
Abstract
Purpose:
To assess what is currently known about unmet needs and care experiences of adolescents and young adults (AYAs) with cancer, identify gaps in the research literature, and highlight potential areas for improvement in future research.
Methods:
Medline, PsycINFO, CINAHL, and EMBASE databases were searched to identify relevant studies from 1990 to July 2015. Eligible articles included self-reported care experiences or unmet needs of cancer patients aged between 15 and 30 years in the period between symptom onset and 2 years post-treatment. Qualitative and quantitative designs were included.
Results:
Forty-five articles from 39 studies (23 qualitative, 12 quantitative, and 4 mixed methods) were rated as “adequate” or “good” quality and reviewed. The majority included any cancer diagnoses and none was longitudinal. There was considerable variation in age ranges and time since diagnosis between studies. Only two studies used standardized survey tools, with both tools validated on adult populations. The most common areas assessed for care experiences and needs were information/communication and fertility. In addition, care experience studies commonly examined clinical expertise and age-appropriate settings, while unmet needs studies reported on emotional support and peer interaction.
Conclusion:
Findings highlight the need for age-appropriate information and treatment facilities, access to emotional support services, and contact with peers. Fertility information and services are a priority issue for this group. Future research would benefit from a consistent definition of the AYA age range, increased used of standardized scales validated with this population, and longitudinal designs to assess changes over time.
Introduction
A
The challenges in treating AYAs with cancer are increasingly recognized, and best practice guidelines for their cancer care are being developed and implemented.5–7 Information about the quality of care provided to AYAs is needed to help inform these guidelines and to evaluate the impact of new initiatives for this age group. While service evaluation has traditionally focused on clinical information, there is growing recognition of the importance of assessing the patient's perspective of the quality of their care through patient-reported measures. 8 Two types of patient-reported measures are commonly discussed in the literature: patient-reported outcome measures (PROMs) and patient-reported experience measures (PREMs). PROMs generally focus on assessing dimensions of health-related quality of life and include patient reports of their functioning, symptoms, and psychosocial well-being.9,10 In contrast, PREMs aim to determine the extent patients’ care experiences meet their expectations and/or best practice recommendations. 8 Understanding patients’ unmet needs is one method for identifying gaps in patients’ care experiences. 11 Needs assessments identify the components of care patients feel are missing or not available. 12 A number of different need domains have been identified in the literature,11–13 including psychological and emotional (e.g., access to support programs), healthcare services (e.g., prompt access to test results), information (e.g., being provided with age-appropriate information), and practical (e.g., transport to treatment centers). The majority of studies assessing cancer patients’ unmet needs exclude adolescents.11,13,14
A second type of PREMs asks about patients’ care experiences, with patients indicating whether specific events or processes occurred during their care. 8 Care experience assessments focus on areas of care consumers or best practice guidelines identify as important and commonly assess patients’ interactions with HCPs, experiences at the treatment facility (e.g., waiting times), information provision (e.g., understandable, delivered when needed), communication (e.g., could ask questions), and coordination of care (e.g., information transfer between HCPs and/or treatment centers). Experience of care measures can be used to inform practice improvements.8,15 While there has been increasing interest in collecting population-based PREMs data from cancer patients,15–18 most studies do not include people as young as 15, and the proportion of late AYAs participating in these studies is generally small.16,19
A new wave of quality-of-care assessment in AYA cancer has recently emerged, with teams in the United Kingdom, United States of America, and Australia working to develop measures assessing the experiences of care and/or unmet needs of this age group.20–22 However, to our knowledge, there has not been a comprehensive systematic review that examines what is already known about unmet needs and care experiences for AYAs with cancer. While Taylor et al. 23 recently conducted a review of studies on AYA cancer, which included some aspects of experience of care, their focus was identifying mediators and moderators of psychosocial well-being and their review was limited to qualitative studies. Although the reviews by Smith et al., 24 Marris et al., 25 and Wilkins et al. 26 included all study designs, each focused on only one aspect of AYA care: nursing adolescents, 24 age-specific models of care, 25 and AYA transition experiences. 26
Adopting a comprehensive approach, this review aims to assess what is currently known about both unmet needs and care experiences of AYAs with cancer, identify gaps in the research literature, and highlight potential areas for improvement in the research undertaken in this area. We focus on studies that assess experiences and/or needs directly and include all research designs.
Methods
Search strategy
We searched Medline, PsycINFO, CINAHL, and EMBASE databases to identify articles that related to the unmet needs and care experiences of AYAs with cancer between January 1, 1990, and July 23, 2015. To ensure articles addressing these issues were captured, we used a broad range of search terms, developed through review of terms used in previous literature reviews of unmet needs and care experiences,14,23 examination of MESH terms used for key articles, and consultations with experts (see Table 1 for search terms used). Indexed subject headings and words within the article's body were searched. Only articles published in English were considered. The database searches were supplemented by searching references of relevant published reviews1,2,23–31 and articles included in our review. The lead author undertook the database searches.
An “and” function combined terms from the three columns.
AYA, adolescents and young adults.
Inclusion criteria
Qualitative and quantitative articles were eligible for review. There is no internationally agreed age range for AYA oncology, with, for example, Australia and the United Kingdom using 15–24 years, while the United States of America uses 15–39 years. For the purpose of this review, AYA was defined as 15–30 years. Articles were included if they reported care experiences or unmet needs; for the care period reported on, the study sample was aged between 15 and 30 years, the sample's average age fell within this range, or the article reported information separately for subgroups within this age range; the findings related to the period between symptom onset and 2 years after treatment completion; and reports came directly from patients (not parent reports, observations, or expert opinion). Articles that focused on quality of life, emotional distress, physical symptoms, or the experiences or needs of patients in a period 2 or more years post-treatment were excluded. Intervention trials and medical record reviews were also excluded. If one study generated more than one publication, all articles were included if different results were presented. However, if the sample and results were similar between articles, only the article with the most complete data was included.
All authors participated in the review process. A subset of abstracts and articles was assigned to each author for review against the inclusion and exclusion criteria, with each abstract and article reviewed by at least two authors. Disagreements were resolved by a third independent review, with subsequent discussion until consensus was reached.
Article classification and data extraction
Each author reviewed a subset of eligible articles, with each article reviewed by at least two authors. Articles were classified according to their methodology (qualitative, quantitative, mixed methods), and reviewers determined whether experiences of care or unmet needs were the main focus of the article, one of several key foci, or an incidental finding among study results. Reviewers also extracted the following data from each article: sample size, gender mix of sample, response rate, method of identifying eligible participants, method of data collection, whether the study used existing survey instruments, country of origin, age of participants at diagnosis, age when participating in study, treatment stage assessed (current, one or more specific periods [e.g., chemotherapy], overall experience) participants’ current treatment stage (e.g., time since diagnosis, currently on/off treatment), and study findings. The lead author compared the data extracted by each reviewer for consistency with discrepancies resolved by rereview of the article.
Research quality ratings
To assess the quality of research articles from different methodological traditions, quality criteria were specifically developed with reference to the Cochrane Handbook for Systematic Reviews of Interventions, 32 the Critical Appraisal Skills Programme, 33 and other guidelines and checklists.34–37 Criteria differed for qualitative and quantitative articles, but included consideration of repeatability, sample size, design, methodology, analytic rigor, and justification of conclusions (see Supplementary Appendix A1 for checklist; Supplementary Data are available online at www.liebertpub.com/jayao). Articles scored one point for every item satisfied, to achieve a total score ranging from 0 (lowest quality) to 15 (highest quality). Mixed methods articles were scored based on their average ratings for qualitative and quantitative components. Based on the total score, article quality was classified as poor (0–6.9), adequate (7–11.9), or good (12–15).
The ratings checklists were piloted on a subset of quantitative and qualitative articles and refined to ensure adequate inter-rater agreement. Once the checklists were finalized, at least two reviewers rated each article. Disagreements (ratings differing by three or more points) were resolved by referral to a third reviewer.
Results
A total of 7025 unique English language articles were identified, of which 5281 were assessed as not relevant based on their titles, for example, referring to AYA survivors of childhood cancer or to a clinical trial (Fig. 1). Abstracts for the remaining 1744 articles were read, and 1372 articles not meeting the inclusion criteria were eliminated. The remaining articles were read by at least two authors to confirm the inclusion criteria were met, and a further 323 articles were excluded. Reasons for exclusion at this stage are shown in Figure 1. The methodology of the remaining 49 articles from 42 separate studies was reviewed with the quality of each article assessed.
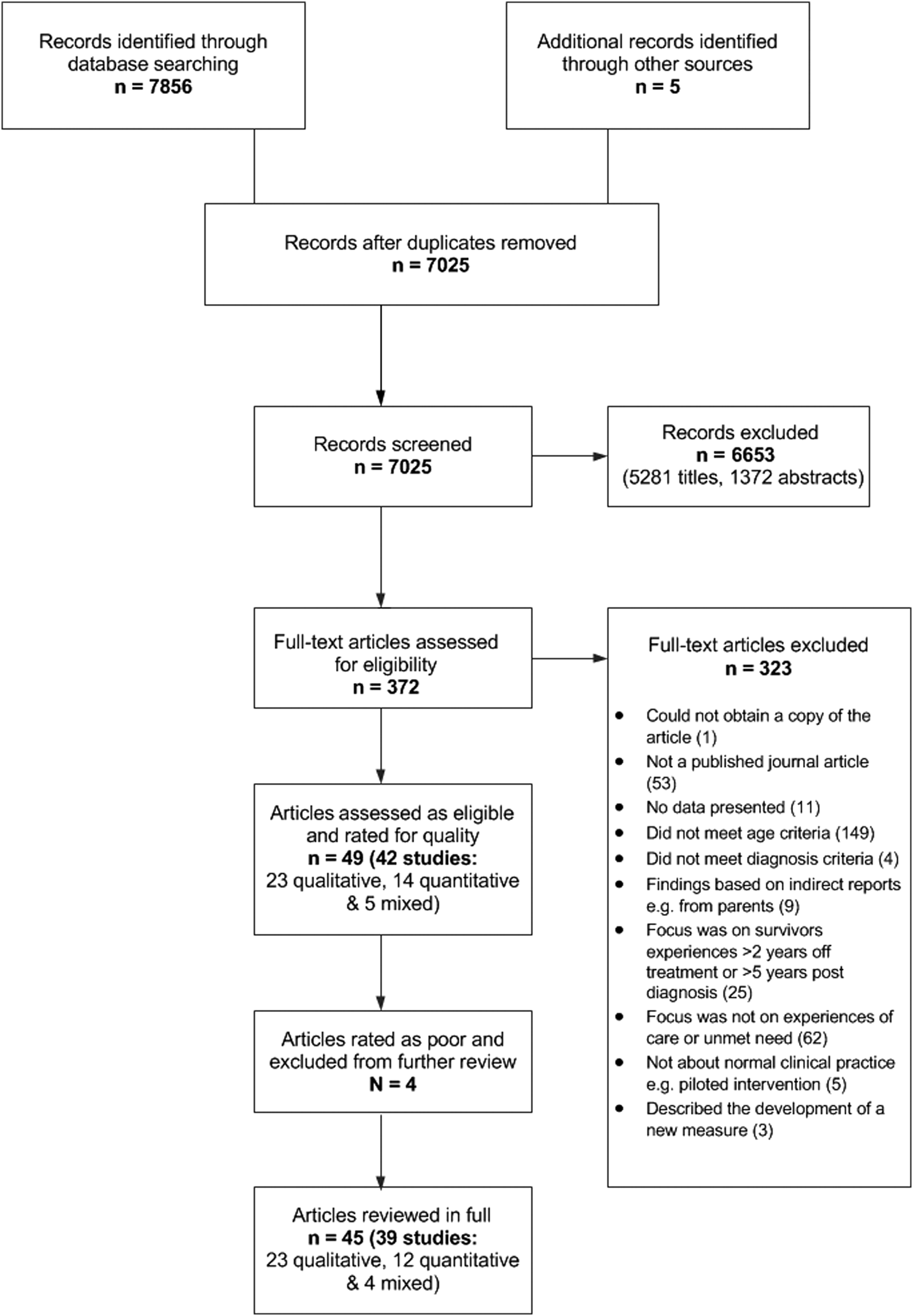
Flowchart of article selection process.
Description of studies
Table 2 summarizes methodological information for the 23 qualitative, 14 quantitative, and five mixed methods studies (detailed description of articles shown in Supplementary Table S1). Fifteen studies were from the United Kingdom, 15 from the United States of America and Canada, and 16 were from other developed countries. The majority of studies (33/42) involved patients with a mix of cancer diagnoses. Four studies targeted specific cancers, two targeted specific treatments, and three targeted patients having treatment that may affect fertility. Unmet needs or care experiences were the main focus of 30 studies, 8 reported unmet needs or care experiences as one of several study aims, while 4 focused on other outcomes, but included sufficient relevant information in their results for inclusion.
Across all study types, the most common avenue for patient recruitment was through adult hospitals (11/42). Sixteen studies recruited patients from a single hospital and 12 recruited from two or more hospitals. One study did not provide information on recruitment source. 38
The average quality ratings of the qualitative, quantitative, and mixed methods article were 9.8 (SD = 2.4), 10.3 (SD = 2.3), and 9.4 (SD = 3.4), respectively, giving the articles an average rating in the adequate range (Table 2). Four articles39–42 received a “poor” quality rating and were excluded from further review. After excluding these articles, the average quality rating across all studies remained in the adequate range (mean = 10.6, SD = 1.8).
Sample size, study participants’ age, time between diagnosis and study participation, and stage of care for the 45 remaining quantitative, qualitative, and mixed method articles are summarized in Table 3, while Table 4 provides detailed information for each study. Sample size was over 100 in three quantitative articles and two mixed method articles, with four quantitative and five mixed methods articles having 40 or fewer participants. Participants’ age ranges varied between articles, and the method of reporting participants’ age also varied. Sixteen articles reported the mean or median age of participants as under 20, while six reported it as over 30. Five articles included people over 40 with one quantitative article involving participants aged up to 74 years. 43 However, as this article reported on patients’ experiences at diagnosis when the median age of participants was 29 years, it was retained in the review.
Time of survey administration.
M = Males.
GP, General Practitioner; HCP, healthcare providers; OT, Occupational Therapy.
Information regarding when participants took place in the research also varied, with some articles reporting time since diagnosis, some reporting time since treatment completion, and some not reporting this information. As Table 3 shows, 18 articles did not provide information regarding the time interval between diagnosis and study participation. Two qualitative and two quantitative articles reported the average interval between diagnosis and study participation as less than 6 months, while for five qualitative and three quantitative articles, the interval was between 2 and 5 years.
Most commonly, articles focused on a specific period of care (17 articles), with 13 articles assessing general experiences or needs throughout cancer care (Table 3). While fertility preservation was the most common specific area focused on (five quantitative articles from five studies and six qualitative articles from five studies), other areas included diagnosis,44,45 chemotherapy, 46 radiotherapy, 47 and transitioning to follow-up care.48,49
While two studies reported in two articles used a validated survey tool,50,51 two studies reported in three articles adapted questions developed by others.21,52,53 However, the survey tool or set of questions used differed between studies.
Care experience findings
Thirty-four articles from 30 studies reported on AYAs care experiences, of which 22 were rated “adequate” for quality and 12 were rated “good.” Findings from articles rated adequate or good were similar. As articles from the same study often reported on similar care areas, studies rather than articles are reported. Across the three study designs, the most common areas examined were fertility (14/30), communication/information delivery (13/30), staff skills/expertise (11/30), age-appropriate treatment setting (8/30), and peer contact/support (8/30) (Table 5).
In the area of fertility, most studies found that young people received insufficient information about preservation options or the impact of treatment on fertility,54–57 with females more likely to find this information lacking or confusing.56–60 Of the five quantitative studies examining fertility experiences, two focused on sperm banking experiences and two focused on women's experiences of discussing fertility preservation and decisions. Both qualitative and quantitative studies reported that fertility discussions were associated with distress and embarrassment54,56,59–62 and five found that emotions impacted on some AYAs’ decision-making.54,56,58,60,63 While some young men found the sperm banking process straightforward,56,57,64 other studies reported more difficult experiences, with sperm banking facilities seen as inadequate, difficult to access, and insensitive.54,61,63 While the presence of parents at sperm banking facilities was a source of embarrassment for some,54,59,61,63 two studies reported that young people wanted their parents to be involved in fertility discussions and decisions.59,64
Communication experiences were most commonly examined through qualitative studies. Communication/information issues included the importance of the HCP in providing clear age-appropriate information about the disease, treatment, and implications for daily life,22,65–70 and the impact of uncertainty on patient well-being.65,67,68,70 The availability of information relating to AYA-specific issues (e.g., fertility, appearance changes, education, finance) was variable.22,47,62 Aspects of communication delivery were also highlighted, with HCP qualities of listening skills, sensitivity, empathy, and trust regarded as key facilitators of information exchange.22,46,48,66 Two studies suggested that young people can be reluctant to raise new issues with HCPs, relying instead on the information provided by their treatment team.22,71
The mainly qualitative studies examining staff skill/expertise focused on whether HCPs had age-specific knowledge and experience. Participants placed importance on being cared for by staff that were knowledgeable about AYA cancers and treatment.65,67,72–74 This was often a key prerequisite for patient trust and confidence.22,65,68,75 HCP's understanding of AYAs’ psychosocial needs was also highly valued.62,68
All study types examining age-appropriate treatment settings tended to focus on the inpatient experience. Key topics included access to facilities for recreation/distraction, relaxation, and studying; opportunities to mix with other young people with cancer; and the importance placed on privacy.22,51,62,66,67,75,76 The benefits of an AYA-friendly schedule were also discussed (e.g., sleep and waking times, visiting hours).62,76
Only one quantitative study used a validated questionnaire to explore AYA care experiences. Reynolds et al. 51 used the Youth Satisfaction Questionnaire, 77 which was originally developed for 9–18-year olds attending mental health services. The scale combines standardized items about overall satisfaction with researcher-developed items tailored to the treatment setting. Reynold's findings on the comparison between specialist AYA and other types of services are discussed in more detail below.
Unmet needs findings
Thirty-five articles from 31 studies reported the unmet needs of AYAs with cancer, with 21 articles rated “adequate” for quality and 14 rated “good.” Findings from articles rated “adequate” and those rated “good” were similar. The most common needs examined related to communication/information delivery (19/31), emotional support (18/31), fertility (17/31), and peer contact/support (16/31) (Table 5). Regardless of research design, studies commonly suggested that needs change as AYAs move through diagnosis and active treatment and into survivorship.3,22,44,52,65,67–70,74,75,78
Studies found that AYAs expressed a need for honest, timely, age-appropriate information in numerous areas, particularly diagnosis, fertility, treatment, health/lifestyle, and survivorship.3,21,22,52,65,68–70,72,73,78,79 The need for information to help young people prepare for their experience was a repeated theme.47,65,69–72 Studies suggest that higher unmet information needs are associated with greater distress and lower overall satisfaction with care.21,50,68,80
Information was a key issue in the area of fertility, with young people having a need for detailed information about their fertility preservation options and the processes involved at diagnosis.21,49,52,54,56,57,69,70,80 Five studies reported that young people had a need for this information to be tailored to their age, developmental stage, and relationship status, to be provided in a sensitive way, and to be accompanied by written/online materials and/or referral to fertility services when appropriate.56,57,59,61,69 The need for age-appropriate preservation services38,54,56,57,59 and fertility information/support for survivors was also discussed.49,56,57,73
Quantitative and qualitative studies reported that AYAs had a need for assistance with a range of difficult feelings, including fear and residual trauma, worries about family and identity, guilt, and uncertainty.22,50,67,70–72,79 Emotional support needs were most commonly reported in relation to diagnosis, decision-making and fertility, and transitioning off treatment.3,22,43,48,50,60,67,69,72 Opinions on the need for professional help varied, with articles from five studies reporting high need in this area,21,22,43,50,80 while other studies found AYAs preferred to turn to friends or family for support.70,73,74,79,81 For those wanting psychological services, access was often limited, particularly for young people in adult treatment settings and for post-treatment survivors.69,80,81
The 16 studies examining peer support needs highlighted the importance AYAs place on meeting other young people with cancer. Qualitative and mixed methods studies reported that AYAs thought peers were a source of emotional support, information about what to expect from treatment, and provided a way to reduce feelings of isolation during the transition to follow-up care.22,66,70,72,79 The preferred setting for interacting with peers depended on where AYAs were in the care trajectory with those currently undergoing treatment valuing the opportunity to mix with other young people in the ward or in waiting rooms, with these interactions a major advantage of AYA-specialist services.22,75,76,79 AYAs also reported a need to maintain connections with their existing friends, with some studies reporting a need for guidance on how best to maintain links and communicate their experiences to healthy peers.3,47,53,71,78
Only one quantitative study used a validated questionnaire to explore unmet needs. 50 This study used the adult Supportive Care Needs Survey-34 (SCNS-34) 82 that examines the presence of unmet needs in the past month.
Influence of AYA-specific treatment centers
Eight articles from six studies examined the influence of being treated at an AYA-specific treatment center on care experiences or unmet needs. Three “adequate” qualitative and one “good” quantitative article reported results only for AYAs treated at a specialist unit,50,57,76,83 while three “adequate” qualitative and one “good” quantitative article compared AYAs treated at a specialist unit to those treated in adult or pediatric settings.22,51,62,84 A qualitative study of an AYA specialist unit reported in two articles76,83 suggested that patients had a very positive experience, with the ward providing a sense of mutual support, access to experts skilled in both cancer care and working with young people, and age-appropriate information. However, both a quantitative 50 and a qualitative study 57 indicated that patients in these wards still have unmet needs. While two qualitative studies reported in three articles suggested those treated on specialist wards had better care experiences than those in other settings, including receiving age-appropriate information, information on fertility preservation, and access to recreational facilities,22,62,84 a quantitative study did not find any difference in care satisfaction levels between AYAs treated in specialist wards and those treated in nonspecialist wards. 51 However this quantitative study did find that those treated in a specialist ward were more positive about aspects of the physical setting and access to peers than those treated in a nonspecialist ward. 51
Discussion
Following an exhaustive literature search, we identified 45 “adequate” or “good” quality articles that assessed the unmet needs and care experiences of AYAs with cancer. Most commonly, studies used a qualitative methodology to examine the needs or care experiences of a heterogeneous sample of AYAs. Participants’ age varied considerably across studies, as did the time from diagnosis to study participation, with many studies reporting experiences that may have occurred up to 5 years previously. Few studies used standardized survey tools to assess either unmet needs or care experiences, and no survey tool was used in multiple studies. These features coupled with the large number of qualitative studies meant it was not possible to provide estimates of the level of unmet needs or patient experiences. However, despite the differences in study designs, general themes could be identified, which suggested the most common needs were for timely and age-appropriate fertility information and services, access to age-appropriate information, care facilities and support (including peer support), and HCPs with AYA expertise.
Previous authors have identified fertility as a key issue for AYAs,1,27 and our review confirmed that this is an area where young people, particularly young women, report unmet needs and poor care experiences. This is consistent with the conclusions by Quinn et al. that young women are more likely to report distress in relation to fertility issues. 85 The studies we examined highlighted the need for the early provision of information about the risk of infertility associated with different treatments, clear communication about fertility preservation options, and access to age-appropriate fertility services, and fertility-related follow-up after treatment. Guidelines for the care of AYAs with cancer need to ensure that fertility preservation is addressed in the post-treatment phase as well as at diagnosis and during treatment.
Another recurrent finding from the articles reviewed was the importance of age-appropriate services for AYAs, most of whom are treated in medical systems where care is divided into pediatric or adult centers. 24 The need for age-appropriate information through all stages of the cancer care journey was a common theme, with some evidence that this may be beneficial for emotional well-being. A recent review of doctor–patient relationships in 12–18-year olds also emphasized the importance of tailoring information to the young person's developmental stage, 86 while another posited a relationship between information/communication and psychosocial well-being in AYAs. 23 The need for age-appropriate emotional support was another common theme. Other reviewers have highlighted the importance of peer contact and support for psychosocial well-being.1,23,28,87 Our review suggests that AYAs should be given opportunities to interact with other young cancer patients, be supported to utilize their existing social support network, and have access to age-appropriate psychosocial services if these are needed.
Our review also found that young people express a need for treatment facilities to be appropriate to their age and a need to be treated by HCPs with AYA-specific expertise. This is consistent with other reviews that have emphasized the benefits of social, recreational and educational facilities, 79 and the potential benefits of an expert treating team for AYA adherence to treatment, survival, and psychosocial functioning.2,88 Several countries have now developed AYA-specific cancer services, which can range from independent inpatient units to multidisciplinary teams attached to adult or pediatric hospitals.1,88 It has been suggested that specialist units allow young cancer patients to access AYA-specific facilities and peer support.24,25 We found few studies that directly compared the needs and experiences of patients treated in specialist AYA settings to those treated in general pediatric or adult services. More research is needed to examine whether AYA-specific services are living up to their promise of delivering better care experiences for AYAs. If future research in this area utilized standard assessment tools and provided details of the model of care delivered, findings from different studies could be combined to allow greater understanding of the aspects of care that work to improve AYAs’ care experiences.
Our review highlighted a number of methodological issues that could help improve future research. With a median sample size of 52 participants, most quantitative studies reviewed had insufficient statistical power to examine associations between variables and large confidence intervals would be associated with any estimates found. Larger sample sizes are needed if reliable estimates of the level of need or care experiences are to be produced. Since AYAs make up a relatively small proportion of cancer patients, 89 greater collaboration between treatment settings and jurisdictions will be needed to ensure quantitative studies have adequate sample sizes. The age range of participants in the different studies was broad, with some focusing on adolescents and some focusing on young adults. There is a need for a more consistent definition of the age range that defines “AYA.” While agreeing on the age range may be controversial, 90 this is emerging as an issue with Quinn et al. identifying similar problems in the Quality of Life literature. 85 Increased use of standardized age-appropriate measures would also facilitate comparisons between studies, care settings, diagnoses, and treatment stages. Many studies we reviewed assessed care experiences that may have happened before 5 or more years for study participants. The extended period between diagnosis/treatment and assessment increases the possibility that recall bias and survival bias influence findings. Studies that assess care experiences and unmet needs closer to treatment are needed. Longitudinal studies are also needed to provide more reliable information on how patient needs and experiences change over time. Incorporating age-appropriate PREMs and PROMs into prospective clinical trials may assist in gathering longitudinal data from larger samples of AYAs while also allowing patient experiences to be related to treatment adherence and survival outcomes.
This review has a few limitations. First, we selected only those studies that obtained reports directly from AYAs. This means that the views and experiences of family members, the experiences of young people as told by their families and partners, and the views of HCPs were excluded. Second, as we included only articles published in English, research from non-English speaking countries was likely to be excluded. Third, we did not assess whether studies examined the impact of demographic factors (e.g., socioeconomic status, residential location [urban vs. rural]), on care experiences or unmet needs. As understanding whether there is equitable access to different treatment and supportive care services is important, future work is needed in this area. In addition, we did not examine the impact of age or developmental stage on care experiences or unmet needs. Finally, differences in the age of study participants, inconsistent reporting of information regarding participant characteristics, and the lack of consistent measures across studies precluded any quantification of results across studies.
Despite these limitations, this review highlights consistent themes regarding care experiences and needs from both qualitative and quantitative studies that strengthen the case for age-appropriate care for AYAs. A priority for future research is utilizing AYA-specific, standardized survey tools to evaluate specialist AYA services and determine whether they make a difference to AYAs' care experiences. Use of standardized tools would also allow results from studies of different models of care or different countries to be compared. However, as patients’ care experiences and unmet needs are only one aspect of understanding the overall quality and effectiveness of care, understanding the relationship between PREMs and more objective measures of medical and psychosocial outcomes is also needed. The AYA quality assessment measures currently under development20–22 have the potential to be valuable tools in these endeavors.
Footnotes
Acknowledgment
This work was supported by a project grant from the National Health and Medical Research Council of Australia (NHMRC) (APP1012250).
Disclaimers
The authors attest that this work is original, that they are the authors, and that it has not been published and is not under consideration for publication elsewhere.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.