
Abstract
Glassy cell carcinoma of the cervix (GCCC) is a very rare and aggressive form of cervical cancer. An adolescent female with advanced metastatic disease was enrolled in our genomic profiling research protocol. We identified high-level amplification of epidermal growth factor receptor (EGFR) and Yes-associated protein-1 (YAP1), which led to the addition of EGFR inhibitors to the chemotherapy regimen. Here, we report the first genetically profiled case of GCCC with potential therapeutic implications.
Introduction and Literature Review
G
Due to its rarity and lethality, GCCC is a severely understudied malignancy and the molecular drivers of this disease are yet to be identified. As part of our ongoing precision medicine clinical research protocol, we performed whole-genome DNA sequencing and RNA sequencing on a 16-year-old female patient diagnosed with stage IVB T3b N1 M1 GCCC. DNA sequencing revealed focal high-level amplifications encompassing epidermal growth factor receptor (EGFR), Yes-associated protein-1 (YAP1), as well as a cluster of matrix metalloproteinases (MMPs). To date, this is the only report of such an in-depth analysis of this disease.
Materials and Methods
Patient accrual
Informed consent was obtained to enroll the patient in our clinical genomics research program. Biopsy material and matched normal tissue (blood) were collected and processed for DNA extraction according to research protocol 111199. This study was approved by the Institutional Review Board at Children's Hospital of Orange County (CHOC).
Next-generation sequencing
Whole-genome sequencing was performed using paired-end sequencing. Nucleic acids from both freshly procured tumor tissue and matched normal (blood) tissue were submitted to the Illumina Clinical Services Laboratory for TruGenome Technical Sequence Data service. Library preparation and sequencing were performed in accordance with the Clinical Laboratory Improvement Amendments (CLIA) and College of American Pathologists (CAP) standards. The tumor DNA was sequenced to a depth of 123× and the constitutional germline blood sample was sequenced to 33×.
RNA was extracted from pre-treatment and post-treatment formalin-fixed paraffin-embedded (FFPE) tissue using the Qiagen AllPrep FFPE Kit. Sequencing libraries were generated using the Illumina TruSeq RNA Access Library Prep Kit and run on a HiSeq2500 instrument (Illumina).
Bioinformatic analysis
The DNA and RNA sequencing data were analyzed using a customized bioinformatic pipeline and contextually interpreted. DNA copy number alterations were visualized using Nexus Copy Number version 7.5 (BioDiscovery). RNA reads were aligned and assembled using Cufflinks, and differential expression was performed using Cuffdiff. Genes with fragments per kilobase of exon per million fragments mapped (FPKM) values <2 were omitted from downstream analysis. Gene set enrichment maps were generated using Cytoscape version 3.2.1. Pathway analysis and predictions were generated using Ingenuity Pathway Analysis.
Immunohistochemistry
Diagnostic staining for EGFR was performed by Clarient Pathology Services, Inc. Additional immunohistochemistry was performed by TGen. The FFPE research samples were deparaffinized, rehydrated, and antigen retrieved, using heat-induced epitope retrieval in citric acid-based buffer, pH 6. The samples were peroxidase quenched, blocked, and incubated with antibodies against phosphorylated EGFR (at#M7299; Dako) and YAP1 (cat#14074; Cell Signaling Technology). 3,3-diaminobenzidine (DAB) and Nova Red were used as peroxidase substrates (Vector Laboratories).
Results
Clinical Presentation
A 16-year-old previously healthy African American female was diagnosed and treated initially for pelvic inflammatory disease. Symptoms included worsening difficulty urinating, decreased urine production, constipation, intermittent vaginal bleeding, and bilateral swelling of the lower extremities. Subsequently, the patient presented at the local emergency department with abnormal electrolyte and blood gas values, kidney dysfunction, anemia, hypotension, and tachycardia. An abdominal computerized tomography (CT) scan revealed a large lower uterine/cervical mass and severe bilateral hydronephrosis. The patient was stabilized with four units of packed red blood cells, tranexamic acid, bicarbonate, and dialysis and then transferred to CHOC Children’s Hospital.
Chest CT scans without contrast revealed posterior subsegmental areas of suspected infiltration and a subpleural right-sided nodular mass, possibly representative of metastatic disease. Abdominal CT scans without contrast showed enlarged bilateral iliac lymph nodes and a central uterine mass (Fig. 1A, B). Subsequent positron emission tomography (PET)/CT scans demonstrated a large lower uterine/cervical mass with extensive abnormal hypermetabolism with a maximum standard uptake value of 11 (right) and 8 (left) (Fig. 1C). Additional multifocal areas of abnormal hypermetabolism were seen in the bones, bilateral lower lung lobes (Fig. 1D), pancreas, and multiple lymph nodes.
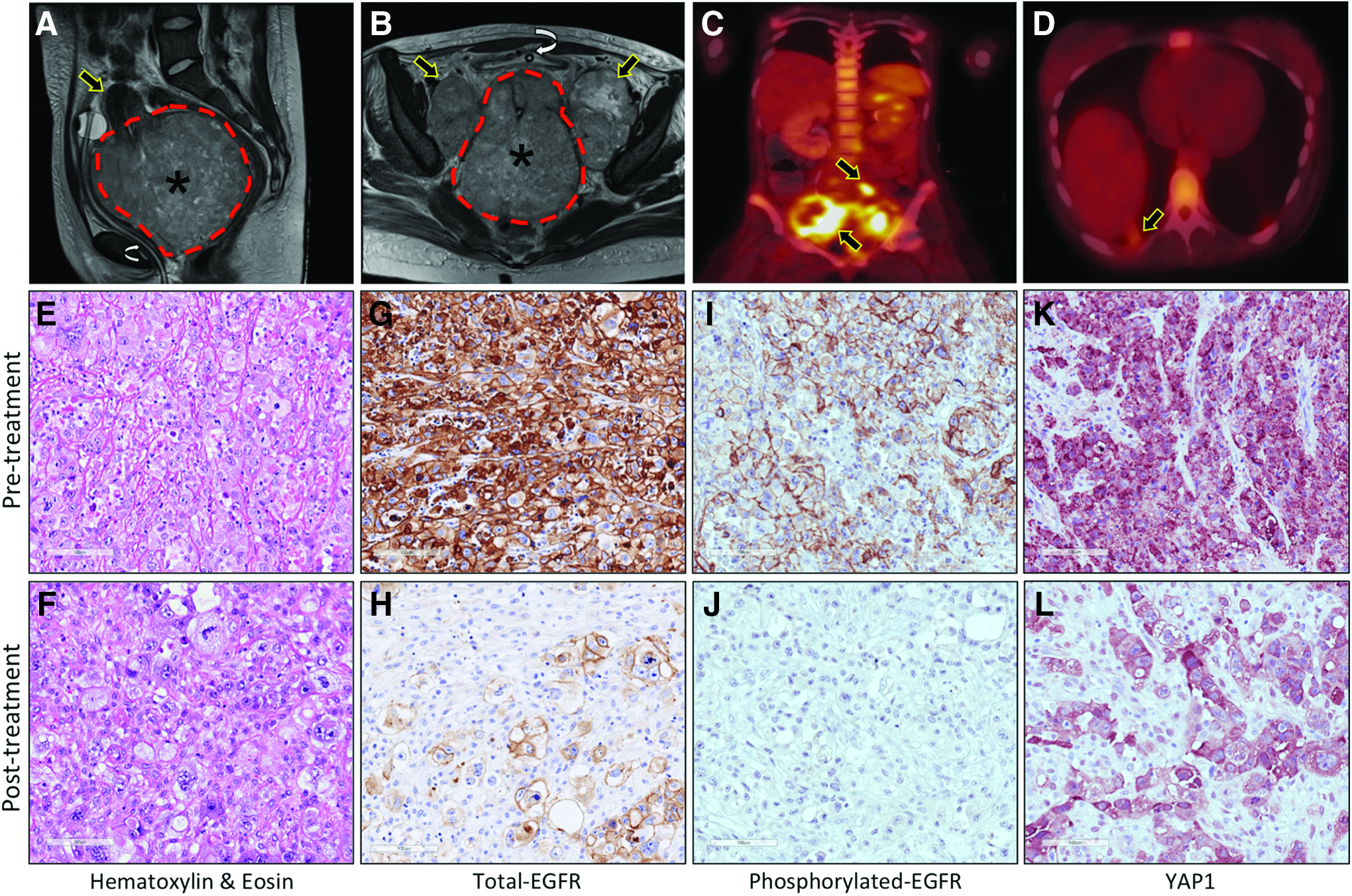
Radiological and histological analysis of GCCC.
Histological assessment of the tissue was suggestive of GCCC (Fig. 1E, F). Immunohistochemical staining of the biopsy demonstrated immunoreactivity for keratin, high- and low-molecular-weight cytokeratin, p16, p63, PAX-8, and scattered immunoreactivity for p53 (data not shown). In contrast, the patient was negative for GATA3, WT1, HER-2/Neu, and human papilloma virus. Cytogenetic analysis of the tumor tissue revealed an abnormal female tissue karyotype with a modal range of 76–82 chromosomes. The combined radiology and histopathology data warranted a diagnosis of stage IVB T3b N1 M1 GCCC.
Radiation and chemotherapy regimen
Therapeutic intervention included the emergent administration of a total of 12 Gy of pelvic radiation over three consecutive days followed by paclitaxel and carboplatin. 4 The carboplatin dose was increased with improved kidney function. The patient received two courses of paclitaxel/carboplatin, given 3 weeks apart. Follow-up CT scans demonstrated a minimal response to therapy. New adenopathy was noted between the spleen and the left lobe of the liver. Omental nodules were also observed. Subsequent CT scans suggested no change in the uterine/cervical mass nor a reduction in size of the bilateral iliac lymph nodes concomitant with the emergence of new peritoneal nodules suggestive of carcinomatosis. These masses were deemed unresectable. Accordingly, the patient's treatment plan was modified to intravenous paclitaxel, cisplatin, and bevacizumab, according to the recurrent metastatic cervical cancer protocol. 5 The patient developed severe neuropathy associated with platinum-based chemotherapeutics and was treated with gabapentin and morphine. The patient received a single dose of cisplatin due to severe exacerbation of neuropathy and declining kidney function. At this point, the molecular profiling data became available.
Discovery of an EGFR amplification and subsequent therapeutic targeting
Whole-genome DNA sequencing of the initial biopsied tissue revealed numerous somatic genetic alterations, including copy number alterations, nonsynonymous coding variants, and structural chromosomal aberrations (Fig. 2A). Notably, high-level amplifications encoding EGFR on chromosome 7p11.2 (Fig. 2B), YAP1 and platelet-derived growth factor-D (PDGFD) on chromosome 11q22 (Fig. 2C), and a low-level amplification of Janus kinase-2 (JAK2) on chromosome 9p24.1 were observed. Multiple MMP genes were also present in the 11q22.1 amplicon (Fig. 2C).
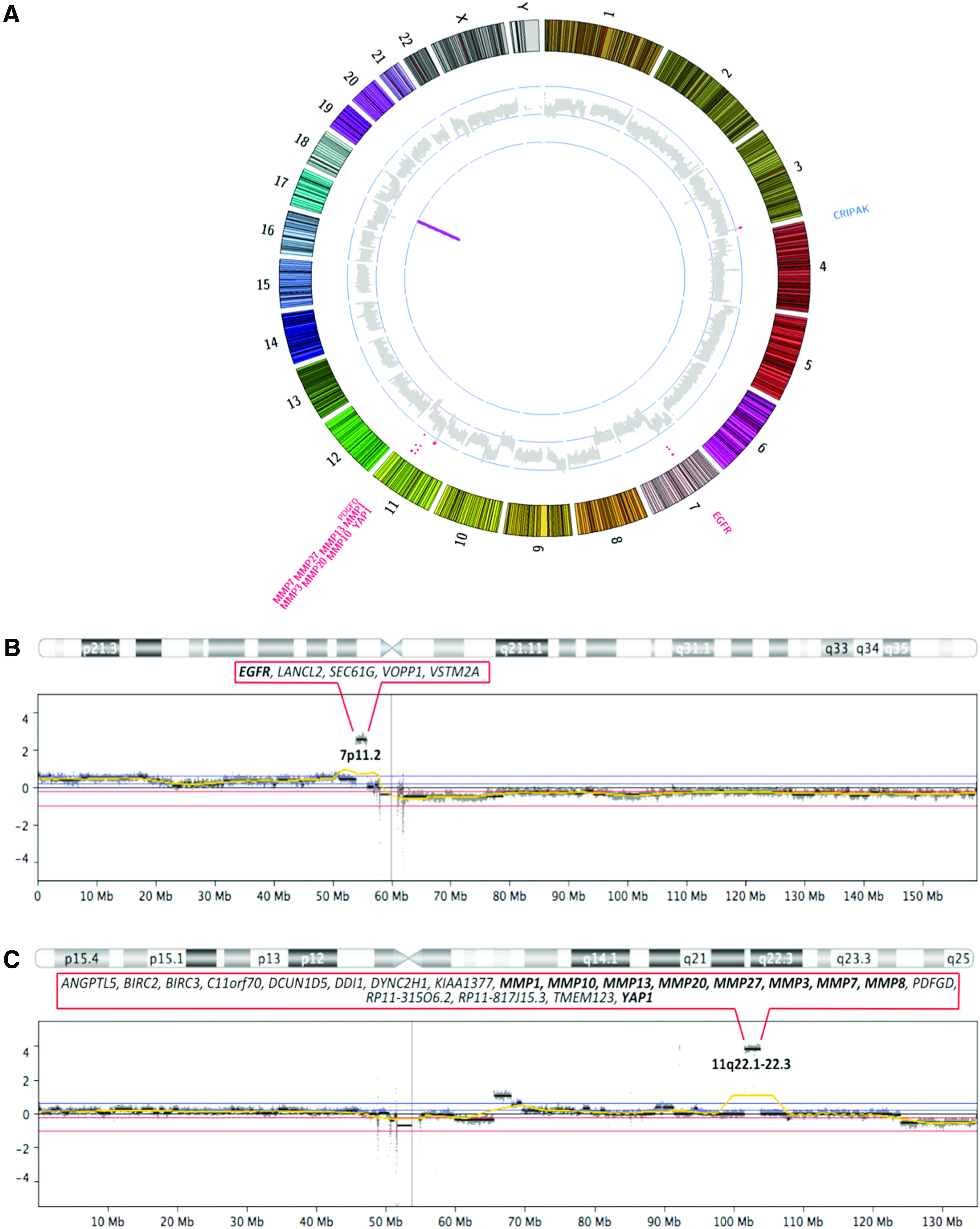
Genomic profile of GCCC.
Given the molecular profiling data, the patient's treatment plan was amended to include the administration of the EGFR inhibitors cetuximab and erlotinib in addition to paclitaxel and bevacizumab (modified from Pignata et al). 6 On days 8 and 15 of this regimen, carboplatin was added because of her lessening neuropathy and increased kidney function. Shortly after receiving day 15 of the revised regimen, the patient developed bowel obstruction. While abdominal and pelvic CT scans revealed multiple dilated bowel loops and worsening carcinomatosis, decreased volume of the central pelvic mass and the bilateral iliac nodes was observed (Fig. 3A). The patient underwent laparotomy with adhesiolysis. Omental, peritoneal, and mesenteric metastatic nodules were observed and a subsequent biopsy of the omental lesion confirmed metastatic GCCC. This tissue was used for further molecular analysis. During this procedure, the bowel obstruction was relieved and decompressed. The patient was unable to continue further therapy due to complications associated with significant disease burden. At this point, the patient was deemed terminal and approached for palliative care.
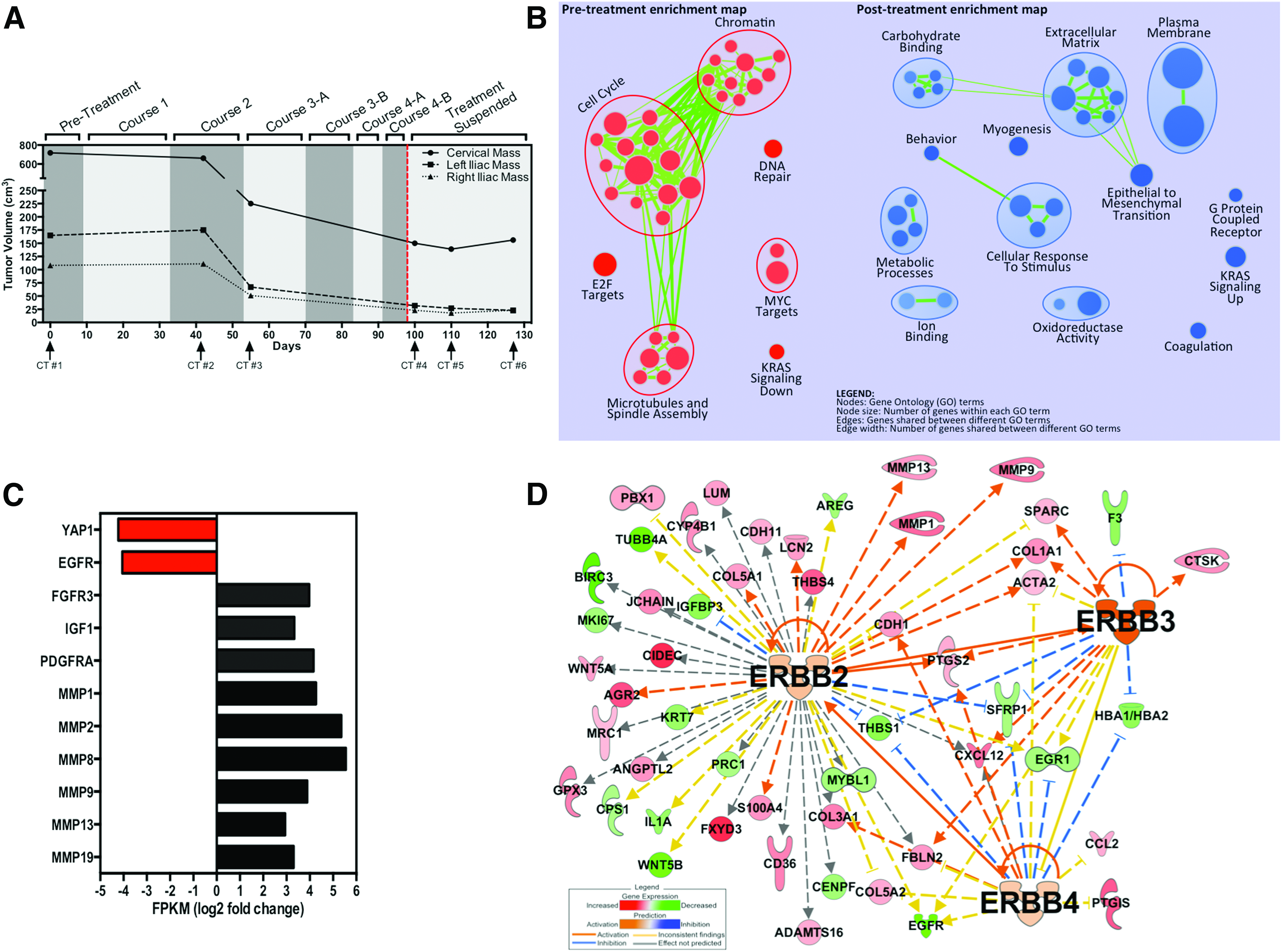
Radiological and molecular response to chemotherapy.
Post-treatment analysis reveals inhibition of EGFR
Inhibition of EGFR was evidenced by decreased immunoreactivity of both total and phosphorylated-EGFR in the post-treatment omental lesion versus the untreated initial biopsy tissue (Fig. 1G, J). A reduction in YAP1 immunoreactivity in the post-treatment tissue was also observed (Fig. 1K, L). In addition, EGFR and YAP1 mRNA levels were decreased in the post-treatment omental lesion in comparison to the treatment-naive biopsy tissue (Fig. 3B). Increased expression of FGFR3, IGF1, PDGFRA, MMP1, MMP2, MMP8, MMP9, MMP13, and MMP19 was observed in the post-treatment sample (Fig. 3B).
Gene ontology analysis indicated that the post-treatment omental tissue displayed a more mesenchymal and invasive phenotype than the primary tumor sample (Fig. 3C). This was accompanied by a predicted increase in ERRB2, ERBB3, and ERBB4 pathway utilization (Fig. 3D) in the post-treatment tissue.
Discussion
We describe an adolescent patient with late-stage metastatic GCCC. This report is the first to utilize next-generation sequencing technology to determine the molecular genetic drivers of this rare and aggressive disease. Furthermore, we demonstrate the possible therapeutic utility of this approach in its ability to elucidate an actionable target in a clinically relevant time frame. Due to the low incidence rate and limited number of published reports, a void remains with regard to the genetic aberrations and molecular mechanisms associated with GCCC. Likewise, in the era of molecularly targeted therapies, this absence of knowledge is detrimental to patients with advanced stage of this disease where standard chemotherapy and radiation have proven ineffective.
The identification of high-level amplification of EGFR reported here is in agreement with the expression of EGFR in 18% of GCCC patients through immunohistochemistry. 7 The concomitant amplification of YAP1, a recently validated oncogene that is amplified in a variety of cancers, including cervical cancer, is also of clinical significance for this patient.8–11 YAP1 is associated with resistance to cetuximab in both colorectal cancer and head and neck cancers.12,13 Despite the genomic complexity of this tumor, these specific amplifications were considered the driver mutations of the malignancy. The combined use of both cetuximab and erlotinib has demonstrated increased efficacy in patients with nonsmall-cell lung cancer and advanced refractory colorectal cancer.14,15 Moreover, the administration of both agents in combination may circumvent the potential cetuximab resistance attributed to YAP1, as evidenced by the decrease in YAP1 mRNA and protein expression in this patient after treatment.
Interestingly, increased mRNA expression of FGFR3, PDGRA, IGF1, MMP1, MMP2, MMP8, MMP9, MMP13, and MMP19 was observed in the post-treatment omental lesion, suggesting the adoption of a more mesenchymal phenotype. In fact, gene set enrichment analysis demonstrated a significant enrichment of genes associated with epithelial to mesenchymal transition (EMT) in the post-treatment omental lesion. EMT is a known means of chemoresistance and it has been demonstrated that the acquisition of the mesenchymal phenotype is responsible for gefitinib resistance in head and neck squamous cell carcinoma cells.16–18
In addition, gene expression analysis predicted the utilization of ERBB2, ERBB3, and ERBB4, members of the human EGFR family. Increased Erb-B pathway activation has been associated with resistance to erlotinib and cetuximab.19–21 This suggests that EGFR inhibition results in the utilization of alternative heterodimeric receptor complexes comprising other HER family members to circumvent the EGFR-based therapy. Taken together, these data are suggestive of potential mechanisms underlying the aggressive progression of this metastatic disease despite the observed primary tumor shrinkage in response to the multimodal treatment regimen.
This report highlights the molecular genetic basis of an extremely rare disease and represents the first case of GCCC treated at CHOC Children's Hospital. We cannot determine if the observed responses were due to the chemotherapy alone or if these responses were enhanced by EGFR inhibition. Furthermore, there are no studies reporting the ability of EGFR inhibition to modulate the effects of paclitaxel and carboplatin. Although these findings may not be representative or applicable to other GCCC cases, the identification of EGFR and YAP1 amplifications is important in attempting to understand the disease in this specific patient. Thus, molecular genetic profiling of additional GCCC cases is needed to validate the findings presented here. If confirmed, these data may represent a new potential therapeutic option for patients with GCCC, especially in the early stages of disease when the tumor burden is not as extensive.
Footnotes
Acknowledgment
This work was supported by a grant from Hyundai Motor American and Hyundai Hope on Wheels.
Author Disclosure Statement
No competing financial interests exist.