with the increasing emphasis on delivering health-information in a “youth friendly” manner using emerging technologies33,34 such as apps and the internet, means that new literature may recently have emerged examining AYAs' capacity to engage with health-related information.
The objective of this review was to provide a comprehensive, updated review of the literature examining health literacy in AYAs with and without chronic conditions in order to guide practice recommendations and inform the development of health education interventions. The review also intends to provide guidance for future health literacy research in more specific populations such as AYAs with cancer. In addition, this review aimed to extend previous reviews by examining AYAs' health literacy in terms of their functional, communicative, and critical components.
3
In particular, this review aimed to address three questions:
Methods
Search strategy
Three online databases (MEDLINE, EMBASE and PsycINFO) were searched using the following search terms: [“health literacy”] AND [“educational status” OR “comprehension”] OR [“health education” OR “information seeking behavior”] OR [“attitude to health” OR “health behavior”]) AND [“adolescent” OR “young adult” OR teen$]. Results were limited to human studies published in English, and, where available, AYA age groups. The OpenGrey and Grey Literature Report databases were searched for gray literature. The reference lists of relevant captured articles were also screened for additional articles.
Selection criteria
Eligible studies were limited to those published from January 1, 2009, to March 30, 2015, to provide a systematic update of literature published since Sanders et al.'s earlier review.7,35 Due to the controversy of defining AYAs, AYAs were defined here as young people aged 10–39 years in order to encompass the World Health Organization's definition of those aged 10–24 years 36 and the National Cancer Institute's definition of those aged 15–39 years. 37 This range enabled the broadest set of AYA-relevant studies to be captured, and ensured that the lower and upper limits of different definitions across countries such as the United States, the United Kingdom, and Australia were covered. Studies involving AYAs with and without any chronic health condition were included. Studies focused on parent/caregiver outcomes were excluded.
Studies were required to examine at least one type of health literacy quantitatively (i.e., functional, communicative, or critical health literacy), though a validated measure was not essential. Types of health literacy were operationalized by the team of authors (including two psychologists and a medical student) based on Nutbeam's model of health literacy, in consultation with a consumer group of AYA cancer survivors. These include functional health literacy if they assessed or measured literacy, numeracy, information search skills, and information sources; communicative health literacy if they examined processes related to decision making, healthcare-related discussions, and interactions around health information; and critical health literacy if they examined how individuals evaluated or critically appraised the validity or relevance of health information. In line with Sanders et al., 7 studies relating to specific types of health literacy (e.g., mental and oral/dental health literacy) were excluded. All types of health behaviors were examined, including exercise, nutrition, sexual health, and medical treatment adherence.
Data extraction
Figure 1 depicts the abstract search and article selection process. Two researchers (M.L. and M.S.) screened 603 records. Full-text articles were examined when abstracts did not yield sufficient information to determine eligibility (n = 38). Interrater reliability was 96% (25 disagreements out of 603 records). Consensus between the reviewers was achieved by discussion of the full text.
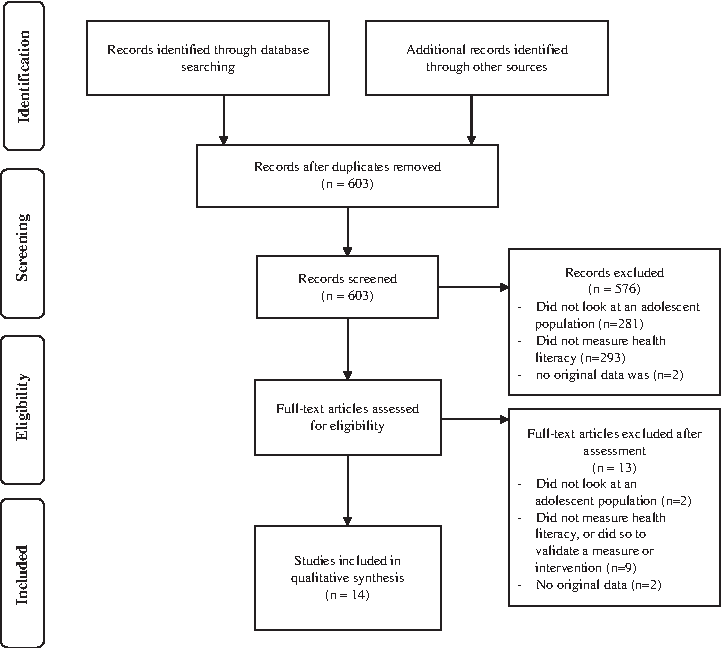
Search and selection process for included articles.
Two investigators (U.S.D. and M.L.) categorized studies as addressing functional health literacy, communicative health literacy, and/or critical health literacy.
Methodological quality
Two investigators assessed the quality of the final 14 studies (M.L. and M.S.). Quality assessment was based on the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist for cohort, case-control, and cross-sectional studies. 38 Criteria assessed included clear reporting of study design, methodology, statistical analysis, interpretation, and disclosure of funding.
Results
Description of included studies
Of 603 articles captured by the search criteria, 14 studies were eligible, representing a combined sample of 16,464 AYA participants (Table 1). All were cross-sectional, mostly conducted in North America (n = 11), and fairly evenly divided between AYAs with and without chronic conditions (n = 6 and n = 8, respectively). Of the six articles examining health literacy in AYAs with chronic conditions, four involved AYAs with HIV. Most studies in healthy samples involved high-school/college cohorts (n = 5). Five studies examined health behavioral outcomes, including nutritional and obesity-related outcomes, physical activity, medication adherence, and substance use. Most studies measured health literacy using validated scales, with three using questionnaires purposely designed.39–41 Consistent with previous findings, 7 the most frequently used measure of health literacy across studies was the Test of Functional Health Literacy in Adults (TOFHLA) and its variants, used in six studies.41–46 See Table 1 for more details.
The cs-TOFHLAd was validated in a later study.
The Adolescent Trials Network is a collective of individual investigators and groups conducting research in young people up to 25 years of age either infected with or at risk of infection with HIV.
Participants were not selected based on any condition, but were selected from waiting rooms of clinics.
ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; BAMS, Beliefs about Medications Scale; BSI, Brief Symptom Inventory; cs-TOFHLAd, Chinese short form Test of Functional Health Literacy in Adolescents; eHEALS, eHealth Literacy Scale; HINTS, Health Information National Trends Survey; HIV, Human Immunodeficiency Virus; HL, health literacy; HPBS, Health Promotion Beliefs Scale; MCQ, Multiple Choice Questionnaire; NVS, newest vital sign; REALM-Teen, Rapid Estimate of Adult Literacy in Medicine-teen; SD, standard deviation; SHLS, Swiss Health Literacy Scale; STROBE, STrengthening the Reporting of OBservational studies in Epidemiology; TOFHLA, Test of Functional Health Literacy in Adults.
Methodological rigor
Papers had an average study quality of 19/25 (range 11.5–22.5), as measured by STROBE (see Table 1 for scores; 71.42% agreement). The generalizability of the findings to broader AYA populations is limited, with only English literature included, most studies undertaken in North America (n = 11),40,41,43–51 and with very specific groups (e.g., college students). All but one study recruited AYAs with a chronic illness from multidisciplinary, primary-care clinics.45,46,50,51
Almost all studies (n = 8)41–46,48,49 used only brief measures indexing basic, functional health literacy skills (e.g., word comprehension), to the exclusion of other more complex aspects of health literacy such as oral, numeracy, and navigational skills.
RQ1: What sources of health information do AYAs use?
Internet
Seven studies examined health resources used by AYAs, three of which focused primarily on “eHealth literacy” 52 (referring to the use of new information and communication technology, especially the internet, to improve health and healthcare) 53 or health literacy related to electronic sources (Table 2).45,46,48 Studies reported that 48–71% of AYAs had accessed online health information in the last year. Studies also reported that most AYAs (70%) would use the internet as their first source of health information, with AYAs perceiving online health information as “easy” or “very easy” to understand. 54 A total of 75% of AYAs had used the internet in their most recent search for health information. 47
Viral loads and CD4 counts are common markers of HIV activity.
No differentiation was given between adequate and marginal scores.
CD4, cluster of differentiation 4; HIV, human immunodeficiency virus; HL, health literacy.
Other sources
Regarding non-internet information sources, AYAs reported high usage rates of school-based sources (Table 2). 40 AYAs' used media sources (including newspapers, magazines, TV, and radio) at similar rates to the internet, and rated these sources as similarly easy to understand. 54 Mixed findings emerged regarding the relationship between information source used and health literacy. While one study found that more health-literate AYAs reported spending more time reading health information “offline,” 41 another study found no association between health literacy and health-related information sources. 40
RQ2: How well are AYAs able to understand, communicate, and critically evaluate the information available to them?
Functional literacy
Twelve studies measured health literacy, and “adequate” health literacy was variously defined (Table 2). All of the studies using validated measures of health literacy reported adequate health literacy in at least 60% of participants (Table 1),41–46,48 and in more than 90% of AYAs in four studies.42,43,45,46 The high prevalence of adequate health literacy was reported, despite low numeracy/literacy skills in several studies among both healthy AYAs and those with HIV.39,41,43,47 One study noted that low numeracy resulted in poorer analytical skills. 47
Communicative literacy
No studies explicitly examined processes related to how AYAs communicated about health information with healthcare professionals.
Critical literacy
Two studies examined the more complex skills relevant to critical literacy. One of these found that while AYAs with HIV were able to appreciate their disease status, only 60% understood the potential implications of their disease, and 9% made final treatment decisions that were logically inconsistent with their expressed understanding/reasoning about their disease (e.g., did not want to take treatment, despite feeling better on medication). 50 The other study among healthy AYAs found that those with poor numeracy skills were more likely to find searching for health information frustrating, and were unsure of how to assess the quality of any information obtained. 47
RQ3: Is higher health literacy associated with health-promoting behaviors in AYAs?
Eight articles examined the link between health literacy and health behaviors (Table 2). Despite the disparate nature of the behavioral outcomes examined, some common themes emerged. Lower health literacy scores were associated with poorer health behaviors across several outcomes, including obesity,40,49 smoking, 40 and self-reported nutrition behaviors. 42 Contrary to this, however, one study highlighted that AYA men classified as “at risk” substance users were more likely to be well-informed and knowledgeable about the risks of the substance relative to abstainers. 54 Neither of the studies examining self-reported physical activity among healthy AYAs reported a significant link with health literacy.40,42
All of the studies examining the relationship between health literacy and treatment adherence were conducted among AYAs with HIV, and the emerging data were mixed. Two studies found greater medication adherence among AYAs who had a better understanding of their disease, although the authors suggested this was due to parental influence.50,51 Self-reported adherence was associated with functional (i.e., literacy and numeracy) skills but not with overall health literacy in another study. 41 However, in another study, no associations were found between health literacy, adherence, and actual disease/health status. 44
Discussion
This review provides a systematic update of the recent literature on health literacy among AYAs with and without chronic illness. Despite various illness-specific experiences, AYAs with various chronic illnesses such as asthma, diabetes, and cancer experience similar psychosocial concerns and challenges within the healthcare system due to their developmental stage. 32 AYA cancer survivors are at increased risks of late effects, such as cardiovascular disease and hypertension, that require ongoing surveillance, highlighting a particular need for health literacy in this population. 55
Across studies, AYAs reported using multiple sources of health information, including the internet and school-based information, and other media such as magazines and TV. The internet was mentioned as the most prominent source of health information used by AYAs across several studies, with most AYAs describing internet-based information as easy to understand. No clear relationship between the types of health information used and AYAs' health literacy could be discerned from the present review. Given that AYAs spend increasing time on the internet,33,56 further rigorous research exploring the role of the internet and its relationship with AYAs' developing health literacy appear warranted to guide future resource development.
AYAs' health literacy levels were wide-ranging. Although most studies reported adequate health literacy in more than 60% of AYAs, estimates ranged between 52% and 99%. This finding is consistent with Sanders et al.'s earlier estimate that one in three AYAs had poor health literacy, 7 but is more optimistic than previously published data reporting that 30–60% of AYAs showed suboptimal health literacy.5,7 This observation should be considered as tentative, considering the comparatively small, selected samples reviewed here. This review also found relatively low levels of functional health literacy, despite adequate overall health literacy. By contrast, findings in the adult literature suggest that only 10–20% show inadequate functional health literacy skills.57,58
Theoretical models have suggested that basic reading literacy and numeracy skills form the foundation on which higher-order skills, such as communicative health literacy and the capacity to evaluate health information critically, are built. 3 The mismatch between functional skills and overall health literacy observed in several studies here appears inconsistent with this theory. It is likely, as has been previously suggested,7,59,60 that the most frequently used health literacy measures are overly simplistic, and may not adequately reflect the spectrum of real-world skills that need to be harnessed for an individual to navigate the healthcare system effectively. Alternatively, it is possible that among AYAs with chronic illness, early and repeated exposure to the healthcare system could compensate for poorer functional literacy. 41 Future research to clarify the relationship between AYAs' foundational health literacy skills and real-world interactions with the health system are likely to shed light on this hypothesis.
The few studies available indicated that AYAs may have difficulties critically evaluating health information, despite adequate knowledge-based understanding. The paucity of studies examining higher-level health literacy prevents clear conclusions from being drawn. Due to their developmental stage, the social, communicative, and cognitive skills required to support these facets of health literacy are likely to be only emerging among many AYAs.15,16,61 Currently available, validated health literacy tools may also be inadequate for capturing these navigational and interaction-based processes.7,59,60 Future studies documenting how AYAs engage with and act upon health information are needed in order to conceptualize better the strengths and challenges that AYAs may be likely to face in interacting with health systems in the real world.
More research was available that answered the important question of how AYAs' health literacy skills may be related to their health behaviors. Lower health literacy was related to poorer health behaviors across several outcomes, as shown across adult findings8–10 and Sanders et al.'s review. 7 However, also in line with adult studies documenting either no or weak associations between health literacy and adherence, mixed findings emerged regarding medication adherence.62–64 All but one study in this review assessed self-reported adherence, however, which is acknowledged as a methodologically questionable measure. 65 Commonalities across studies between healthy literacy and health outcomes, including smoking, obesity, and poor nutrition, were found. In contrast, Sanders et al. 7 reported a strong association between general literacy skills (measured by reading grade levels) and health behaviors, including substance abuse and acquisition of sexually transmissible illnesses. These mixed findings highlight the complexities involved in translating information understanding to the enactment of positive health behaviors.
Future directions
This review has revealed several gaps in the literature. Future studies need to consider the role of the internet as a source of health information, the unique developmental stage of AYAs, the social and familial context of AYAs, and the process of developing health literacy. Little research exists regarding AYA health literacy, especially in chronic illnesses. Future research should consider utilizing existing large-scale AYA cohort studies (e.g., through the U.S. National Cancer Institute and National Adolescent and Young Adult Health Information Center)66,67 in order to assess health literacy.
AYAs have been described as “digital natives,” 68 who are exceptionally computer and internet literate, and report using the internet to meet a range of health informational and supportive care needs.33,69 This review highlighted emerging support for the role of the internet as a source of health information, though gaps remain in our understanding of the extent to which different AYA groups use the internet and whether this has the potential to support the development of health literacy. Online tools and resources have the potential to increase the reach of health services and interventions to otherwise underserved populations.70,71 AYA-targeted internet-based interventions hold promise for providing appropriate health information and assisting in the development of health literacy. Future research should also address perceived versus actual validity of health information online.
Organizations such as the Health on the Net Foundation 72 and National Network of Libraries of Medicine 73 have recently provided a list of websites that they consider to be valid and reliable. Future recommendations for practitioners include promoting such websites, or a list of vetted websites with AYA-specific health information. In addition, practitioners should ensure that they provide support to young people, as well as provide information in an AYA-appropriate way.
There also appear to be considerable gaps in understanding how current health literacy models 3 interact with adolescents' normal development. 14 The paucity of research examining higher-level communicative and critical literacy skills indicates that more complex, navigational processes remain poorly understood, despite the fact that these components are likely to be the most challenging, and critical, to target in interventions. Nutbeam's model of health literacy maps on to the trajectory of AYA development. An upward transition of health literacy from basic functional literacy to higher-level critical analysis of information coincides with AYAs' own advancing social and cognitive development. Nutbeam proposed that health education may play a vital role in assisting an individual to progress through each step of health literacy. 3 The modest number of articles included in this review limits the capacity to propose a health education plan based on the present data. However, it would be worthwhile for future research to consider how health-related education could be harnessed during the AYA years to aid the development of higher-level critical health literacy. More in-depth qualitative research with AYAs may also assist in this endeavor by exploring and identifying mechanisms underpinning poor health literacy. Current measures used within the field focus on assessing health literacy in terms of basic, functional skills often categorizing health literacy in a binary adequate/inadequate capacity.7,59,60 The use of only brief measures indexing health literacy is a shortcoming of the field that has been previously noted.7,59,60 Tools to assess health literacy in AYAs with cancer have recently been reported. 74 However, future work is needed to develop new methodologies for assessing health literacy levels in practice. This review has focused on AYAs' health literacy at an individual level. Future work may extend upon this by considering how best to capture AYAs' social environment and exposure to various social determinants of health in order to enable a more grounded, real-world conceptualization of AYAs' health literacy as it exists in practice.
As noted by Sanders et al., 7 it is also critical that future studies examining AYAs' health literacy consider the “collective health literacy” skills of key individuals involved in their care and support, such as parents, family members, and teachers, with qualitative studies highlighting the important role that parents and caregivers continue to play for AYAs with chronic illness. 61 Understanding how AYAs' health literacy skills develop over time both over the course of an illness trajectory and as they take increasing responsibility over their health management will be critical. Conceptualizing the development of these skills within AYAs' social- and illness-related context will contribute to the development of age-appropriate health systems, including transitional processes to assist AYAs to move successfully to adult healthcare systems.17,20,21
Given that some AYAs appear health literate, it would be useful for future research to examine the factors and processes that are important in developing health literacy. The development of health literacy skills and how they can be supported as AYAs mature over time remains an important question for youth-friendly health services to understand.
Strengths and limitations
This review synthesized recent data on health literacy among AYAs with and without chronic illness, extending past reviews by systematically examining functional, communicative, and critical components of AYAs' health literacy skills. 3 Due to the recent focus on the AYA population within health settings, 32 and the growing role of online health information, this review provides a more relevant overview of health literacy for AYAs. It also complements and extends upon Sanders et al.'s review 7 by providing the available literature on health literacy in AYAs with a chronic illness, a population in greater need of adequate health literacy.
The present findings should be considered in reference to a few limitations. In many ways, the included articles were disparate in their target age ranges, populations, measured outcomes, and mode of recruitment. The lack of health literacy research in AYAs (leading to a modest sample size included here and inability for further meta-analysis) limits the ability to synthesize across groups and also with Sanders et al.'s review. 7 However, the reviewed articles were consistent in their reliance on adult measures of health literacy and their focus on health literacy as a binary (adequate/inadequate), individual-level skill, and being largely U.S.-based in origin. The current conceptualizations and measures of health literacy therefore may be inadequate to capture health literacy among AYAs both with and without chronic illness.
An additional limitation is the difficulty defining the AYA range. 75 Due to the minimal research on AYA health literacy, all articles addressing AYA populations, regardless of their definition, were included. This resulted in two articles being included with some participant ages extending outside of the authors' definition,39,43 which may limit the relevance of the findings of this review.
Most of the reviewed studies included in the analysis used standardized and validated measures developed for adult populations (e.g., TOFHLA). Given the uniqueness of AYAs in their cognitive and social development, the use of adult measures may limit the findings of reviews included. Only articles published in English were included in the analysis, which may have reduced the cultural relevance of the findings. The majority of studies recruited AYAs with a chronic illness from multidisciplinary, primary-care clinics, which may have potentially skewed results. All 14 studies also suffered from a lack of control groups and cross-sectional designs, which has limited the interpretability of results.
The inclusion of only quantitative data may have also limited the ability to capture AYAs' experience of health literacy by excluded studies exploring some of the more “real world” process-based aspects of health literacy, or excluding studies exploring AYAs' experiences in communication and interacting with healthcare professionals.
Conclusion
Tailoring health services to be developmentally appropriate for AYAs is a critical goal to support the health of young people on the cusp of adulthood. This review points to the need to conceptualize the development of health literacy skills among AYAs within their developmental and social context over time. The recent data examined here indicate that although many AYAs may have adequate health literacy, nearly half may not, and this appears linked with poorer health behaviors in some domains. For AYAs with a chronic illness such as cancer, health literacy becomes even more important when young people are beginning to take on more autonomy and responsibility regarding their health behaviors. Ensuring AYAs with chronic illnesses have adequate health literacy may reduce their risks of developing medical complications later in life. The present data have important public health implications, given the potential cost and impact of future years of poor health that may be experienced by young people both with and without chronic illness. With the paucity of information regarding health literacy in AYAs with cancer, this review also provides insight into improving health literacy for this vulnerable population.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Mona Sajeev (Behavioural Sciences Unit, Kids Cancer Centre, Sydney Children's Hospital and UNSW Medicine, University of New South Wales, Australia) to early data screening and article selection processes involved in this review. This contribution was not financially compensated. Ursula Sansom-Daly is supported by an Early Career Fellowship from the Cancer Institute NSW (ID: 14/ECF/1-11) and an Early Career Fellowship from the National Health and Medical Research Council of Australia (APP1111800). Claire Wakefield is supported by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1067501) and an Early Career Development fellowship from the Cancer Institute NSW (ID: 11/ECF/3-43). Afaf Girgis is funded through a Cancer Institute NSW grant. The Behavioural Sciences Unit is supported by the Kids with Cancer Foundation. The Cancer Institute NSW, the National Health and Medical Research Council of Australia, and the Kids with Cancer Foundation did not play any role in the design and conduct of the study; data collection, management, analysis, or interpretation; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.