
Abstract
Purpose:
Childhood cancer survivors (CCS) are at increased risk of primary gonadal insufficiency (PGI). This study evaluated the prevalence and clinical characteristics of PGI in CCS.
Methods:
In this single-center, retrospective, observational, longitudinal study, we characterized CCS with PGI attending the oncology Long-Term Follow-Up (LTFU) Clinic at an Australian university hospital (January 2012–August 2014). From a cohort of 276 CCS, 54 (32 males) met criteria for PGI: elevated gonadotropins plus low estradiol/amenorrhoea (females) or low testosterone/small testicles for age (males).
Results:
Median age at primary diagnosis was 4.8 years (inter-quartile range [IQR] 3.0–9.7 years) and at LTFU, it was 22.3 years (IQR 18.2–25.7 years). Fifty-three participants (98.1%) were treated with known highly gonadotoxic therapies: alkylating chemotherapy (96.3%), radiotherapy (70.3%), total body irradiation (29.6%), bone marrow transplantation (51.9%), or multimodal protocols (68.5%). At primary diagnosis, 86.7% participants were Tanner stage I and at LTFU, 89.1% participants were Tanner stage V. More females (95.5%; n = 21) than males (40.6%; n = 13) were treated with hormone development therapy (HDT) (p < 0.01). Of these, more than half (n = 18; 7 males) required pubertal induction. There was no significant difference in serum luteinizing hormone/follicle stimulating hormone (LH/FSH), testosterone/estradiol between those untreated and those treated with HDT. Among those on HDT, 60.7% had persistently elevated FSH±LH and 33.3% had low testosterone or estradiol. Six males had semen analysis (five azoospermic, one oligospermic). Psychological assessment was documented in 61.1% of participants, and two-thirds reported fertility concerns.
Conclusion:
PGI is an evolving phenotype that is common in CCS. Suboptimal treatment and non-adherence occur frequently. Ongoing assessment is essential to ensure prompt diagnosis, adequate intervention and to promote HDT adherence.
Introduction
M
In males, PGI is defined as impaired spermatogenesis, testosterone production, or both. 10 As Leydig cells have greater resistance to chemo/radiotoxicity in comparison to spermatogonial germ cells, males CCS may have elevated follicle stimulating hormone (FSH), low inhibin B, reduced testicular volume, and azoospermia; however, they may maintain adequate testosterone production. Therefore, normal pubertal development and sexual function may be preserved.7,11,12 In females, <40 years of age, PGI is characterized by primary amenorrhoea (pre-pubertal) or secondary amenorrhoea (for >4 months), elevated FSH, and low estradiol. 13 Intermittent reproductive capacity may be preserved, as some ovarian function is retained in almost 50% of females with PGI and 5%–10% conceive spontaneous viable pregnancies.14,15 In both males and females, PGI diagnosis can be complicated by concomitant secondary gonadal insufficiency that is caused by hypothalamo-pituitary damage from surgery or cranial irradiation (>40 Gy); however, even doses >18 Gy are associated with decreased fertility.16,17
Factors affecting the risk of PGI include cancer type, treatment modality, age at diagnosis, and sex. 18 Chemotherapeutic agents, specifically alkylating agents (AA), (e.g., cyclophosphamide, busulphan) are gonadotoxic in a dose-dependent manner. 19 Cyclophosphamide is particularly gonadotoxic, affecting both resting and dividing cells, and cumulative doses >7.5 g/m2 are associated with PGI.10,19 In males, doses >7.5 g/m2 are associated with reduced fertility and azoospermia, although testosterone production is often maintained unless dose exposures exceed 20 g/m2.10,12 In females but not males, the age of chemotherapy exposure affects PGI risk; females who are treated after 6 months of age but before puberty are at lower risk due to ovarian quiescence, causing diminished ovarian perfusion and exposure to chemotherapeutic agents. 20
The gonadotoxicity of gonadal irradiation is dependent on pubertal status and radiotherapy dose and location (direct gonadal, total body irradiation [TBI], or scatter from abdominal/pelvic irradiation). 19 Pre-pubertal males are at increased risk, and direct testicular radiotherapy can impair fertility at low doses; 1–3 Gy is associated with reversible azoospermia, and permanent azoospermia can occur after >3–6 Gy.10,21,22 Testosterone production is preserved until higher dose exposures (>24 Gy if pre-pubertal and >30 Gy if post-pubertal). However, subclinical Leydig cell insufficiency may be observed after doses <14 Gy.21,22 In contrast, post-pubertal females are at greater risk of radiotherapy-induced PGI due to a smaller follicular reserve pool. Therefore, abdominal/pelvic irradiation doses associated with infertility decrease with increasing age: 20.3 Gy:birth, 18.4 Gy:10 years, 16.5 Gy:20 years, and 14.3 Gy:30 years.23,24
The gonadotoxic effects of bone marrow transplantation (BMT) are secondary to pre-conditioning regimens, notably TBI, high-dose AA, and the cumulative gonadotoxicity of multimodal protocols.25–27 In females, ∼50%–60% receiving chemotherapeutic conditioning and almost all additionally receiving TBI develop PGI.28–30 In males, the majority receiving TBI develop Sertoli and mild Leydig cell damage.29,31 Surgery to the pelvis or gonads (e.g., for neuroblastoma or gonadal tumors) can also directly impact fertility due to removal of, or damage to, gonads and their sympathetic nervous supply.8,32
The increased risk of PGI in CCS is well documented. However, comprehensive clinical data regarding puberty, fertility, and treatment in this group are limited. 8 Therefore, the aim of this study was to determine detailed clinical characteristics of participants with PGI from a large cohort of CCS with a broad spectrum of oncological diagnoses.
Methods
Participants and study design
This was a single-center, retrospective, observational longitudinal study that evaluated CCS attending the oncology Long-Term Follow-Up (LTFU) Clinic at an Australian pediatric university hospital. To attend the LTFU Clinic, participants must be 5 years disease free. Patient information was extracted from a database of all participants attending the clinic between January 1, 2012 and August 15, 2014 (n = 276). Database information was coded by clinicians and input by a research assistant (baseline demographics, height/weight/BP, investigations, medications, examination findings, and late effects.) Six participants attended twice during this period, but data were only extracted from the first clinic visit.
Definitions
Primary gonadal insufficiency
Elevated gonadotropins, at any point plus low estradiol/amenorrhoea (females) or low testosterone/small testicles for age (males). 33 Therefore, participants with central hypogonadism (persistently low gonadotropins) were excluded from the study. Participants treated with cranial radiotherapy but with elevated gonadotropins met PGI criteria and were included.
Data collection
Setting
Department of Oncology, The Children's Hospital at Westmead, Sydney, Australia.
Demographics
Date of birth, age at diagnosis and LTFU Clinic visit, sex, primary cancer diagnosis, and treatment protocol (including radiation dose/location, AA/cyclophosphamide [dose/m2], BMT conditioning).
Clinical data
Height/weight, Tanner stage at diagnosis and LTFU visit, sexual function, symptoms of hormonal deficiency, current medication, and contraceptive/fertility status. Height/weight were measured using standard anthropometric techniques with participants in light clothing and shoes removed. Pubertal status was assessed directly by physicians using Tanner staging.33,34 Testicular volume was recorded using a Prader orchidometer.
Biochemical data
Blood samples collected within 6 months of the extracted LTFU visit were included: testosterone (males) and estradiol (females), luteinizing hormone/follicle stimulating hormone (LH/FSH), and vitamin D. Anti-mullerian hormone (AMH) was measured only in selected females. Blood samples were analyzed at the institution's NATA-accredited Clinical Diagnostic Laboratories. Gonadotropins were measured using the Immulite Immunoassay analyzer (Siemens Healthcare Global) and gonadal steroids by an in-house radioimmunoassay that was specifically developed to be sensitive at peri-pubertal ranges. Results were considered abnormal if outside age-specific standardized local laboratory reference ranges: males—LH: 0.2–6.1 IU/L, FSH: 0.5–6.3 IU/L, testosterone: 3–13 nmol/L (14–18 years) or 11–30 nmol/L (≥18 years); females—LH: 0.6–9.8 IU/L, FSH: 1.4–6.8 IU/L, estradiol: 100–410 pmol/L.
Semen analysis and cryopreservation
Offered to males ≥16 years old with clinical suspicion of Sertoli cell dysfunction, after appropriate counseling from a clinician.
Bone mineral density
Measured using a narrowed fan-beam DEXA (Lunar Prodigy; GE Healthcare) and analyzed using GE Encore 13.60 software. Results within 12 months of LTFU were included for analysis.
Psychological assessment
Data on psychological health were collected from evaluation sheets completed by the LTFU psychological team. Issues in the following areas were recorded: family/parents, fertility, sleep, school/education, diet/exercise, drugs/alcohol, mood, anxiety, peer relations, work/vocational, cognition, medical-related appearance, identity/sexuality, and romantic relationships.
Statistics
Data were transferred onto an Excel spread sheet and analyzed using IBM SPPS® Statistics Program versions 22.0. Multivariate logistic regression models, Pearson's chi-square, and Student's t-tests were used to calculate p values, which were considered significant at 5% (p < 0.05).
Ethical approval
This study was approved by The Sydney Children's Hospital Network Human Research Ethics Committee (LNR/14/SCHN/263).
Results
Demographics
Participants were 54 CCS (males 32; 61.5%) meeting study criteria for PGI from a cohort of 276 CCS (19.6%). Median age at primary cancer diagnosis was 4.8 years (inter-quartile range [IQR] 3.0–9.7 years) and 22.3 years (IQR 18.2–25.7 years) at extracted LTFU appointment. There was no significant difference in the age at diagnosis (p = 0.94) or LTFU (p = 0.25) between sexes. Cancer diagnoses were leukemia (35.2%; n = 19), sarcoma (25.9%; n = 14), brain tumor (13.0%; n = 7), neuroblastoma (n = 5), lymphoma (n = 4), Wilms’ Tumor (n = 2), and one each for hepatoblastoma, germinoma, and refractory anemia with excess blast cells.
Tanner stage was documented at baseline for 83.3% participants (n = 45; 25 males) and at LTFU for 85.2% participants (n = 46; 27 males). At baseline, most were Tanner stage I (n = 39; 23 males) and at LTFU, most were Tanner stage V (n = 41; 25 males). Testicular volume at LTFU was recorded for 90.6% males, and mean size was 7.4 mL (range 2–17.5 mL).
Treatment protocols
Most participants received multimodal treatment protocols (68.5%; n = 37). Figure 1 illustrates the overlap between gonadotoxic agents used: Of 54 participants, 53 (98.1%) were treated with an AA, TBI, focal radiotherapy, or multiple gonadotoxic agents. The remaining participants received five chemotherapeutic agents. All participants were treated according to standard chemotherapy protocols, 52 of which (96.3%) included an AA. Cyclophosphamide was used most commonly (n = 50) followed by busulfan and ifosfamide. Participants’ treatment protocols contained one to five AAs, with most including one (32.7%; n = 17) or two (44.2%; n = 23) AA. Cyclophosphamide (g/m2) dosage data were available for 40 participants. Median dosage was 9.7 g/m2 (IQR 6.2–16.0 g/m2), with no significant difference between sexes (p = 0.78).
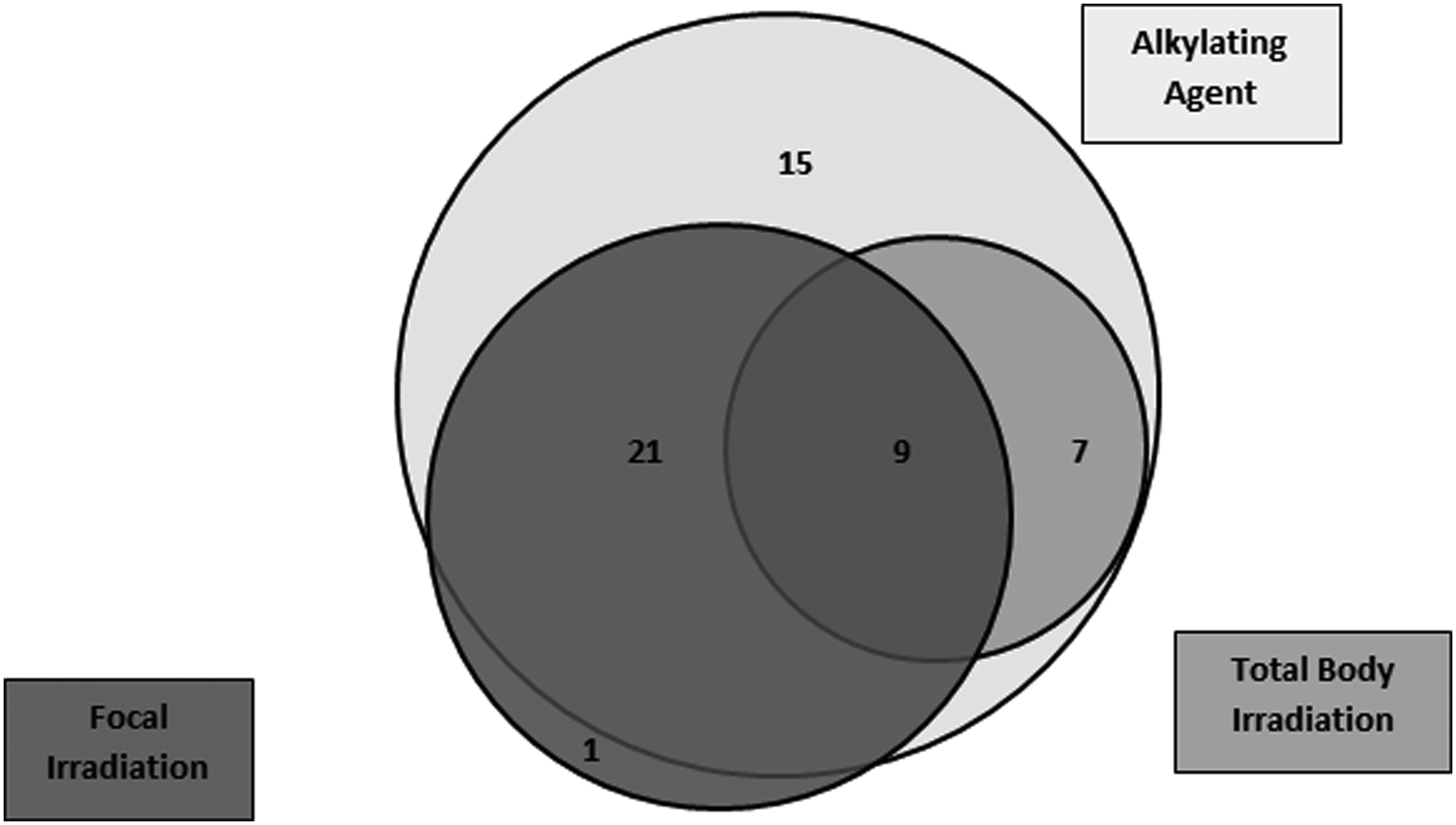
Gonadotoxic agents in a cohort of childhood cancer survivors with primary gonadal insufficiency (n).
Thirty-eight (70.3%) participants received radiotherapy, 16 (29.6%) of whom received TBI (Table 1). All participants treated with TBI, abdominal/pelvic or testicular irradiation also received cyclophosphamide. Twenty-eight participants (51.9%; 15 males) received a BMT (13 autologous, 15 allogenic), all of whom received ≥1 AA or an AA and radiotherapy. All participants treated with gonadal irradiation (males: testicular [n = 4]; females: abdominal/pelvic [n = 4]) were pre-pubertal at treatment onset. All required hormone development therapy (HDT), and all but one (male) required pubertal induction. Of the BMT cohort, all but one was pre-pubertal at treatment onset and 79% required HDT. This included 93.6% of BMT participants treated with TBI and cyclophosphamide and 66.7% of BMT participants treated with chemotherapy alone. Those not requiring HDT were treated with lower cyclophosphamide doses (1.2–8.0 g/m2) than those requiring HDT (4.8–17.5 g/m2). Participants receiving radiotherapy or BMT were significantly more likely to be treated with HDT (p = 0.02 and p < 0.01, respectively).
Radiotherapy doses expressed as range or median and (IQR):
39.4 Gy (IQR 18–54.9 Gy), b10.8–45.0 Gy, c10.8 Gy-24.0 Gy, d12.6 Gy (IQR 12.0–13.2 Gy).
48.7 Gy (IQR 30.0–77.4 Gy), f10.8–50.4 Gy, g12.6 Gy (IQR 12.0–13.2 Gy).
Includes focal irradiation to the axilla (n = 1) and lower limb (n = 3).
9/10 received TBI and focal radiotherapy.
IQR, inter-quartile range; TBI, total body irradiation.
Hormonal profiles and HDT
Gonadotropin and gonadal hormone results are shown in Tables 2 (males) and 3 (females). Ten participants had suppressed LH/FSH at the extracted LTFU Clinic as a result of HDT.
m/n = number of participants with hormonal parameters measured/total number of participants in cohort.
FSH, follicle stimulating hormone; HDT, hormone development therapy; LH, luteinizing hormone.
m/n = number of participants with hormonal parameters measured/total number of participants in cohort.
Female participants excluding one pregnant participant (estradiol 1632 pmol/L, LH 9.8 IU/L, FSH 0.1 IU/L).
Estradiol results excluded for four participants on oral contraceptive pill were <18, <18, 33, and 46 pmol/L.
Males
Thirty-two males had PGI, by definition, of whom 13 (40.6%) were treated with HDT at any time. Seven males required pubertal induction, all of whom remained on treatment at the extracted LTFU Clinic. Six males were treated for later symptomatic testosterone deficiency and secondary sexual characteristic development. In all, 12 males remained on HDT at the extracted LTFU. Of these, 10 received intra-muscular testosterone undecanoate, 1 used testosterone patches, and 1 used oral testosterone undecanoate. In total, eight males had low testosterone, of whom five were reportedly on HDT and all were Tanner stage V. Five males had documented symptomatic improvement (improved libido, mood, “mental clarity,” stamina) after HDT or worsened symptoms when non-adherent.
Females
Twenty-two females had PGI, of whom 21 (95.5%) were treated with HDT at any time. Eleven females required pubertal induction, and the remainder were treated for later symptomatic estrogen deficiency or secondary sexual characteristic development. Eighteen females remained on HDT at the extracted LTFU Clinic, including all those treated for pubertal induction. Of these, 10 used oral estradiol-valerate and 4 used estradiol hemihydrate patches. Four were prescribed ethinyl-estradiol containing an oral contraceptive pill (OCP) for additional treatment of acne. As ethinyl-estradiol may cross-react with estradiol on radioimmunoassay, estradiol concentrations in this group may be invalid. 35 Therefore, these results were eliminated from whole-group analysis. Of the four females not on HDT, one was pregnant, one was considering HDT, and two were prescribed HDT but non-adherent. Five females had low estradiol, which included the known non-adherent participants and three participants on non-OCP HDT. AMH was available for four females (18.2%), three of which were low (<0.1–3.0 pmol/L) although one had naturally conceived two pregnancies.
Significantly more females than males were treated with HDT (p < 0.01). Of those on HDT, 63.6% males and 58.8% females had persistently elevated FSH±LH and 45.5% males and 23.1% females had low testosterone or estradiol, respectively. There was no significant difference between HDT-treated and -untreated participants in serum LH/FSH, testosterone, or estradiol (Tables 2 and 3).
Sexual and reproductive health
Six males had semen analysis, of which one was oligospermic (0.1 million/mL) and opted for semen cryopreservation and five were azoospermic. Reasons cited for not providing samples included young age (n = 5), disinterest in fertility status (n = 4), no current relationship (n = 3), and no specified reason (n = 14). Sexual history was documented for 48.1% participants (n = 26; males 20). Of the males, 75.0% (n = 15) were reportedly sexually active, seven used contraception, and one had conceived a pregnancy. All females with documented sexual history were sexually active. Four used barrier contraception, one was pregnant (second spontaneous conception), and one had completed an unsuccessful in vitro fertilization cycle.
Bone health: vitamin D and bone mineral density
Fifty-two participants (96.3%) had vitamin D measured, 10 of whom were vitamin D deficient (<50 nmol/L). A further seven had resolved vitamin D deficiency after treatment. DEXA results were available for 10 participants (7 males). Five participants (four males) had osteopenia. All were vitamin D replete on vitamin D supplementation, and four were on HDT. No participants had osteoporosis.
Psychological health
Forty-three (79.6%) participants had a documented psychological assessment. Detailed data were available for 33 participants, of whom 27 (81.8%) reported an issue in at least one domain. Primary concerns were fertility (n = 21; males 12), cancer/treatment-related appearance (n = 20), and mood (n = 17). Few participants reported concerns regarding romantic relationships (n = 4) or identity/sexuality (n = 3).
Discussion
PGI is a common late effect of childhood cancer, and it is clearly identified in one in five CCS in this study. The gonadotoxic effects of standard cancer therapies are well established. Indeed, all but one participant was treated with known highly gonadotoxic agents with anticipated outcomes. 32 Therefore, adequate surveillance and prompt recognition of at-risk patients is imperative.
A number of obstacles exist to enable the accurate assessment and diagnosis of PGI in young CCS. Pubertal status, which is highly relevant to predict the impact of cancer treatment on pubertal development and fertility, can be challenging to evaluate clinically. For males, germ cell damage causing testicular atrophy can limit pubertal assessment by testicular volume, as seen in this cohort. 10 In both sexes, adrenal androgen-mediated development (pubic/axillary hair growth) further complicates evaluation and no internationally accepted assessment protocol exists.10,36–38 Importantly, many CCS progress through puberty normally, including secondary sexual characteristic development. However, this does not necessarily equate to normal reproductive health, and, as such, hypogonadism and impaired fertility status should be assessed separately. 26
Inaccuracies exist when ascertaining hormonal deficiency symptoms, as these are subjective and confounded by other variables, for example, fatigue may be secondary to a disturbed sleep cycle. As the majority of CCS were pre-pubertal at cancer diagnosis, many will not have experienced fully adequate gonadal hormone levels and may not recognize relevant symptomatology such as hot flushes, vaginal dryness, and erectile dysfunction. Therefore, patients should be explicitly questioned regarding these and educated accordingly. Nonetheless, the use of such symptoms to indicate hormonal abnormalities or denote HDT efficacy is useful; almost half of all HDT-treated males reported symptomatic improvement on treatment.
To assess fertility, additional parameters are required. In males, although semen analysis remains the gold standard, participants of this study were reluctant to provide samples (<20%), limiting both assessment and the opportunity for semen cryopreservation.10,39 In such cases, inhibin B, the most accurate serum marker of impaired spermatogenesis, may provide a more acceptable alternative for fertility assessment. 12 In females, AMH, a serum marker of ovarian function, is a convenient and superior adjunct or alternative to FSH due to its consistency throughout the menstrual cycle.23,40
Once a diagnosis of PGI has been established, management includes HDT, fertility preservation, and fertility treatment if indicated. We utilize the term HDT as opposed to hormone replacement therapy to focus on the development and normalization of pubertal and hormonal parameters. Significantly more females (95.5%) than males (40.6%) were treated with HDT, which may reflect that females have a more obvious marker of PGI in menstrual dysfunction, thus increasing identification. All who require pubertal induction should continue on HDT, as they clearly have inadequate endogenous hormonal concentrations and achieving full adult sexual maturity should not be considered the end point of HDT. Those with normal gonadal hormones and elevated gonadotropins represent a clinical dilemma. For such patients, we recommend more frequent follow-up to recognize deterioration in the compensated state and to promptly detect subclinical deficiency.
A finding of concern was the lack of difference in gonadal and gonadotropin hormone concentrations between those treated and those not treated with HDT. Suboptimal replacement or therapy non-adherence is indicated by elevated gonadotropins, which was evident in nearly two-thirds of those treated with HDT. As one third of these also had low testosterone/estradiol, there is a vital need for further evaluation of HDT dosing and formulations, and we recommend that clinicians explicitly discuss issues regarding therapy adherence with CCS, and provide education accordingly.
Fertility preservation options in CCS are dependent on sex, pubertal status, and urgency of cancer treatment initiation.8,41–43 We recommend that clinicians routinely discuss the impact of cancer treatment on fertility and explain fertility preservation options during the acute phase of cancer diagnosis and treatment, if developmentally appropriate. Fertility discussions should be revisited regularly throughout LTFU and fertility assessment and preservation should be offered, as necessary.
The wider health consequences of long-term gonadal hormone deficiency necessitate regular assessment of psychological, cardiometabolic, and bone health.9,10,44,45 In this study, DEXA measurement was limited (18.5%). However, given the high rate of osteopenia (50% of those measured), bone mineral density should also be assessed regularly. Psychological issues are also common in CCS and can be further exacerbated by hormonal deficiency. 46 Two-thirds of participants had psychological concerns related to fertility in this study. As such, we recommend that clinicians enquire actively about these sensitive subjects, including relationships and identity/sexuality that were reported infrequently in our cohort.
Study strengths include the use of a detailed database comprising clinical data obtained from face-to-face consultations, examinations, and biomarkers. Limitations include infrequent participant follow-up due to the clinic model and limited detail on fertility assessments. Furthermore, this study measured testosterone and estradiol with radioimmunoassay rather than mass-spectrometry, which is more sensitive at low estradiol concentrations. 47
Conclusion
Survival rates for childhood cancer are continuing to improve, and LTFU Clinics must adapt to the changing medical needs of CCS throughout adolescence and adulthood. The significant risk of PGI for CCS is clearly demonstrated in this study, and the damaging long-term effects on both physical and psychological health are well known.8,9,48,49 Future studies should evaluate the reliability of non-invasive markers of fertility (AMH/inhibin B) in young CCS and utilize mass-spectrometry for gonadal hormone measurement. We recommend consistent and proactive surveillance to enable early identification of subclinical hormonal deficiency and PGI. Prompt endocrine referral, intervention, and promotion of HDT adherence should follow, to normalize pubertal development, maximize fertility, and promote long-term health.
Footnotes
Acknowledgments
The assistance of staff of the Academic Department of Adolescent Medicine, the Long-Term Follow-Up Clinic, the Department of Oncology and the Institute of Endocrinology & Diabetes at The Children's Hospital at Westmead is gratefully acknowledged. Dr. Liz Barnes from the Kid's Research Institute at The Children's Hospital at Westmead provided statistical support. Human resources were provided by Linköping University, Sweden.
Author Disclosure Statement
No competing financial interests exist.