
Abstract
Adolescents and young adults (AYA) face individual and social challenges different to other age groups that shape their experience of cancer and the associated psychological distress. This critical review examined the availability of AYA-specific psychosocial interventions to assess the impact they have and identify elements that make them successful. Five literature databases were searched for psychosocial intervention studies involving AYAs with cancer, on and off treatment, aged 10–30 years, published between 1980 and 2016. Eleven out of 42 identified studies were included in the final review after quality assessment. All but two interventions showed positive results on at least one measure of psychosocial well-being. A distinctive difference between the supportive needs of those on and off treatment was noted, and differences in intervention design and delivery formats were identified between the two subgroups. Analysis of specific intervention characteristics that achieved the successful outcomes was more challenging due to the large variation in outcome measures used. This review demonstrates that psychosocial intervention research for AYA with cancer is increasing and the results show a potential benefit of intervention participation. Further work is needed to validate whether the benefits achieved by intervention participation remain over time.
Background
C
Adolescence is associated with a range of unique challenges, including peer pressure, progression in education and employment, development of identity, formation of relationships, and sexual maturity. A diagnosis of cancer during this period further compounds this already challenging time. Both the disease and its treatments cause physical pain, lethargy, limitations to daily functioning, social isolation, and changes in appearance and relationship dynamics.3,4 While all of these factors might be considered stressful at any age, it is more so for young people who face additional challenges and disruptions during such a developmentally critical time period. 5 Adolescents diagnosed with cancer are therefore at a higher risk of developing psychological problems, both during and after treatment, with reports of lower QOL and self-esteem when compared to peers. 6 Furthermore, increased diagnoses of mental health problems, such as anxiety and depression, have been reported in AYAs diagnosed with cancer. 7
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) published 14 quality statements aiming to contribute to quality improvements within the care of children and young people with cancer. 8 This included the need for children and young people, as well as their families, to have their psychological and social needs assessed throughout their cancer journey and receive support based on their individual needs. Due to the acknowledged “gap” in AYA research,9,10 the evidence base supporting the application of psychosocial support in clinical practice specifically for AYA with cancer is minimal and evidence-based psychosocial interventions are rarely provided as part of routine care.
A review reporting interventions aimed at reducing cancer-related distress in adolescents included four studies and concluded that there was an absence of psycho-oncological intervention research with adolescents. 11 The results of the studies in this review were varied, with only one study reporting significant improvements in psychosocial well-being. 12 A later review 13 examined interventions aiming to improve psychosocial well-being in AYA with a range of long-term conditions, including cancer. Of the 25 studies in this review, only 7 included cancer patients. The review found that the majority of studies demonstrated an encouraging improvement on at least one psychosocial outcome measure and they found evidence to suggest that skills-based interventions achieved the greatest improvements. However, results were inclusive of all long-term conditions and subgroup analysis of cancer patients was not conducted. It is therefore difficult to know if the conclusions are applicable to young people with cancer. The number of studies, including cancer patients, has increased since the first review, 11 suggesting a growing interest in this field of research, indicating priority for a further review to be undertaken.
The aims of this review were as follows:
• Identify intervention studies specifically aiming to improve psychosocial well-being in AYA with cancer. • Evaluate the benefit of interventions, demonstrated by an improvement on a recognized measure of psychosocial well-being. • Identify specific characteristics of the interventions that are successful in improving psychosocial well-being to guide future studies within the field.
Methods
Data sources and search strategy
The literature review was guided by search terms published previously 13 and included terms related to population, intervention, and outcome (Appendix). The search was conducted on electronic databases (MEDLINE, PsycINFO, CINAHL, and EMBASE) from 1980 until May 2016. A search of gray literature was also conducted using the PsycExtra database for the same time period. Finally, a hand search was conducted using the references of identified studies. The two earlier reviews11,13 only included randomized control trials (RCTs). As they identified a small number of eligible studies and highlighted that an RCT may not be the optimal study design to evaluate a complex intervention, 14 it was decided to allow the inclusion of multiple study designs.
Eligibility criteria and study selection
Studies were eligible for inclusion in the review if they
• Reported an intervention that aimed to improve psychological or social well-being evaluated through reporting the use of a psychosocial outcome measure. Psychological and social well-being was defined broadly as the way a person thinks and feels about themselves and others, including being able to adapt and deal with daily challenges while leading a fulfilling life (e.g., this included measurements of QOL, anxiety, coping, social support but excluded clinical/medical outcomes, such as toxicity and adherence). • Included young people with cancer aged 10 to 30 years.11,13 If the intervention involved children or older adults, studies could be included in the review if the AYA data were presented separately. • Published in English, Spanish, or Portuguese in a peer reviewed publication (reflecting the expertise of the review team).
Studies were excluded if
• The intervention aimed to improve psychosocial well-being in groups other than AYA cancer patients (e.g., parents, although studies that aimed at young people but also provided support to family members were included). • The intervention included young people with a diagnosis other than cancer, unless the results for the AYA cancer population were reported independently. Review of titles, abstracts, and full-texts of search results was conducted by one reviewer, which was independently reviewed by a second. Three reviewers extracted information from eligible studies directly into a spreadsheet to ensure that identical information was reviewed. This was cross checked by a fourth.
Methodological quality
An assessment of methodological quality of studies meeting the eligibility criteria was conducted using either the Consolidated Standards of Reporting Trials (CONSORT) 15 or the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 16 critical appraisal instruments. The percentage of criteria that was fulfilled was calculated for each study and studies were classified as Q1 (achieved >75% of quality criteria), Q2 (fulfilled 50%–74% of quality criteria), or Q3 (<50% of quality criteria achieved). Studies rated Q1 and Q2 remained eligible for synthesis of results.
Method of synthesis
Four reviewers independently reviewed the results. Due to the abstract nature of the concept of psychosocial well-being, there was no uniformity in study outcomes in the eligible studies. Further examination of the outcome measures used showed that a total of 17 aspects of psychosocial well-being were assessed (Table 4), with many studies using multiple instruments. It was therefore not possible to group outcomes together for analysis, and so, a sign test was used to display the effect of the intervention on each individual outcome, with a plus sign indicating a significant positive effect on psychosocial outcomes, a minus sign suggesting a significant worsening, and an equal sign showing no significant difference.
Results
Identification of studies
Of the 1632 articles that were identified in the search, a total of 18 fulfilled the inclusion criteria (Fig. 1).12,17–33 The 18 studies represented 26 years of psychosocial intervention research in AYA with cancer. The majority of studies were conducted in the United States (n = 13), with others hosted in Hungary, Taiwan, Canada, New Zealand, and Israel. Eight studies were RCTs and the remaining ten utilized a nonrandomized trial design (Table 1).
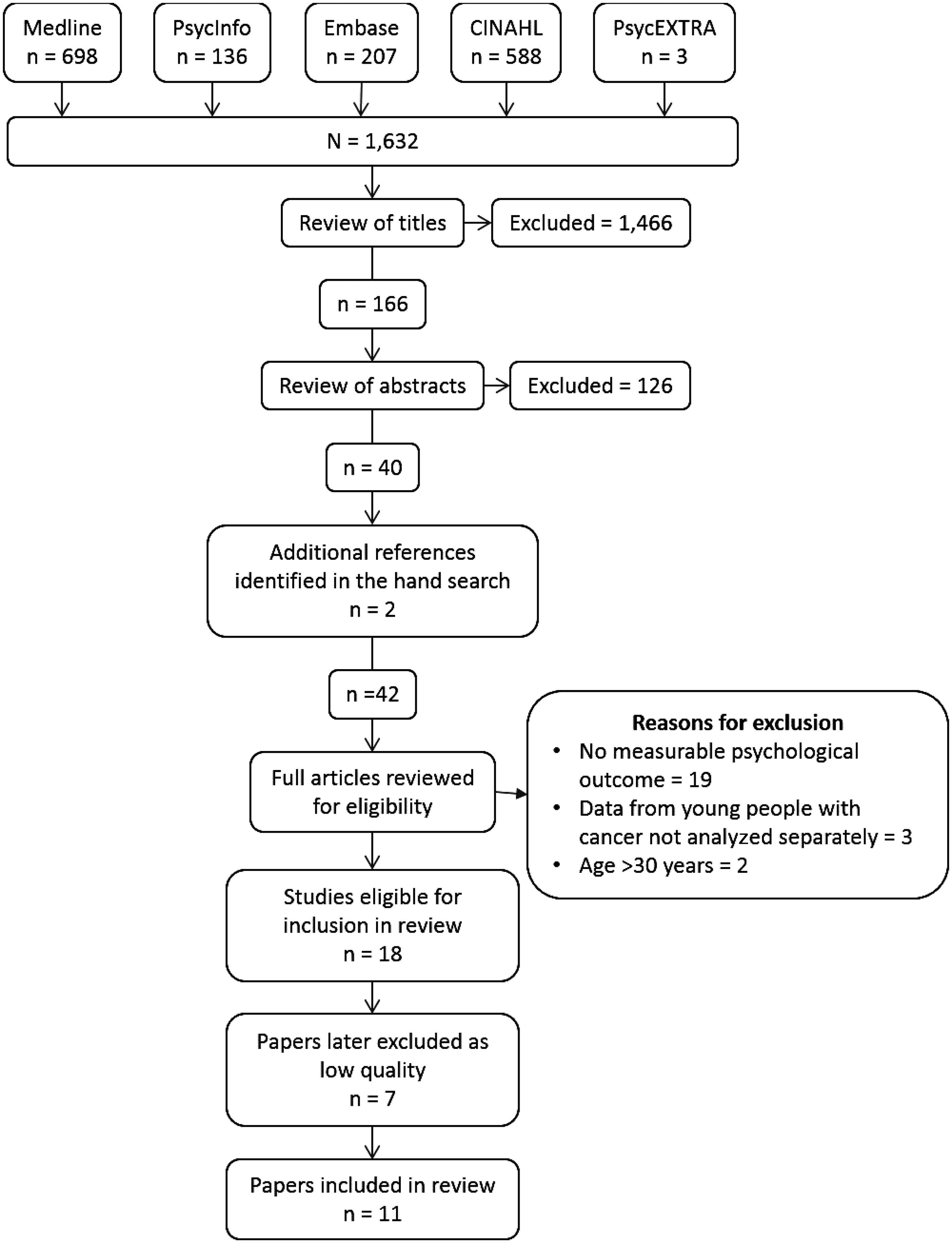
Flowchart showing the number of published articles selected and excluded from the database searches through to the publications included in the review.
Scored according to fulfillment of percentage of critical assessment tool criteria (CONSORT/STROBE): Q1 = >75%; Q2 = 50%–74%; Q3 = <50%.
ACP, advanced care planning; AYA, adolescents and young adults; RCT, randomized controlled trial; TYA, teenage and young adult; QOL, quality of life.
Assessment of study quality
Five studies scored as high quality (Q1), six were moderate quality (Q2), and seven were identified to be of poor quality (Q3) (Table 1). Common areas of weakness included the following: non-RCTs not describing the setting/location of the study12,17,19–21,26,30,31,32; not specifying how the sample size was derived12,17–20,24,26,28,30,32,33; including a low number of eligible participants12,25,27–29,31; not providing details of missing data23,27–29,32; and not providing complete details of the randomization process in an RCT.12,17–20,22,23,25,27 However, there were areas that were consistently reported well, including the scientific rationale and objectives12,17–23,25–33; clear definition of the outcomes (although the primary outcome was often not identified, see Table 3)12,17–23,25,27–33; and detailing the methods of analysis.12,17,22,25,27–33
The 11 studies with quality scores of Q1 and Q2 were included in the final review to ensure that recommendations were based on only high-quality evidence (Tables 2 and 4).
The number in the article does not add up to the total number of participants.
ALL, acute lymphoblastic leukemia; CNS, central nervous system; HD, Hodgkin's disease; ns, not stated; na, not applicable because patients self-referred to join the study.
Study characteristics
Eligible studies included interventions aimed specifically at improving the psychosocial well-being of young people on-treatment (n = 7) or interventions to support young people off-treatment * (n = 2). Undoubtedly, both groups face psychosocial challenges; however, the life events and psychological and social issues facing each group are often described as different and unique. It was therefore decided to present the synthesis of results separately. Two studies included young people both on and off treatment and were therefore included in both sections.12,30
Psychosocial interventions for young people on-treatment
The nine studies reporting interventions to support AYA on-treatment12,20,22,25,27–29,30,33 included a combined total of 754 participants aged 9–29 years, ranging from a sample size of 10 to 375 participants (Table 2). Sample size was supported by a statistical calculation in four studies.22,25,27,29 The study by Wu et al. 27 was included in the review because the majority of young people were within the specified age range (personal communication). All but four studies12,20,30,33 included a higher proportion of males; eight were not tumor specific (cancer type was not specified in one 25 ).
Eight studies aimed to address the psychosocial impact of cancer treatment by improving cancer knowledge and coping abilities12,20,22,25,27,28,30,33 and one specifically focused on the psychological impact of premature confrontation with morbidity 29 (Table 3). A variety of different intervention styles were utilized, including a combination of activities and counseling (n = 1) 12 ; specific skills training sessions (n = 3)20,27,33; and activity-based interventions (n = 5).22,25,28–30 Two interventions were delivered through computers22,25 and the remainder were face-to-face (n = 7)12,20,27–30,33 involving the individual (n = 8)12,20,22,25,27,29,30,33 and the family (n = 1). 29 Of the face-to-face interventions, one was a one-off event 20 and six consisted of multiple sessions delivered over a number of weeks.12,27–30,33 Three of the interventions were delivered by specialist trained therapists,12,28,29 one by a trained instructor 30 and two by research assistants.20,27
Outcomes in bold are primary outcomes. Canada et al., Hinds et al., Jones et al., Lyon et al., Schwartz et al., Hooke et al. did not state which outcomes were primary/secondary.
Psychosocial interventions for young people off-treatment
The four studies reporting interventions to support young people off-treatment12,19,30,31 included a total of 53 young people aged 10–29 years at the time of participation (Table 2). The age at diagnosis was reported in two studies,12,19 mean 11 years (SD = 3.8) and time since treatment was completed ranged from 4 months 12 to mean 9.3 (SD = 6.1) years. 19 Four studies included a range of diagnoses.12,19,30,31
One concentrated on psychosexual development following cancer, 12 two studies on physical activity, education, and coping,30,31 and finally, one study aimed to improve overall QOL 19 (Table 3). Intervention methods included activity based (n = 3)19,30,31; and a combination of activities and counseling (n = 1). 12 All the interventions were delivered face-to-face. Delivery of the intervention was in groups (n = 3)19,30,31 or individually (n = 1). 12 One was delivered as a one-off event, 19 one consisted of two sessions with additional work to be undertaken between sessions in the participant's own time, 12 and two involved 6 to 16 weekly sessions.30,31
Synthesis of findings
Irrespective of whether the intervention was aimed at young people on- or off-treatment, all but two interventions27,33 had a positive effect on at least one measure of psychosocial well-being (Table 4). For those studies focusing on young people off-treatment, benefit was found in all the outcomes measured.12,19,30,31 In two studies, no positive effect was reported due to recruitment difficulties and small sample size.27,33
Shading highlights primary outcomes.
At end time point but not earlier follow-up times.
Decreased levels of anxiety for both intervention and control groups from baseline to 3-month assessment.
Postintervention but not maintained at 3- and 12-month follow-up times.
Improved QOL postintervention, although this was not maintained over 3 months of follow-up, due to a response shift (the covariance structure was used to evaluate changes in the meaning of QOL between survivors and controls, showing the weekend intervention brought survivors' conceptualization of QOL closer to that of their age cohort).
Improvement in anxiety scores was significant for participants aged 10–12 years and showed a trend for improvement in participants aged 13–17 years (not significant).
Most studies used multiple outcome measures assessing different aspects of psychosocial well-being. Five studies specified their primary outcome,22,27,29,30,33 of which only one study by Robb et al. 29 used a psychosocial measure as the main endpoint for a psychosocial intervention study. Only one study showed significant improvement across all measures. 12 Even when the same outcome measures were utilized across studies, findings were varied. For example, the findings by Jones et al. 25 showed no improvement in self-efficacy, whereas the findings by Kato et al. 22 did. All the studies measuring symptom distress and resilience reported no significant benefit20,29,33 and the majority, including a measure of QOL, also found no benefit of intervention use.22,25,27
Discussion
This review aimed to identify studies specifically aiming to improve psychosocial well-being, to evaluate the benefit of interventions, and to identify which characteristics make an intervention successful in improving psychosocial outcomes. The review reporting in 2009 focused solely on AYA with cancer examining the availability of psychosocial interventions and identified only four studies and concluding that the use of evidence-based interventions with this population was rare. 11 This current review identified 18 studies, which may, in part, be due to the inclusion of trial designs other than RCTs and it may also suggest a growing interest in psychosocial intervention research undertaken with young people who have cancer. Also promising and clinically relevant is the finding that most studies demonstrated a positive effect of intervention participation. However, this observation is based on the fact that most studies used multiple outcome measures with no or little discrimination of the specific benefit of the intervention.
Synthesis of results was challenging due to the variety of outcomes and measures used. What was surprising was how few studies specified a psychosocial endpoint as a primary outcome. Also, inclusion criteria very rarely required screening for psychological pathology. While most studies showed a positive effect, the specificity of benefit was more so for those young people off-treatment where there were improvements in both primary and secondary outcomes. This may reflect the greater need for interventions when treatment has finished as young people on treatment focus more on the physical demands of treatment. 9
Only one study achieved significant improvements on all the psychosocial outcomes measured. 12 In fact, the interventions aimed specifically at young people off-treatment appeared to have more demonstrable benefits overall in comparison with those designed for patients on-treatment. For example, all the studies involving young people off-treatment and using QOL as a measure of psychosocial outcome showed improvements, while QOL did not improve in any study with young people on-treatment. Similarly, anxiety was reduced in young people off-treatment following interventions, but there was no improvement in those on-treatment. These results are not necessarily suggestive that interventions are more beneficial for young people off-treatment than those on-treatment; it may be that these are not realistic outcomes to measure during treatment as many other mediating factors, such as the demands of treatment, may be influencing perceptions of psychosocial well-being. In addition, problems relating to psychosocial well-being may be more of a priority for young people off-treatment than for those receiving active treatment, who maybe more focused on physical health.
Interventions aimed at improving psychosocial well-being remain an important aspect of care for young people on-treatment, but the long-term benefits when treatment ends cannot be ascertained because current research only evaluated short-term outcomes.
Interventions to support psychosocial well-being had a range of designs, aimed at different aspects of psychological well-being, and were delivered in different ways. This made direct comparisons difficult; however, some key differences in intervention formats were acknowledged between those targeting young people on- and off-treatment. First, interventions designed for young people off-treatment were more likely to be group or family based; in contrast, those designed for young people on-treatment were mainly focused at the individual level. Off-treatment interventions involved a counseling/reflective methodology or focused on physical activity to improve well-being, while on-treatment interventions involved more skills training or were activity led. Furthermore, interventions designed for young people on-treatment tended to be aimed at improving general coping with a cancer diagnosis and managing cancer treatment, whereas interventions for those off-treatment were more tailored to specific areas of psychosocial well-being affected by a cancer diagnosis.
It is interesting to note that the majority of studies focus on young people during treatment, yet young people report that many of the psychological challenges they experience occur when treatment ends. 9 When young people are receiving treatment, they are more likely to have equal access to all the services that are available, but when treatment has ended and they are discharged from secondary care, young people are reliant on primary care providers to access psychological care. Often the availability of psychological/emotional support is limited, and therefore, young people have to wait protracted time periods before receiving any targeted therapy. 9
Issues relating to the choice of outcome are a common limitation of current evidence. In part, this may be due to the complexity of the outcome being investigated; “psychosocial well-being” is a broad term encompassing a range of different factors such as QOL, anxiety, depression, support, coping, and stress, which can be challenging to measure quantitatively. 35 An added challenge for intervention research is to achieve congruence between the aims and design of the intervention and the choice of outcome. Selection of the appropriate instruments to demonstrate an effect of the intervention while ensuring young people understand the questions in the outcome measure and that they are of relevance to them might be difficult.
Furthermore, there are currently only a limited number of psychosocial measures that have been validated for use within the AYA age range, spanning the traditional child/adult age continuum. 36 The extent therefore to which reliable and valid conclusions can be drawn from work using unvalidated measures is limited. As noted previously, young people with cancer face a unique set of age-specific individual and social challenges that shape their experience of cancer and subsequently psychological distress, and therefore, measures that have been devised for the child or adult cancer population may not be transferable to this age group. A recent review of psychosocial measures for use with AYA with cancer identified seven instruments that were reliable and validated for this population. 36 Despite the studies included in the review using a range of between 3 and 11 outcome measures per study, only three studies incorporated the instruments found to be valid for use with this population.22,28,29 The limited number of validated measures within the psychosocial domains impacts on researchers' abilities to measure change in psychological or social well-being, which is a further limitation of current intervention research within this age group. A final limitation highlighted in the current review was the number of studies that did not differentiate between the primary and secondary outcomes or specified multiple outcomes as being primary outcomes.
Although Sansom-Daly et al. 13 concluded that skills training appeared to be a beneficial characteristic of intervention success, little can be concluded from this review regarding the efficacy of specific intervention designs due to the heterogeneity of outcomes. Future intervention development research needs to focus on optimizing knowledge regarding who (group/individual), how (face-to-face/web based), and format (skills based/reflection). More attention to theory in the development of interventions will also guide the primary outcome measure. Many studies administered a battery of instruments; if every aspect of psychosocial well-being is measured then by the process of elimination, something will show a significant improvement. For example, a single study 29 measured eight different aspects of psychosocial well-being, yet benefit was only found for social integration, coping, and family environment; furthermore, this benefit was not apparent across all measurement time points. Administering multiple instruments has the added limitation of decreasing acceptability to young people and consequently can result in participant dropout and missing data. 37
Two further concerns that have not been addressed in the literature are the issues of the length of follow-up and cost-effectiveness. The longest follow-up time in the studies identified in this current review was 1 year, with the majority of studies ending at 3-month follow-up. This is a short amount of time to assess impact of an intervention in improving psychosocial outcomes, especially for young people on-treatment, where treatment may be ongoing for a number of months and late effects may not be apparent until 5 to 10 years later. Furthermore, only assessing benefit in the short term will not show the sustainability of effectiveness. This leads to the second concern, the omission/absence of economic evaluation to show the cost-effectiveness of interventions. Many of the interventions were resource intensive requiring the input of trained professionals and therefore to be implemented as standard care; healthcare providers will need cost–benefit evidence to influence implementation.
Conclusions
This review has identified that the body of research addressing psychosocial interventions for AYA with cancer is expanding, and the evidence suggests that interventions are beneficial in relieving some aspects of psychological distress. Two subpopulations were identified and different intervention designs were utilized to address their different psychological and social concerns. Further work is needed to identify the most successful characteristics of psychosocial interventions for AYA with cancer. However, it may be that different characteristics are successful for different subgroups or at distinguishing between and improving different elements of psychosocial distress.
Footnotes
Acknowledgments
R.M.T. is funded through an NIHR Programme Grant for Applied Health Research (Reference RP-PG-1209-10013). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Author Disclosure Statement
No competing financial interests exist.