
Abstract
Purpose:
Health literacy is a critical determinant of health and an emerging public health concern. Little is known about the health literacy of adolescents and young adults (AYAs) or about the ability of young patients to communicate health needs and critically evaluate information. We used qualitative methods to investigate the three aspects of health literacy (functional, communicative, and critical) in Australian AYA cancer survivors.
Methods:
Forty Australian AYA cancer survivors, aged 15–29 either at diagnosis or recruitment, participated in semistructured interviews. Participants were asked about sources of information and ability to understand information, communicate questions, and critically evaluate the validity, reliability, and relevancy of information to their situation. Self-reported adherence levels and advice for AYA-specific care was also obtained. Interviews were coded and analyzed for emergent themes using QSR NVivo 10.
Results:
Almost all AYAs named their doctor as the primary source of information. Most AYAs reported no difficulties with understanding, communicating, or assessing relevancy of information. Conversely, few AYAs reported confidence in assessment of validity and reliability of information. The doctor–patient relationship appeared to be an influential factor in all aspects of health literacy.
Conclusions:
AYAs frequently reported having a good understanding and communication around health information; however, few AYAs described engaging in critical evaluations of this information. The potential impact of the doctor–patient relationship across several domains of health literacy suggests that more focus could be placed on promoting health literacy at physician, community, and societal levels, in addition to promoting individual skills.
Introduction
H
Inadequate health literacy negatively influences numerous health outcomes, including increased hospitalizations, mortality, and health expenditure, and decreased uptake of preventative medicine.6–8 Previous research shows high levels of inadequate health literacy in adults. In one study, half of ∼30,000 American adults demonstrated low or marginal health literacy, 9 while a similar proportion of Australian adults possess health literacy levels considered inadequate to “meet the complex demands of everyday life.” 10 Adults with chronic medical conditions are particularly at risk of limited health literacy, 11 and are further influenced by socioeconomic determinants of disease, such as low socioeconomic status (SES) and educational attainment. 12
Adolescents and young adults (AYAs) undergo rapid development, improving their capacity to process information, think logically, and comprehend abstract concepts. 13 Consequently, they may be predisposed to underdeveloped health literacy skills. 14 AYAs are potentially ill equipped for healthcare autonomy at this critical stage, with lower rates of adequate health literacy among 15–19 year old Australians compared with older age groups. 10 With adolescent health behaviors predictive of adult behaviors and chronic disease risk, this time period is critical for the implementation of preventative medicine. 14
These developmental challenges may be exacerbated in AYAs with chronic disease. Relative to healthy AYAs, children with chronic diseases are expected to gain autonomy earlier, have a greater involvement in health decisions, and demonstrate a higher level of health literacy.14–16 In addition, there are often reciprocal effects of adolescent development and chronic conditions. Disease- and treatment-related demands may negatively impact school attendance and achievement, possibly contributing to low functional health literacy and decreased treatment adherence. 17 AYAs with cancer may be particularly vulnerable to the impacts of poor health literacy and treatment adherence, given their unique needs and biology of their cancers. 18 Relatively high survival rates in AYA cancer and a stable incidence over the last 10 years have resulted in a growing population of AYA cancer survivors with long-term healthcare interactions.18,19 Understanding the health literacy of AYA cancer survivors facilitates development of targeted interventions, thereby potentially improving future health outcomes.
Therefore, this study aimed to explore health literacy in Australian cancer survivors within the AYA age group either at diagnosis or interview. The current literature focuses on quantifying functional health literacy, with minimal research on communicative or critical health literacy, or qualitatively exploring health literacy.
20
This study aimed to expand on current knowledge by capturing how survivors described health literacy-related experiences, rather than seeking to quantify their health literacy levels. We also sought to understand the role of health literacy in the broader context of their healthcare. Specifically, the following three questions were addressed:
1. What were the sources of cancer information used by AYAs? 2. What were the barriers and facilitators to functional, communicative, and critical health literacy, and treatment or appointment adherence? 3. What recommendations did they have for clinicians regarding AYA-specific care?
Methods
Participants
This study was part of a larger study examining autobiographical disruption in AYA cancer survivors. 21 Eligible participants (1) were aged 15–29 at treatment or study recruitment; and (2) completed cancer treatment up to 5 years before interview. Survivors of both pediatric and AYA cancer were eligible.
Ineligible participants (1) had insufficient English skills to complete the interview; and/or (2) demonstrated severe psychological distress (i.e., disclosed suicidal intent, symptoms of psychosis or substance abuse, or scored >28 on the depression subscale of the Depression, Anxiety, Stress Scales-Short Form [DASS-21]). 22
Interview
We used a qualitative methodology to provide a comprehensive examination of health literacy, as suggested by Manganello. 14 Three psychologists (U.S.D., C.W., and B.M.) developed the semistructured interview, which aimed to explore all aspects of health literacy during the AYA years. Participants who were younger than 15 during treatment were encouraged to discuss healthcare encounters during their AYA years (e.g., during long-term follow-up clinics). Questions were based on Nutbeam's model of health literacy, 5 and centered on information sources, functional, communicative, and critical health literacy, as well as treatment or appointment adherence. Advice for AYA friendly care was also solicited. Table 1 shows the interview schedule.
While additional information was obtained from a questionnaire and another semistructured interview for the overarching study, only data relevant to the current study are reported here.
Procedures
This study received institutional ethics approval before commencement. Potential participants were identified through the Sydney Youth Cancer Service and long-term follow-up clinic at Sydney Children's Hospital, Randwick. We implemented our Standard Operating Procedure 23 to exclude ineligible or deceased participants.
We mailed study packages (containing study and eligibility information, a consent form, and a questionnaire) to prospective participants. Upon return of consent forms, a research officer telephoned participants to confirm eligibility and schedule interviews.
Interviews were conducted by two registered clinical psychologists (U.S.D., B.M.) and lasted ∼20 minutes. Consent for audio recording was gained at the beginning of each interview. Participants entered a draw for a $200 gift voucher, but were not otherwise reimbursed for involvement.
Data analysis
Data collection and analysis were guided by the conceptual framework of Miles and Huberman. 24 Interviews were recorded and transcribed verbatim and then analyzed using QSR NVivo 10. The coding tree was developed by two authors (M.L., U.S.D.), with top-level nodes based on the Nutbeam model and our research questions, and emergent themes designated as child nodes. We used counts and cross-tabulations to identify and quantify emergent themes. Participant discussion relating to top-level nodes was coded as “negative” or “positive” (i.e., did or did not have difficulty, respectively), and child nodes categorized separately under “barriers” or “facilitators.”
We hypothesized that several demographic variables (age at diagnosis, SES, and education level, stratified as presented in Table 2) could affect health literacy. We examined differences in qualitative data (e.g., the proportion of positive and negative health literacy experiences described) between these subgroups a priori to identify systematic differences.
Demographic data were missing for three participants.
SEIFA is an Australian index of relative socioeconomic advantage and disadvantage, and is based on postcode. This particular split was chosen as it almost equally divided our sample into relatively advantaged and disadvantaged.
Highest level completed year 10 or 12.
Includes TAFE, apprenticeships, and those still at university.
CNS, central nervous system; SD, standard deviation; SEIFA, socioeconomic indexes for areas; TAFE, technical and further education.
Results
Study population
We identified 352 potential participants, of which 209 were unreachable. The remaining 143 participants received packages, of which 60 were recruited into the larger study, with 43 opting into this study. Three of these participants were lost to follow-up, for a final 40 (28%) participants. Further details are provided in Figure 1.
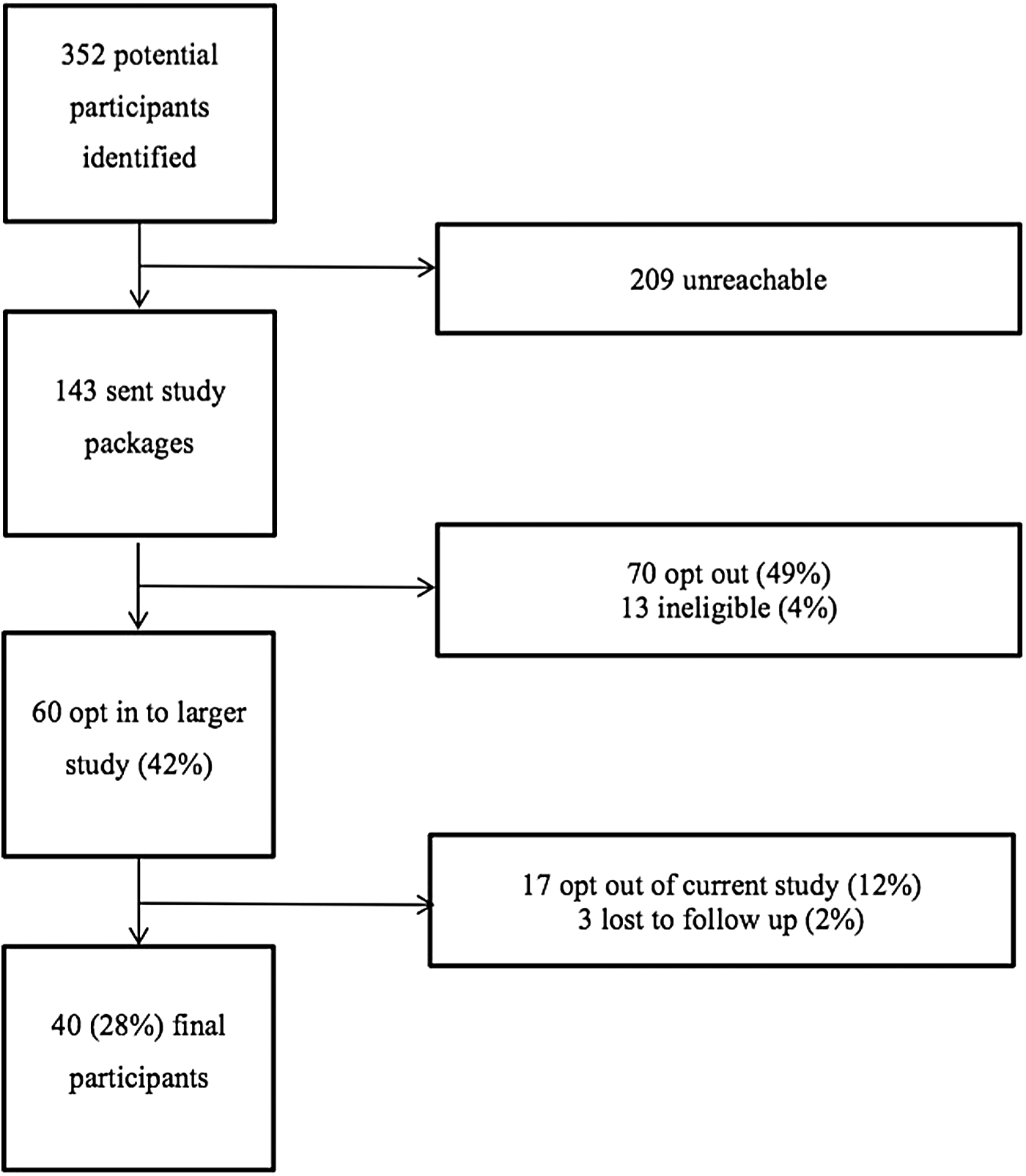
Recruitment process.
Of the 40 participants, half were male (n = 20). Age at interview ranged between 17 and 31 (mean 22.9, standard deviation [SD] = 3.50), with a mean age of 10.7 at diagnosis (SD = 6.07, range 5 months–22 years). Approximately two thirds (n = 27) were younger than 15 at diagnosis. Table 2 outlines further demographic characteristics of the sample.
While we hypothesized that the data would differ between the demographic subgroups described in Table 2, we found few systematic differences. Hence, reported results are for the whole sample (n = 40). As questioning was variable and guided by participants' previous answers, percentages relate to participants who discussed each theme.
Sources of health information
The most commonly reported sources of information were healthcare professionals. Almost all AYAs reported receiving their information from doctors (n = 32); “it would've come …95% from my doctor” (Male; 14 years at diagnosis, 29 at interview). Table 3 provides further illustrative quotes from participants. Nurses (n = 10) were another common source of information, with one participant stating, “the majority…was from my CNC [clinical nurse consultant]” (Male; 16, 20). Other healthcare professionals (n = 7) and parents (n = 8) were also frequently consulted.
Other information sources included informational pamphlets (n = 6), books (n = 5), and the internet (n = 7). Ten AYAs specifically reported avoiding the internet.
“They said early on not to use the internet.” (Male; 17, 31)
“You couldn't really put any reliance into net [sic] sources.” (Female; 13, 25)
Functional health literacy
AYAs' reported ability to understand information was varied, with most AYAs describing no difficulties (n = 20/31; 65%). The information was often perceived as being “not really hard to understand” (Female; 9, 21) because “the doctors would always explain things well to me” (Male; 20, 22).
However, other AYAs reported struggling with terminology and pacing of information (both n = 7). Participants described doctors using “big scientific words” (Female; 14, 26) and “all this scary language which as a 14 year-old, I didn't understand” (Female; 14, 20).
“I don't want to think about that right now… Or like, I'm not really at a point in my life where I feel like I have to think about it…Yeah, I suppose the, like the issue of, ‘do I really want that information right now?’ and it's just like, ‘here it is…’” (Female; 1, 24)
“It was just so much information and…I was still in shock.” (Male; 15, 17).
AYAs also reported that clinicians misjudged development levels.
“I got really frustrated with people like talking to me like a little boy.” (Male; 8, 26)
Communicative health literacy
Most participants reported no concerns with asking questions (n = 31). The main facilitator was a strong doctor–patient relationship (n = 16).
“I think the doctors just did a fantastic job with me and helped me to understand everything that I needed.” (Male; 20, 22)
“I guess we had that long-standing relationship…I felt a bit more comfortable because he was the one regular person that I went to see so I felt ok asking him certain questions.” (Female; 5 months, 27)
Other facilitators included being “not scared to ask” (Female; 9, 20) or having the right personality (n = 5).
“I suppose I'm a confident person. I'm not scared about putting out my own opinion or asking questions.” (Male; 20, 22)
Perceived barriers to communicative health literacy included a poor relationship with their doctor (n = 8). Doctors were often “on a cycle,” making it “really hard to build up a relationship with them” (Female; 22, 23).
“I have a different doctor every time that I go…I feel like I'm talking to a stranger, so I find it very hard to talk about anything in detail.” (Female; 1, 24)
In addition, AYAs described some doctors' poor interpersonal skills, such as not feeling “like they have an open person treating them, that's willing to let them ask the questions” (Female; 11, 21).
Five participants reported being uncomfortable with asking questions. Another five participants had unanswered questions (primarily regarding late effects), despite not expressing difficulties with asking questions.
Critical health literacy
Slightly more participants reported not assessing relevancy of information, compared with those who did (n = 21 vs. 16). Nontailored information was the main reason for assessing relevancy (n = 7).
“Sometimes the information that they give the people at the hospital is quite generic…and you kind of have to pick apart what parts are relevant for you.” (Male; 11, 21)
Most AYAs did not assess the validity or reliability of information received, chiefly because they trusted their doctor(s) (n = 22/31; 71%).
“I trusted them because they really did seem like they knew what they were doing.” (Female; 19, 23)
“It's not like you're going to question a doctor or a nurse or something.” (Male; 17, 21)
Of those who analyzed validity or reliability (n = 9), almost all were checking sources other than doctors (n = 8/9; 89%).
“When I was reading it online, I don't trust anecdotes from people, like, one place isn't reliable.” (Male; 20, 22)
Adherence
A third of our participants considered skipping appointments or treatment (n = 12/33; 36%). Of these, four acted on their desires. They described multiple motivations for adherence, including parental influence, and necessity for survival (n = 7 and n = 9, respectively).
“Mum was pretty on it,” (Female; age at diagnosis unknown, 18)
“This is the only thing that's going to save my life,” (Male; 11, 21)
The principal barrier to adherence reported was treatment intensity and side effects (n = 9).
“I was having three doses of chemo and then a week later I was having another two doses and it was just really full on.” (Female; unknown, 18)
“I went to this stage where I just wanted to not do chemo anymore…I was just sick of it.” (Female; 15, 17)
Suggestions for healthcare professionals
The main suggestion for AYA-specific care was provision of support (n = 11), especially peer support (n = 4). Participants reported that they “want someone, relevant to their age” (Male; 17, 21) who “you could talk about your treatment and sort of help each other” (Female; 18, 22).
Participants approved of pediatric and adolescent-specific services (such as Starlight Rooms, which are “medical-free havens” present at Australian pediatric hospitals) 25 that allowed them to “disconnect from what was really happening” (Male; 12, 22) (n = 4).
“There are a lot of things…that distracted me from the fact that I was in hospital. I remember getting to play on a Nintendo, and that was a big rush.” (Male; 9, 26)
Another common suggestion was for developmentally appropriate communication (n = 11). Participants called for clinicians to be genuine and involved during interactions with patients.
“There were people who…spent half the time scribbling notes and dot-points and stuff. And then there was someone who would actually come in and sit on the bed and ask you how your day was and like those were the ones you really liked and enjoyed talking to.” (Female; 16, 26)
Discussion
Overall, AYAs described being confident in the domains of functional and communicative health literacy, but reported lower rates of critical analysis. This is consistent with Nutbeam's hierarchical model, with the separate constructs building on each other. The varying levels of confidence are also expected given that social and communication skills are acquired during adolescence, while critical analysis skills continue developing beyond adolescence. 13 The finding that AYAs are confident with functional and communicative health literacy is reassuring, especially given research linking higher functional literacy with greater patient satisfaction. 26
Doctor–patient relationship
The impact of the doctor–patient relationship was described across all domains of health literacy, in accordance to past research. 27 Indeed, many of the other barriers or facilitators of health literacy (e.g., use of jargon) are contributors to AYAs' perceptions of the relationship. While the doctor–patient relationship has been previously identified as a factor to AYA adherence, this was not reported by our participants. 28
The apparent influence of the doctor–patient relationship suggests that developing rapport and improving communication skills may improve health literacy. Improving the doctor–patient relationship in adolescent cancer settings requires involving AYAs in treatment decisions, providing developmentally and culturally appropriate information, and utilizing appropriate communication methods. 29 AYAs with chronic conditions also consider other factors to be vital, such as advocacy, competency, confidentiality, privacy, and a holistic approach to the patient.30,31 Confidentiality appears to be particularly influential,30,32 as adolescents are more likely to access healthcare or disclose risky health behaviors when confidentiality is ensured.33–35
There are also important theoretical implications. Until recently, definitions of health literacy focused on the skills and abilities of the patient, to the exclusion of the broader environment in which health literacy processes take place. 36 Frameworks are evolving to reflect the importance of external factors; however, a greater emphasis on societal factors is required for a holistic approach to health literacy. 37
Digital health resources
The internet was not a primary source of information for our participants. This finding is in contrast with previous literature and despite the central role the internet holds in AYA lives: more than 80% of Australian 14–17 year olds consider it very or extremely important, with 70% accessing it daily.26,38,39 Furthermore, exposure to credible online health information positively correlates with health literacy, while internet use in cancer patients may lead to more active decision-making.40,41 Digital methods of communication can improve patient communication without affecting physician productivity, 42 while new technologies (e.g., smartphone applications) can be used to supplement traditional sources of information. 43
Given their potential as a health literacy facilitator, importance in AYAs' lives, and wide accessibility, it may be beneficial to promote the use of the internet and other digital resources. However, the barriers cited by participants—primarily reliability and physician disapproval—warrant acknowledgment. In particular, reliability is widely variable and studies show a dearth of reliable online information.44–47 Therefore, the overall reliability of online health resources needs to be developed and promoted.
Provision of support
Our AYAs described the need for improved psychosocial support, reinforcing past research. 48 The perceived lack of peer support may be important given community-based peer support can promote health literacy. 49 In addition, peer support is often particularly influential in AYAs, more so compared with parents or other adult figures. 13 Therefore, the effect of peer support on health literacy warrants further investigation.
Strengths and limitations
This study thoroughly explored health literacy in Australian AYA cancer survivors. It extended upon existing literature by examining communicative and critical health literacy, which has often been previously unexamined. 50 Our qualitative methodology allows characterization of these new concepts.
However, several limitations warrant acknowledgement. With a recruitment rate of 28%, the generalizability of these results may be limited. The recruitment rate also may reflect a self-selected sample. We speculate that participants with stronger communication skills and higher education levels were more likely to opt in, particularly given the requirement of two interviews and a long questionnaire. With focus on the impact of cancer, participants with more intense experiences (either positive or negative) may have also been more likely to contribute. The length of time between active treatment and interview for many of our participants may also exacerbate the existing limitations of retrospective research and recall bias. Other limitations involve the self-report nature of this study and the modest sample size.
Conclusion
This comprehensive qualitative study is expanded upon current literature by characterizing the experiences of Australian AYA cancer survivors across a range of health skills. Our findings highlight the importance of quality doctor–patient communication. We identified other barriers and facilitators for health literacy, including jargon use, inappropriate information delivery, and reliance on doctors. Larger studies building on the foundations of this qualitative work will be critical to develop AYA health literacy.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Eden Robertson in coordinating recruitment and data collection to this study, as well as Sarita Herse, Kate Marshall, Emily Spencer, Julie Ta, and Nicole Weavers.
Author Disclosure Statement
Ursula Sansom-Daly is supported by an Early Career Fellowship from the Cancer Institute NSW (ID: 14/ECF/1-11) and an Early Career Fellowship from the National Health and Medical Research Council of Australia (APP1111800). Claire Wakefield is supported by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1067501) and an Early Career Development fellowship from the Cancer Institute NSW (ID: 11/ECF/3-43). The Behavioural Sciences Unit is supported by the Kids with Cancer Foundation. Neither the Cancer Institute NSW, the National Health and Medical Research Council of Australia, nor the Kids with Cancer Foundation played any role in the design and conduct of the study; data collection, management, analysis, or interpretation; preparation, review, or approval of the article; or the decision to submit the article for publication.