
Abstract
Purpose:
Few studies have addressed the adaptive mental health status of young adult (YA) survivors of childhood cancer (SCCs) and the siblings (SIBs) of the same families. This article explores the existence of different psychological well-being (PWB) profiles and verifies their relationship with life satisfaction, resilience, and mental adjustment among Italian YA survivors of childhood leukemia or lymphoma and their own SIBs.
Methods:
YA SCCs (n = 35) who had been off primary treatment for at least 5 years and their SIBs (n = 47) completed anonymous self-report questionnaires for PWB, life satisfaction, resilience, and mental adjustment. The survivors at the time of the survey had an average age of 27 years (SD 3.37) and they were an average age of 12 years (SD 1.93) at diagnosis. Their own SIBs had an average age of 29 years (SD ±5.25).
Results:
No significant differences were found between SCCs and their SIBs in all considered dimensions. Only 12% of the sample showed evidence of clinically significant mental health disorders, 51% manifested medium levels of resilience, and 49% fit a functional PWB profile. By means of cluster analysis, three PWB statuses could be derived: self-devaluing (25.5%), fatalist (25.5%), and eudaimonic (49%). Each of these PWB statuses exhibited a significant distinct profile in terms of life satisfaction, resilience, and mental adjustment.
Conclusions:
There is a need to establish psychosocial services that offer follow-up examinations aimed to not only prevent mental disorders but also to promote PWB.
Introduction
A
SCCs may have late effects from treatments, which can reduce quality of life. The family, as a unit, survives cancer with the patient and therefore the family members are considered to be second-order survivors.7,8 Recently, researchers have highlighted that siblings (SIBs) of cancer patients experience relevant psychological struggles such as negative emotional reactions and poor quality of life in emotional, family, and social domains.9,10
For YA SCCs and their SIBs, there is an important identity transformation that occurs in transitioning from active treatment to survivorship. Studies of the transition experience from patient to survivor have found that survivors have an extremely difficult time returning to their normal lives and recovering their identities. 11
However, limited research has focused on the long-term psychosocial adjustment of YA SCCs and their SIBs. Furthermore, the majority of existing studies have highlighted two main limitations: (1) they used an impairment model of adjustment12,13 and (2) they were predominantly variable oriented.
The impairment model defined well-being as the absence of diagnosed psychological disorders or limitations in physical functioning. 14 These studies showed that in general, survivors did not report substantially different frequencies of emotional problems than did the comparison groups without a cancer history.15,16 Nevertheless, the current YA psycho-oncology research17–19 has directed its attention toward a multidimensional and thriving model of adjustment 12 that assesses happiness, life satisfaction, and level of functioning in multiple domains. Indeed, some qualitative researches 18 highlighted that SCCs reported as positive late effects closer relationship with their family20,21 and increased faith. 22 In another interesting study emerged increased hope, personal growth, existential perspective, healthy living, and new strength. 23
One of the most recognized models in the thriving field is the multidimensional model of Carol Ryff and Core Keyes, 24 which defined psychological well-being (PWB) as the presence of six distinct dimensions: autonomy, environmental mastery, personal growth, positive relationships with others, purpose in life, and self-acceptance. From this perspective, PWB is more than adjustment. 25 The studies and interventions in this field highlighted that PWB is quantifiable and linked to better physical health, lower disease rates, decreased disability, and reduced early mortality rates through optimal regulation of multiple neurological and physiological systems. 26 Furthermore, because previous studies of YA survivors were variable oriented, they neglected the personal approach aimed to identify a well-being typology and profile that is more coherent with a multidimensional view of well-being. 27 The general aim of the present study was to explore the level of PWB, life satisfaction, and resilience, as well as adjustment, in a group of YA SCCs and their SIBs. More specifically, the purpose was to explore the existence of different PWB profiles and to verify their relationship with life satisfaction, resilience, and adjustment. Comparisons with SIBs have the advantage of minimizing the bias through the similarity of family environment and certain aspects of genetic factors. 28
Methods
Participants and procedure
With approval from the institutional ethics review board, the recruitment of survivors and their SIBs relied on the Pediatric Clinic of the University of Milano Bicocca, Monza and Brianza Foundation for the child and his/her mother (MBBM) in Lombardy, San Gerardo Hospital, Italy. It is one of the most important centers of pediatric hematology in northern Italy.
Originally, the Pediatric Clinic consulted the medical charts related to the adolescents who received a diagnosis of leukemia or lymphoma between the 1998 and 2003. Survivors who had received grafts or had relapsed were excluded. The Pediatric Clinic compiled a list of 39 eligible SCCs who were YAs and had been off primary treatment for at least 5 years at the time of the survey. The principal researcher (S.M.) mailed questionnaires to each of the qualified survivors and to the SIBs of the same families. It was required that the survivors and their own SIBs independently complete the questionnaires. All participants were informed of the aim, the objectives, and the methods of the study. A stamped addressed envelope was provided with each questionnaire.
Measures
Psychological well-being
Participants completed the Italian version 29 of the PWB Scale, 24 which is a self-rating 18-item inventory that covers six areas of well-being: autonomy, environmental mastery, personal growth, positive relationships with others, purpose in life, and self-acceptance. Participants respond using a six-point format that ranges from strongly disagree to strongly agree. High scores indicate a high self-rating on the dimension assessed. Cronbach's alpha of the total score was 0.77. Cronbach's alpha of subscales ranged from 0.49 to 0.60.
Life satisfaction
Participants completed the Satisfaction with Life Scale (SWLS), 30 which is a short five-item instrument designed to measure global cognitive judgments of satisfaction with one's life. Participants respond using a seven-point format that ranges from strongly disagree to strongly agree. Scores ranging from 30 to 35 indicate highly satisfied, 25 to 29 indicate satisfied, 20 to 24 indicate moderately satisfied, 15 to 19 indicate slightly dissatisfied, 10 to 14 indicate dissatisfied, and 5 to 9 indicate extremely dissatisfied. Cronbach's alpha was 0.85.
Resilience
Participants completed the Italian version of the General Self-efficacy Scale (GSE), 31 which is a short 10-item instrument designed to measure one's sense of personal competence in managing challenging problems and difficulties. Cronbach's alpha was 0.86.
Participants respond using a four-point format that ranges from strongly disagree to strongly agree.
The Italian version was standardized for the AYA population. A score lower than 27 means low resilience (0–30 percentile), a score ranging from 27 to 30 means a medium level of resilience (31–60 percentile), and a score higher than 60 means a high level of resilience (61–100 percentile).
Adjustment
Participants completed the Italian version 32 of the Symptom Checklist-90-R (SCL-90-R), 33 which is a 90-item self-report symptom checklist with nine symptom scales measuring common psychological problems and a widely used summary scale of overall distress, the Global Severity Index (GSI), which combines information on a number of symptoms and the intensity of distress. Each item is rated on a five-point scale of distress (0–4) from not at all to extremely. Case identification is based on Italian validated case rules developed for the SCL-90, 32 which defines a screening as positive if the GSI or any subscale T score is >63 (90th percentile). Participants with GSI elevations >63 were classified as having significant psychological maladjustment. Cronbach's alpha of the GSI was 0.98. Cronbach's alpha of subscales ranged from 0.76 to 0.92.
Statistical analyses
First, the normality of all the measures was tested by univariate skewness and kurtosis index. Consistent with Marcoulides and Hershberger, measures of both skewness and kurtosis index ranging from 1 to −1 were accepted as normally distributed.
The GLM multivariate analysis of variance (MANOVA) and chi-square test were performed to analyze possible differences in mean scores and the levels of each scale according to patient versus sibling and female versus male variables. The sample characteristics were analyzed with descriptive statistics.
Consistent with the study's aims, a person-centered approach was adopted.34–36 Specifically, a cluster analysis of the six dimensions of PWB was conducted using a two-step procedure. 37 In the first step, a hierarchical cluster analysis was performed using Ward's method based on squared Euclidian distances. In the second step, an iterative k-means clustering procedure was conducted to explore the existence of different PWB profiles. Bonferroni's post hoc analysis was then performed to detect differences in PWB profiles.
To examine whether PWB profiles reported meaningful differences in adjustment, life satisfaction, and resilience, a chi-square test was conducted between the PWB profiles emerging from the cluster analysis and the levels of GSI, SWLS, and GSE.
Version 22 of SPSS for Windows was used for all statistical analyses.
Results
Study sample
Thirty-five YA SCCs and their own 47 sisters and brothers responded within a data collection period of 4 months, thereby resulting in a response rate of 90%.
Table 1 shows the demographic characteristics of the SCCs and their own SIBs.
Preliminary mean-level analyses
All scales were normally distributed.
The GLM MANOVA revealed nonsignificant patient versus sibling and female versus male differences in the distribution of participants across the means of all six PWB dimensions, as well as levels of life satisfaction, resilience, and adjustment. Therefore, patients and SIBs were considered to be a single sample in later analyses.
Table 2 shows the descriptive statistics of all six PWB dimensions. Compared with the PWB mean scores of the healthy YA population, 29 the present SCCs and their SIBs scored lower in autonomy (p < 0.05) and self-acceptance (p < 0.000).
Only 12% of participants showed evidence of clinically significant psychological disorders, and only 15% were dissatisfied with life. The 51% manifested medium-high levels of resilience (Fig. 1). There were no significant differences in the distribution of SCCs versus SIBs across the levels of psychological disorders (χ2 = 2.40; df = 1; p = 0.12), of life satisfaction (χ2 = 3.1; df = 2; p = 0.21), and of resilience (χ2 = 0.05; df = 2; p = 0.97).
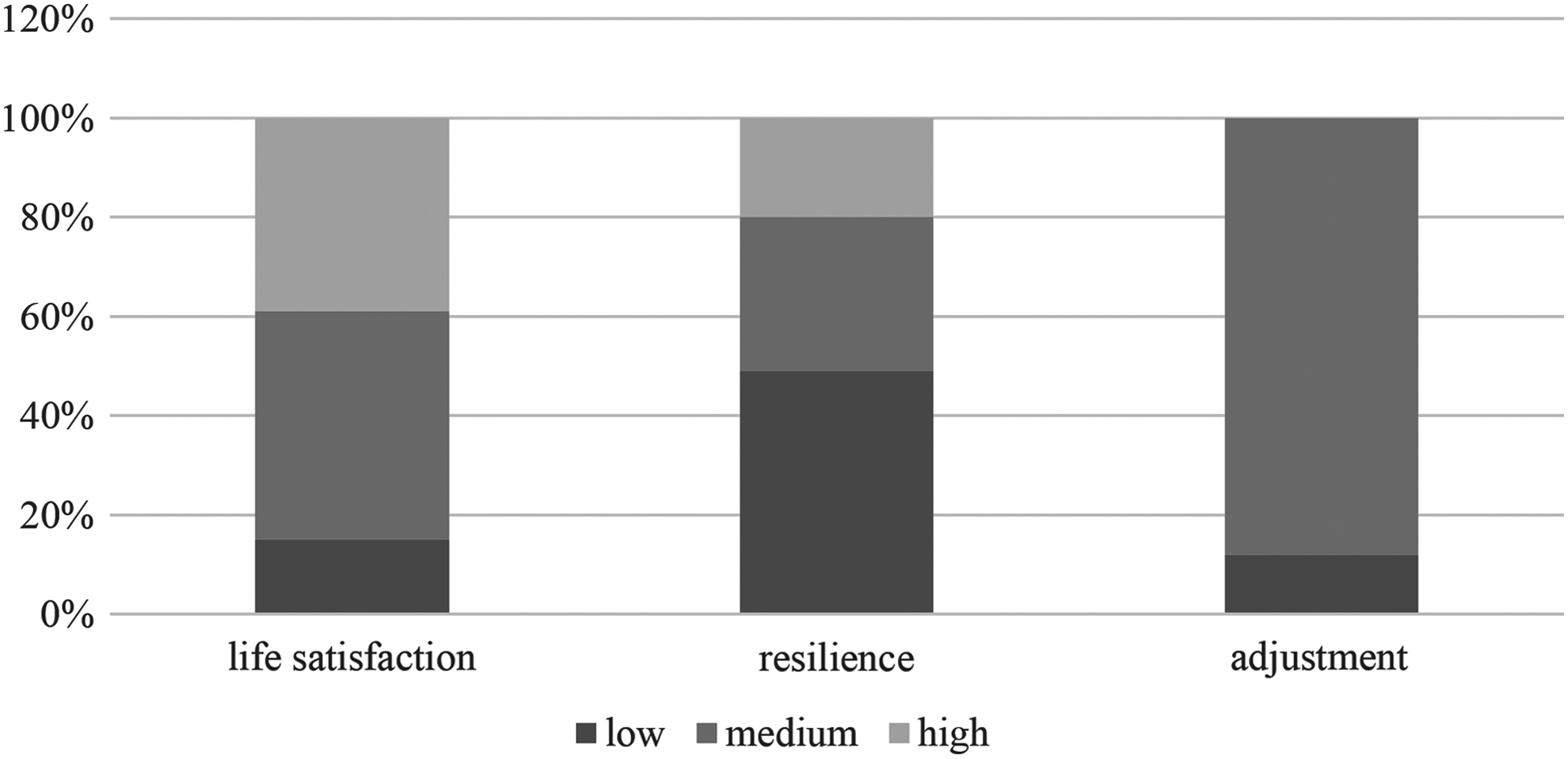
Frequencies of life satisfaction, resilience, and mental adjustment levels.
Cluster analysis
Univariate and multivariate outliers were sought before performing the cluster analysis because outliers can affect the results. 38 No such outliers were found. A cluster analysis of the six dimensions of PWB was performed, and two to four cluster solutions were evaluated in terms of substantive interpretability, parsimony, and explanatory power.
Cluster solution
As a result, three clusters were retained (Table 3). The cluster solution explained between 35% and 52% of the variance in the PWB dimensions (Wilk's Lambda = 0.11, F = 21.63, p < 0.000, η2 = 0.66). In the two- and four-cluster solutions, there were problems of interpretability and parsimony.
The chi-square test conducted to determine the effects of the distribution of participants across SCC versus SIB groups on cluster membership was nonsignificant (χ2 = 1.41; df = 2; p = 0.49). The cluster solution was reliable for both SCCs and SIBs; therefore, patients and SIBs were considered to be a single sample in later analyses.
The first cluster (Table 3), designated self-devaluing (25.5% of the sample), was characterized by low scores on autonomy, self-acceptance, and positive relationships (Z-scores ranged from −1.13 to −0.70) and by moderate-low scores on environmental mastery, purpose in life, and personal growth (Z-scores ranged from −0.47 to 0.04).
The second cluster (Table 3), designated fatalist (25.5% of the sample), was characterized by low scores on environmental mastery, personal growth, and purpose in life (Z-scores ranged from −1.08 to −0.61), by moderate-low scores on self-acceptance and positive relationships (Z-scores ranged from −31 to −0.30), and by moderate-high scores on autonomy (Z-score 0.44).
The third cluster (Table 3), designated eudaimonic (49% of the sample), was characterized by higher scores (Z-scores ranged from 0.51 to 0.71) than the other two clusters in all six PWB dimensions other than autonomy, which received a moderate score (Z-scores = 0.36).
Cluster membership, life satisfaction, adjustment, and resilience
The chi-square tests conducted to determine the effects of cluster membership on the distribution of participants across levels of life satisfaction (χ2 = 33.7; df = 4; p < 0.000), resilience (χ2 = 23.4; df = 4; p < 0.000), and adjustment (χ2 = 9.9; df = 2; p < 0.001) were significant. A comparison of the expected and observed values indicated that low levels of life satisfaction were more likely (standardized residual >2) among those in the self-devaluing cluster and less likely (standardized residual <2) among those in the eudaimonic cluster, and vice versa (Fig. 2). A comparison of expected and observed values in resilience reveals the same significant pattern of life satisfaction (Fig. 3). With regard to mental adjustment, a comparison of expected and observed values indicates that low levels of maladjustment are more likely (standardized residual >2) in the eudaimonic profile (Fig. 4).
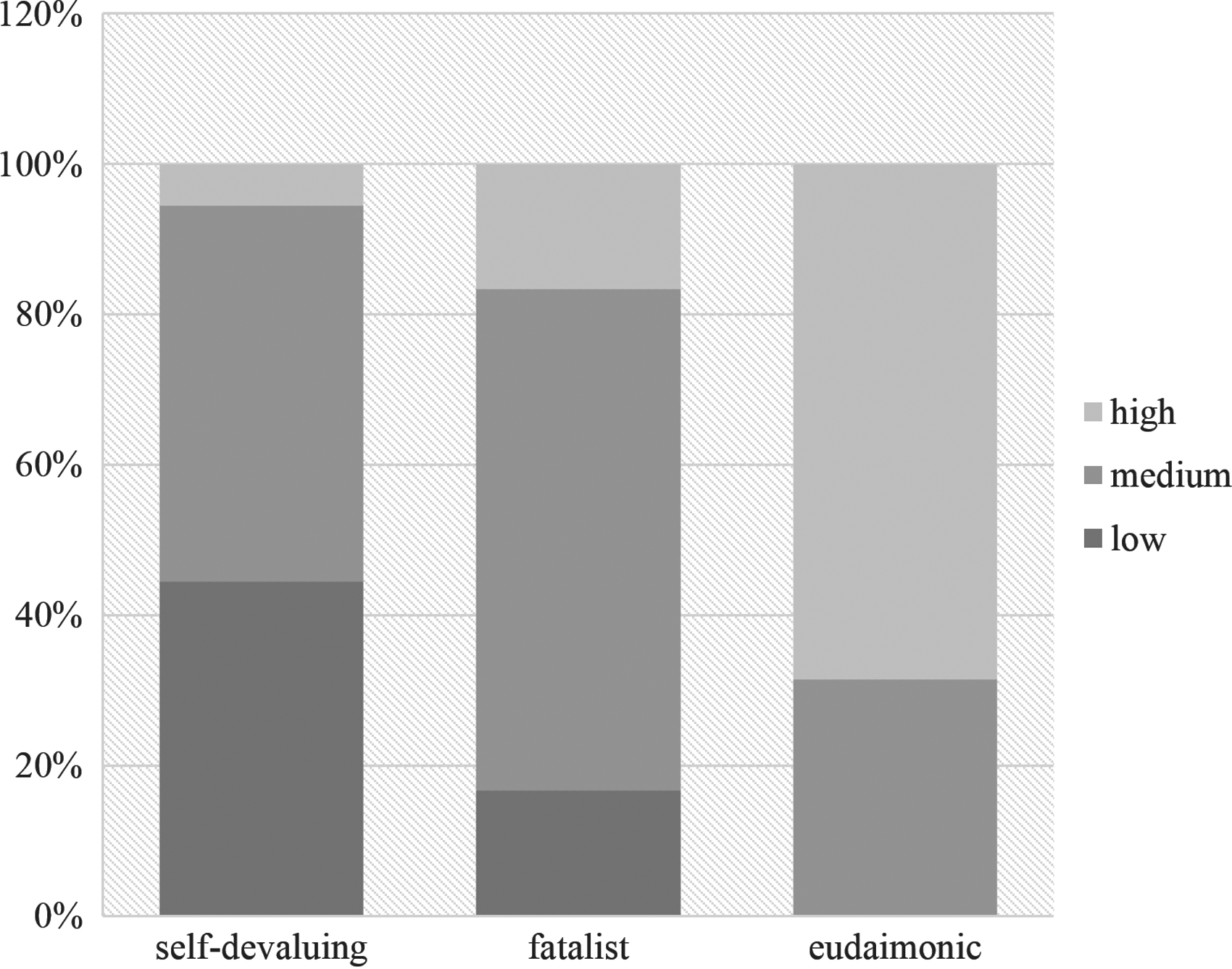
Distribution of life satisfaction levels within the self-devaluing, fatalist, and eudaimonic clusters.
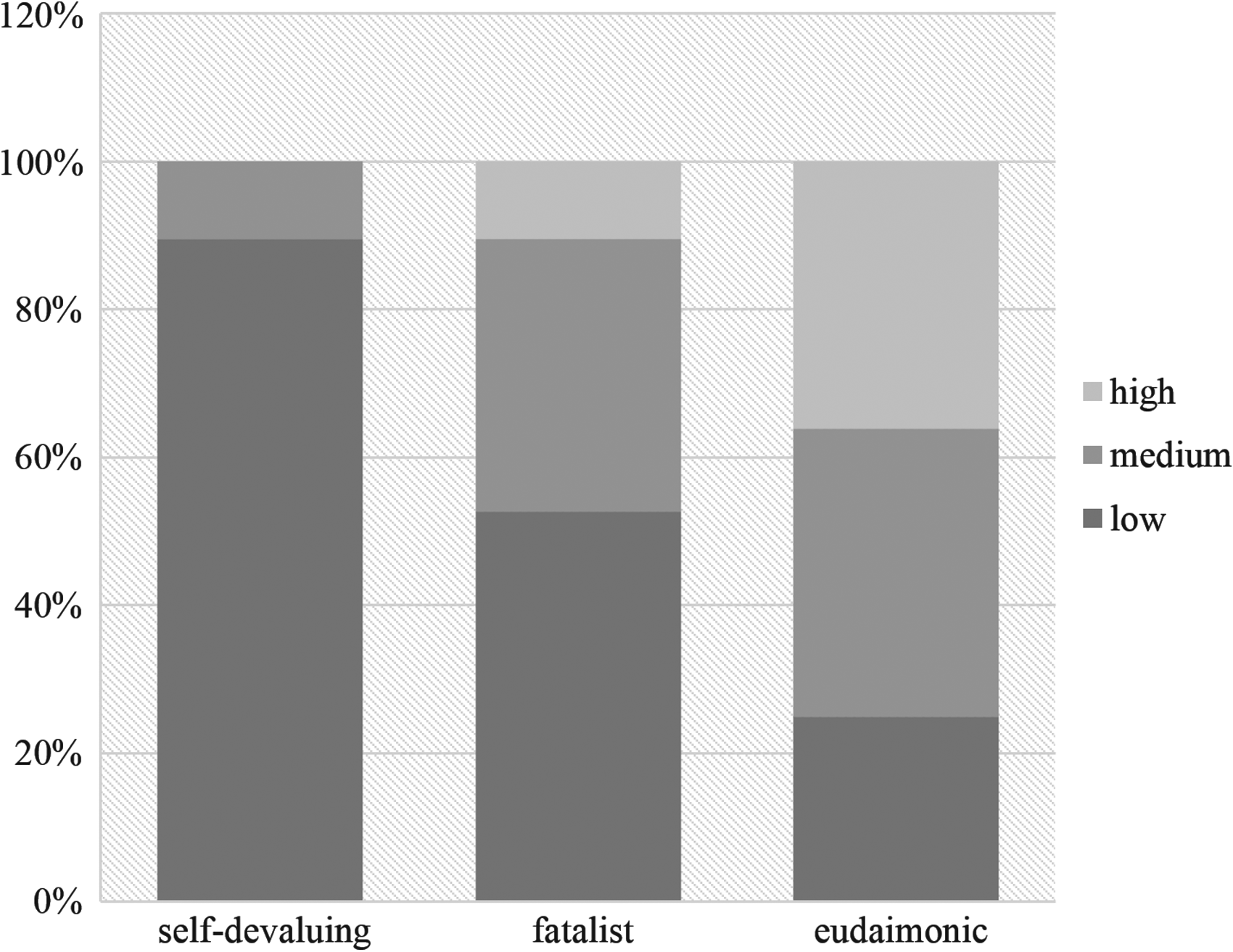
Distribution of resilience levels within self-devaluing, fatalist, and eudaimonic clusters.
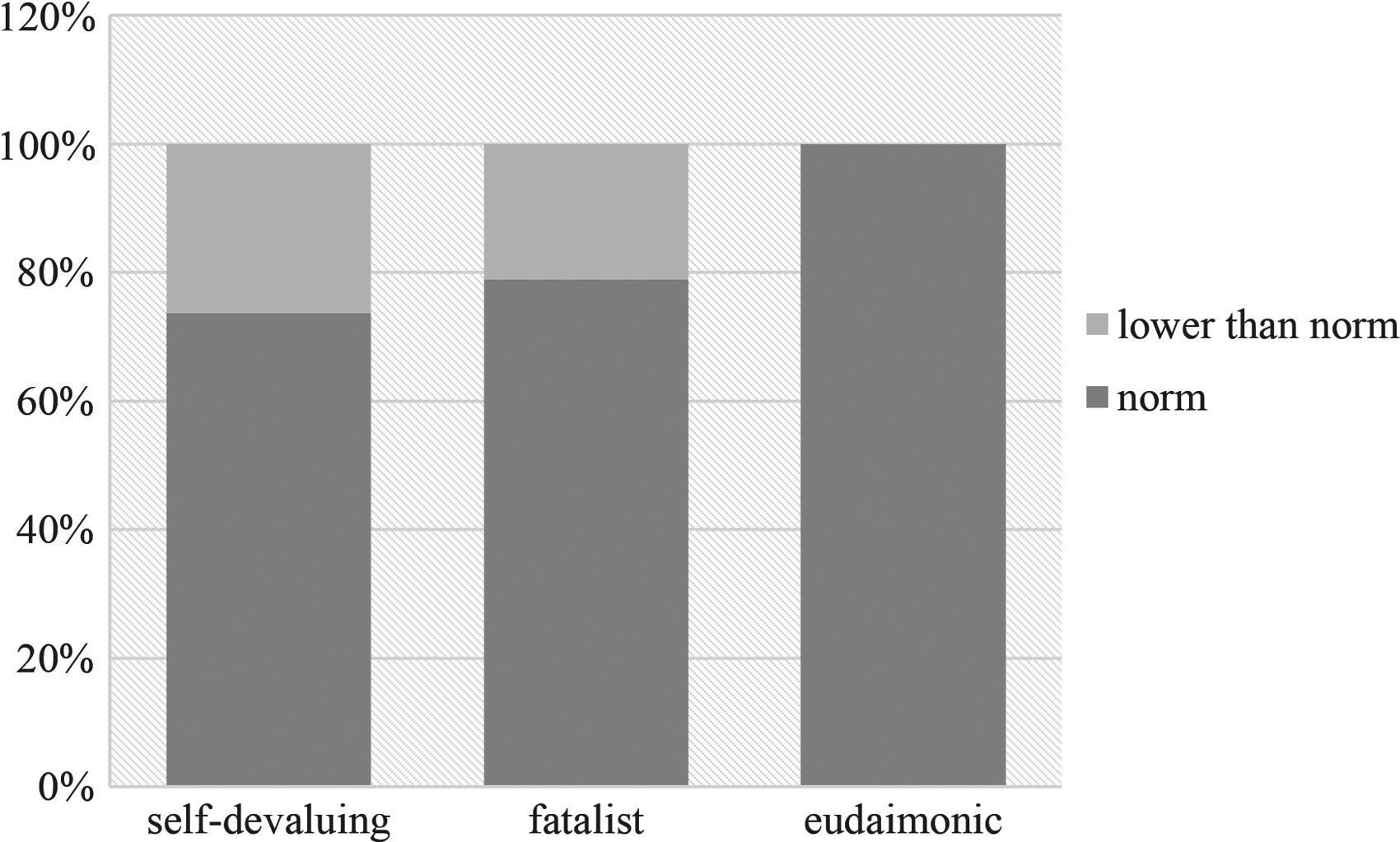
Distribution of adjustment levels within self-devaluing, fatalist, and eudaimonic clusters.
Cluster membership and clinical evidences
Three profiles of psychological functioning have been identified by comparing the cluster solution retained with the clinical guidelines of the Ryff and Keyes multidimensional model. 24
Participants belonging to the self-devaluing cluster rely on the judgment of others to make important decisions. They wish to be different from what they are. They have few close trusting relationships with others.
The participants belonging to the fatalist cluster possess a sense of personal stagnation. They have few goals, have difficulty managing everyday affairs, and lack a sense of control over the external world. On the other hand, they possess moderate independence.
Participants who belong to the eudaimonic cluster possess a positive attitude toward self. They have warm, satisfying, and trusting relationships with others. Furthermore, they are capable of strong empathy and intimacy and are open to new experiences. Finally, they are self-determined and independent, capable of resisting social pressures.
Discussion
To our knowledge, this study is the first one that applied the multidimensional model of PWB proposed by Ryff and Keyes 24 to assess the current state of well-being of YA SCCs and their SIBs of the same families. The first interesting finding is that YA SCCs and their own SIBs did not differ, neither in mean scores of PWB and in levels of life satisfaction, resilience, or mental adjustment nor in the cluster membership. With regard to mental adjustment and life satisfaction, these results appear to align with the literature in this field, in that they highlight that SCCs score worse than their SIBs on overall physical, but not emotional, aspects of quality of life and that most survivors reported that they are currently satisfied with life. 15 Furthermore, SCCs and their SIBs remain psychologically adjusted compared with population norms. 15
These results allow to understand the importance of the thriving model of adjustment proposed. In fact, from an impairment 12 perspective, only a low percentage of the participants is considered in need of support due to their symptomatology and to their psychological maladjustment. However, from a positive human health perspective, 25 with respect to living a purposeful life and effectively engaging in life, half of the sample manifests a need of well-being promotion. Effectively, consistent with the results of the most recent literature, 39 the present study evidenced that only the eudaimonic profile highlighted a fully functioning status: its members were globally satisfied with life and perceived themselves as able to manage stressful life events. On the contrary, the self-devaluing and fatalist ones were more lacking on these well-being outcomes, even if the majority of them were psychologically adjusted.
The choice to use a person-centered approach allowed us to verify the uniqueness for both SCCs and SIBs of some specific dimensions of PWB. In fact, autonomy, self-acceptance, and positive relationships played a more crucial role in enhancing life satisfaction and resilience than environmental mastery, purpose in life, and personal growth. These results lead to an interesting research question. In fact, the majority of the literature on resilience highlights the effective role of environmental mastery, purpose in life, and growth in preventing anxiety, depression, and psychological disorders and in fostering happiness and life satisfaction.
On the contrary, to date, there is little evidence regarding the importance of autonomy from social judgment and of the awareness of personal resources and limits. It could be important to verify if these specific resources are important in all the psychological phases of response to illness diagnosis or only in some of them. Furthermore, it could be interesting to verify whether these dimensions are critical in promoting resilience and adjustment exclusively in YA SCCs and their SIBs or if they are also important in promoting these characteristics in the general YA population.
Implication for clinical practice
From a clinical and applied perspective, the results of the present study indicate the need to establish psychosocial services that engage not only patients but also their SIBs. 40
Furthermore, it is crucial to offer both examinations and interventions aimed not only to prevent psychological maladjustment but also to promote PWB. This second type of action consists of fostering programs and environments that support in the participants the desire to care for themselves.41,42 Such oversight must sustain the improvement of a personal awareness that advocates the will to be autonomous, purposeful, and engaged with life.
We think that an important guideline in this direction comes from the WHO 43 that highlighted the crucial role of the life skills education programs for enhancing well-being. Life skills may be defined as abilities for adaptive and positive behavior that enable individuals to deal effectively with the demands and challenges of everyday life. 43 WHO identified five basic areas of life skills that are relevant across cultures: (1) decision-making and problem solving; (2) creative thinking and critical thinking; (3) communication and interpersonal skills; (4) self-awareness and empathy; and (5) coping with emotions and coping with stress. To date, the few studies available verified the effectiveness of life skills education programs in enhancing PWB,44,45 proving the relevance to carry on this new road.
Limitations and strengths
Some limitations were evident and largely pertained to the sample. First, the small sample size of this study restricts both interpretation and generalization of the results. More specifically, it could compromise the power to detect differences in PWB profile and in other well-being variables based on SCC versus SIB membership.
Another limitation is that all the SCCs were survivors of blood cancer. It limits the utility of these findings to other typology of cancer survivors. More research with larger samples is needed to clarify the function and correlates of PWB in the experience of cancer survivorship of both patients and family members.
It may also be useful in future research to include a control group of patients affected by another chronic illness or affected by another traumatic event to verify whether the pattern of response to illness and survivorship experience was owing to the cancer experience or whether it reflects a possible pattern of the struggle with other stressful events.
Another limitation is the use of the short version (i.e., 18 items) of PWB scale that has been recently recognized by Ryff 46 as less reliable than the medium and long forms because off psychometric problems with the individual scales (low alpha coefficients). That was because items for the short version were not selected to maximize internal consistency, but rather to maintain fidelity with the conceptual foundation of each scale. 46 In future studies, it could be relevant to use the medium version (i.e., 42 items) for a more reliable understanding of the unique role of each PWB dimension.
Despite the marked limits, the present study has three main strengths. The first one is its joined focus on both SCCs and their own SIBs that allows highlighting their similar pattern of response to survivorship experience. The second one is its thriving perspective that allows verifying the need to extend and integrate the adjustment model aimed to threatening and preventing psychological disorders with the thriving ones aimed to enhance PWB. The third one is its person-centered perspective that encourages an integrated and individual comprehension of the psychological trajectory of the participants.
Footnotes
Acknowledgments
The authors thank the survivors and their SIBs for their precious participation in the study.
Ethics Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
No competing financial interests exist.