
Abstract
Purpose:
Childhood cancer is stressful for the entire family. Preoccupation and anxiety surrounding the child's illness may result in parents of children with cancer being overprotective or less emotionally responsive toward their children. Such parenting in response to a negative life event like childhood cancer may cause survivors to be more insecurely attached than healthy peers, which could have downstream effects on survivors' romantic relationships later in life. Therefore, we examined survivors' perspectives on parent behaviors, adult attachment, and marital status among adult survivors of childhood cancer relative to controls.
Methods:
One hundred forty-nine young adult survivors and 149 matched controls (Mage = 28, range 20–40) indicated their relationship status (single vs. partnered) and completed standardized questionnaires assessing memories of upbringing (warmth, overprotection, rejection) and adult attachment (avoidance, anxiety).
Results:
Adult survivors of childhood cancer remembered mothers and fathers as emotionally warmer (d = 0.53/0.30), and mothers as less rejecting than controls (d = 0.30). Adult attachment was overall similar between survivors and controls, but partnered survivors reported particularly low attachment-related anxiety. Childhood cancer was related to higher mother and father warmth, which were associated with lower attachment-related avoidance and in turn with a greater likelihood of being in a relationship.
Conclusion:
Adult childhood cancer survivors did not remember their parents as overprotective, but reported more positive parenting relative to controls; and similar adult attachment and relationship status. The results were unexpected, but offer novel insights for future prospective studies, which are necessary to better understand psychosocial late effects of childhood cancer.
Introduction
Y
Childhood cancer is a source of intense stress for the whole family, 28 and although parents may genuinely try to support their ill child throughout diagnosis and treatment, they must juggle several responsibilities. On top of worries and practical challenges, normal family routines are disrupted, interfering with children's school, parents' work, or healthy siblings' well-being.29–31 Additionally, parents view their children with cancer as vulnerable, 32 which can prompt them to be overprotective, use less discipline, or spoil them. 33 Apart from potentially becoming overprotective, parents may not be emotionally available. They may be less attentive toward their children's emotions or avoid certain negative emotions (e.g., fear of dying 34 ) as a result of their own worries and responsibilities. Parents of children with cancer are indeed at risk for high distress/anxiety, 35 and anxious parents, in general, tend to be less warm and more controlling than their less anxious counterparts.36,37 Such altered parenting (i.e., less warm/emotionally available, overprotective) may disrupt the bond between parents and children and lead to more insecurely attached children (i.e., more anxious and avoidant 38 ). Thus, although attachment is formed early in life,39,40 and is assumed to remain relatively stable from childhood to adulthood,41–43 it could be disrupted by childhood cancer. This has not been studied explicitly, but could be expected based on studies that link negative life events (e.g., abuse, poverty, parental death, divorce) to insecure attachment.22,23,25,44 Children that had experienced negative life events were found two times more likely to switch from secure to insecure attachment from infancy to early adulthood 22 ; and the overall stability of attachment across the life span was questioned lately as ∼40% of infants who were securely attached, had insecure attachment at age 18. 45 Whether childhood cancer qualifies as such a negative life event and whether it is related to adult attachment has not been studied previously.
Secure attachment in adulthood is characterized by the ability to let others (i.e., romantic partners) get close without worrying about being abandoned or getting too close. 27 Insecure attachment, on the other hand, encompasses avoidant and anxious attachment styles wherein people have difficulties trusting or depending on others (avoidant), or where people have excessive worries about not being liked and desire to keep people too close (anxious). 27 Thus, attachment styles are vital for the quality of romantic relationships,26,27 but less is known about whether attachment styles facilitate or hinder engaging in romantic relationships (vs. staying single). One seminal article 46 suggested three processes of how attachment styles and marital status might be related: First, avoidantly attached adults may be more likely to be single, as they favor independence and self-reliance. Second, anxiously attached adults may be more likely to be single due to extensive worries along with past rejections and failed relationships. Third, single individuals may not be different in their attachment styles from partnered individuals as they rely on other attachment figures (e.g., friends, parents, siblings). 46 The limited empirical evidence has shown support for all three proposed processes (e.g., process 1,47,48 2, 49 and 350,51) and more research is needed. Studies on attachment styles among adult childhood cancer survivors are missing, but qualitative studies indicate support for process 1 and 2. Specifically, survivors were found to either have a desire to be very close to a partner or keep people at distance. 13 Survivors also reported internal barriers to forming romantic relationships, such as concerns that dating partners feel sorry for them,14,52 hesitations to disclose their cancer history/side effects, and fear of rejection.15,53–55
Although empirical evidence is scarce, there are indications that childhood cancer, as a potential negative life event, can alter parenting and, therefore, disrupt attachment even after it has been established in early childhood. Consequently, this could have a profound impact on survivors' adult attachment and romantic relationships throughout life. Specifically, we hypothesized that [H1] survivors would remember their parents as more overprotective and as less warm/emotionally available, and that [H2] survivors would be more insecurely attached in adulthood than healthy peers (i.e., more avoidant and anxious). We further expected attachment to differ between single and partnered individuals, hypothesizing that [H3] singles (both survivors and controls) would report higher attachment-related avoidance and/or anxiety. Finally, we hypothesized that [H4] childhood cancer would be associated with a greater likelihood of being single, through parenting and insecure adult attachment (hypothesized model in Fig. 1).
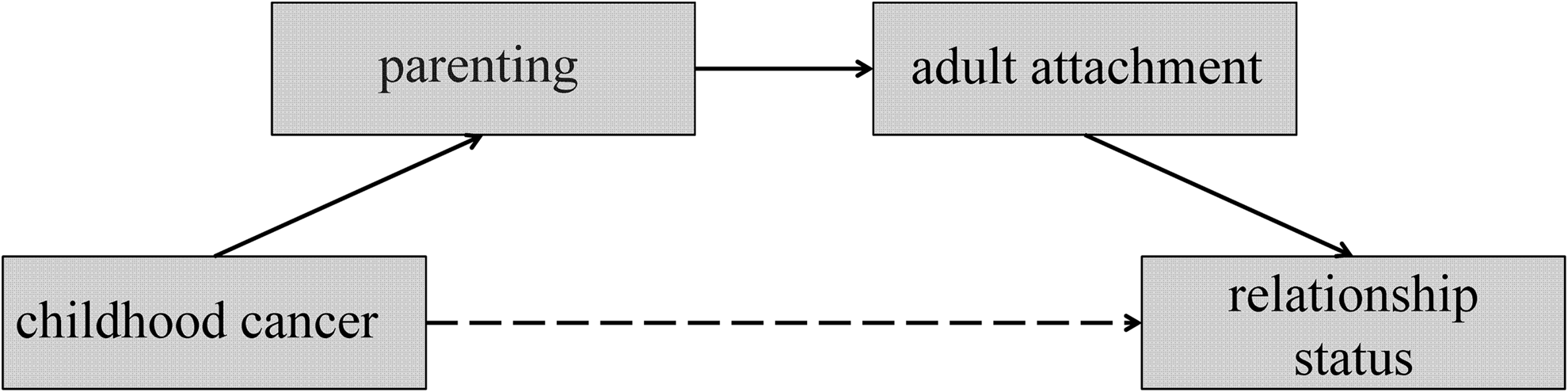
Hypothesized model of childhood cancer indirectly influencing survivors' relationship status in adulthood, through parental behaviors and survivors' adult attachment.
Methods
Data collection and eligibility
Adult survivors of childhood cancer treated at Nationwide Children's Hospital in Columbus, Ohio were eligible if (1) they were young adults (aged 20–40) at recruitment, (2) aged 5–18 at diagnosis of any malignancy (and thus likely to remember treatment), and (3) at least 5 years post diagnosis. Eligible survivors were identified via the hospital's registry and sent an invitation letter, which provided a web link and unique identification number for survivors to complete the survey online. If survivors did not participate within 2 weeks, they were reminded by phone. Participants were compensated $20. This study was approved by the Institutional Review Boards of Nationwide Children's Hospital Columbus, Ohio and the University of Groningen, the Netherlands.
Participants
Childhood cancer survivors
A total of 539 survivors were sent an invitation letter, but 119 participants had confirmed incorrect contact information. Thus, 420 survivors potentially received our letter. We had incorrect phone numbers for another 186 survivors (as identified in the reminder procedure), which could indicate that letters were also sent to outdated addresses. Hence, the number of eligible participants who potentially received our invitation ranged from 234 to 420, of which 173 survivors started the survey (RR = 41%–74%), and 166 completed it. Seventeen participants were subsequently excluded due to skipped/contradictory answers (n = 7) or not meeting inclusion criteria (n = 10). Thus, complete data were available from 149 adult childhood cancer survivors.
The final sample consisted of 55% female (n = 82) and 91% Caucasian (n = 135) survivors. They were young adults with a mean age of 27.8 years (SD = 5.3, range 20–40) and were diagnosed 16.2 years before this study (SD = 6.4, range 5–34 years) at an age of 11.7 (SD = 3.8, range 5–18 years). Survivors had been treated for brain tumors (n = 52, 35%), leukemia (n = 42, 28%), lymphoma (n = 31, 21%), or other solid tumors (n = 24, 16%).
Healthy controls
U.S. residents were invited to participate in this study by Survey Sampling International (SSI), a company specializing in survey data collection. Four hundred people aged 20–40 years without a previous or current cancer diagnosis participated. From this pool, we matched one control to each survivor based on gender, age, and race. After matching, groups were also found similar on other sociodemographic factors (i.e., relationship status, education, occupation).
Measures
Memories of upbringing
EMBU is the Swedish acronym for “my memories of upbringing,” a scale measuring adults' perceptions of their mothers' and fathers' parenting behaviors. The 23-item short version EMBU 56 assesses three subscales for mothers and fathers separately: emotional warmth, overprotection, and rejection. If participants were raised by a single mother/father, they were presented with the respective version of the EMBU. Each item was answered on a 4-point scale (no, never to yes, most of the time). For each subscale, items were averaged with higher scores indicating more emotional warmth, overprotection, or rejection. Psychometric properties of this measure have been tested extensively across several countries and various languages, finding strong validity and reliability. 56 Cronbach's alpha ranged from 0.79 to 0.91 for all subscales among survivors and controls.
Adult attachment
The short version of the Experience in Close Relationships Scale (ECR 57 ) is a widely used, validated, and reliable measure to assess insecure adult attachment. It produces two separate sub-scales: attachment-related anxiety and attachment-related avoidance (six items each). Items referred to current/potential romantic partners to accommodate both partnered and single individuals. Participants rated their level of agreement with each item on a 7-point Likert scale ranging from strongly disagree to strongly agree. Items were recoded and summed to yield the two subscales, with higher scores indicating greater attachment-related avoidance/anxiety. Cronbach's α equaled 0.82/0.81 (avoidance) and 0.80/0.76 (anxiety) for survivors and controls, respectively.
Statistical analyses
Multivariate Analyses of Variance (MANOVA) were used to compare differences in parenting and adult attachment using group status (survivors vs. control), relationship status (single vs. partnered), and their interaction as fixed factors [H1–3]. In addition, Cohen's d effect sizes were calculated to estimate the magnitude of mean differences. Power analyses using G*Power 58 assured that with two groups of 149 we had ample power (>0.9) to detect moderate differences (d = 0.4) between groups. Bivariate correlations among all variables were calculated to check for multicollinearity and are presented for the sake of completeness. Finally, double mediation models were tested using PROCESS, an SPSS macro. 59 We tested whether childhood cancer (vs. healthy control) was indirectly associated with relationship status (partnered vs. single) via parenting and attachment-related avoidance or anxiety (H4, Fig. 1). This procedure produces tests of direct and indirect effects for each model based on 10,000 bootstrap subsamples. We z-transformed all variables for mediation analyses to provide standardized beta-weights.
Results
Group comparisons [H1–3]
Under H1, we expected survivors to remember their parents as overprotective and as less warm, which was not supported by our data: Overprotection was similar between groups, while survivors experienced their mothers and fathers as emotionally warmer (d = 0.55/0.30) and mothers as less rejecting (d = 0.32; Table 1) than healthy peers. Contradicting H2, adult attachment was similar between survivors and controls (Table 1). In addition, memories of parenting and adult attachment did not vary based on gender, age, or age at diagnosis. As expected under H3, adult attachment differed between single and partnered participants, such that singles (n = 110) reported both higher attachment-related avoidance and anxiety than partnered participants (n = 188; d = 0.91/0.24; Table 2). We had also expected that this would be true for survivors and controls, which was the case for attachment-related avoidance (i.e., no significant interaction was found), but not attachment-related anxiety: We found a significant interaction indicating that partnered survivors reported the lowest levels of attachment-related anxiety, while the other three groups were comparable (d = 0.38–0.47; Table 2).
Fifty-six participants grew up in single-parent household; therefore reports for fathers and mothers ranged from n = 116–142 in both groups; 12 participants grew up with a legal guardian and were not included in analyses involving parenting; Note that we explored differences by gender and associations with age (at study participation) finding no gender differences (all ds < 0.13) or associations with age (all rs < 0.13). Further, survivors' age at diagnosis was unrelated to the investigated concepts, as survivors diagnosed before age 13 (n = 81) versus 13+ (n = 68) did not differ (ds<0.19).
p < 0.01.
equal numbers of partnered survivors and controls were married versus in a committed relationship: n = 48 versus 44 survivors and n = 53 versus 43 controls.
p < 0.01.
p < 0.05.
Relationship status and cancer [H4]
Mediation analyses tested our final hypothesis [H4] where we expected that childhood cancer would be associated with a greater likelihood of being single, through parenting and insecure adult attachment. These mediation analyses were performed separately for the three mother and three father parenting variables in combination with either attachment-related avoidance or anxiety (i.e., 12 models). Analyses showed several significant, but scattered pathway associations within these models (note that bivariate correlations between parenting and attachment were rather weak with rs ≤ 0.32; Table 3). The expected indirect effect from cancer, via parenting and attachment, to relationship status was only found in three models (Fig. 2). Specifically, having had cancer was associated with higher emotional warmth in fathers (model A) and mothers (model B), which was associated with lower attachment-related avoidance in adulthood and a greater likelihood to be in a romantic relationship. Models A and B explained 22% and 20% of the variation in relationship status. Similarly, cancer was associated with lower mother rejection (model C), which was again associated with being partnered, but through lower attachment-related anxiety and not avoidance (explaining only 2% of the variation; Fig. 2).
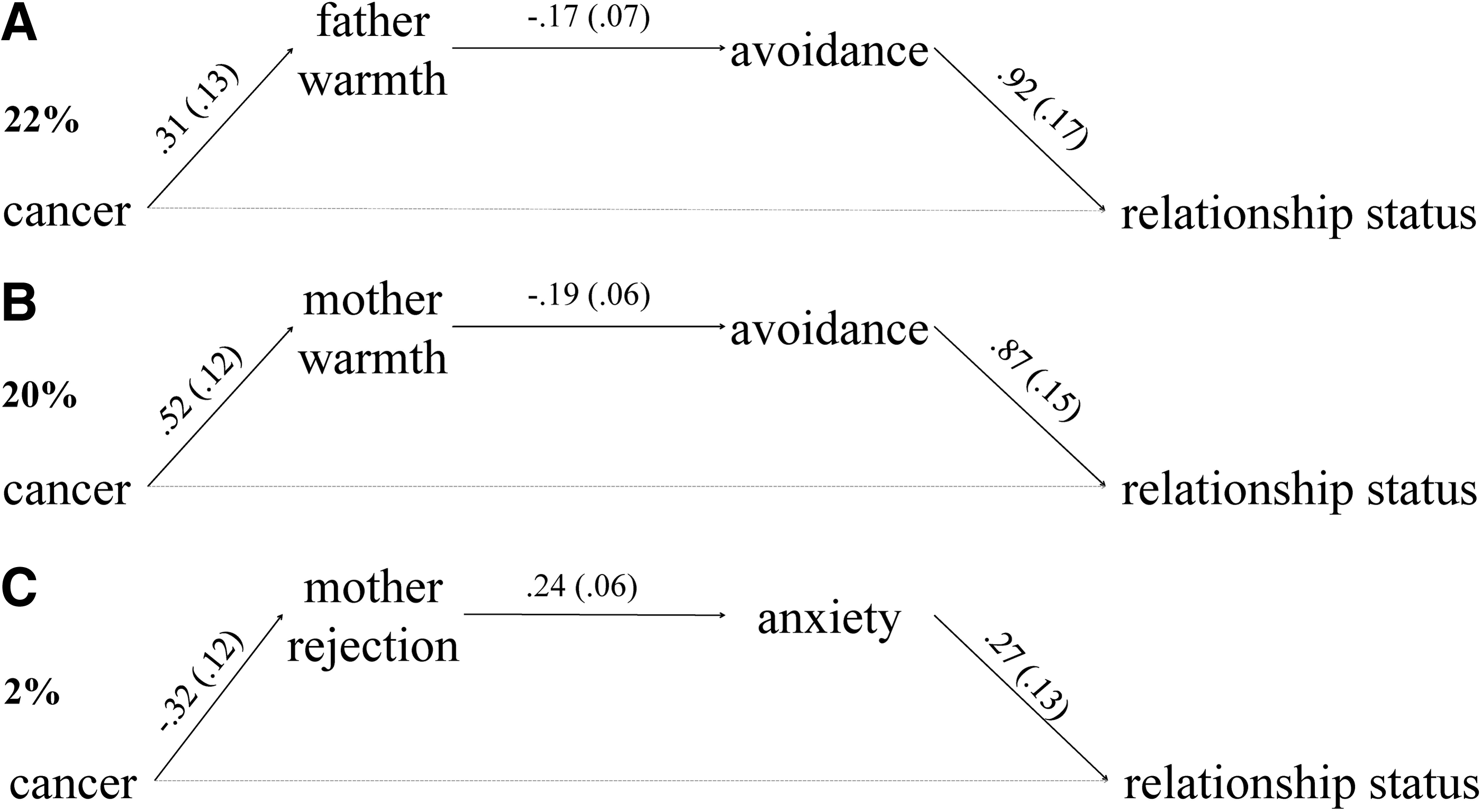
Results of the three models that showed significant indirect effects.
p < 0.01.
p < 0.05.
Discussion
This study examined childhood cancer survivors' memories of their parents' behaviors, adult attachment, and relationships status. Survivors' adult attachment was overall similar to controls, but partnered survivors reported particularly low attachment-related anxiety. Moreover, survivors remembered their mothers' and fathers' parenting more positively than did controls (i.e., warmer and less rejecting), which contradicted our hypothesis that the stress of childhood cancer might strain the parent-child relationship. The differences in perceived parenting behaviors were modestly related to attachment and relationship status in adulthood. Specifically, childhood cancer was indirectly associated with a greater likelihood of being partnered in adulthood via higher perceived parental warmth and lower levels of attachment-related avoidance. However, portions of these associations remain unexplained, and several aspects should be considered.
Survivors recalled their parents as considerably warmer and less rejecting than controls (d = 0.32–0.55), which could be a direct consequence of parents' efforts to comfort their children during and after cancer treatment. Although parents are distressed when caring for a child with cancer, 35 they also experience increased closeness with their children.60–62 Supporting this notion, we found survivors remembered their parents' behaviors as more positive than controls, and contrary to our expectations, survivors did not recall their parents as having been more overprotective. However, survivors not identifying their parents as overprotective in hindsight, might be seen as a type of “interpersonal pattern”: although parents of children with cancer genuinely exhibit overprotective and controlling behaviors, 33 children may not recognize these parenting practices as such, due to their close/warm parent-child relationship. Thus, children may adapt to their parents' close involvement throughout treatment and survivorship,63,64 and they may come to interpret these parenting behaviors as normal, warm, or appropriate rather than overprotective. This might also be supported by qualitative studies where survivors report feeling very close to their families. 65
Furthermore, positive parenting could have served as a source of resilience for survivors, as they did not differ on adult attachment. This was surprising, considering studies among children with other diseases (e.g., cystic fibrosis, asthma) that found these children were more insecurely attached. 38 This suggests that childhood cancer could have different implications for families than other childhood-onset diseases, potentially because life can be resumed after childhood cancer treatment, while other diseases are chronic and require continuous monitoring/treatment. Additionally, it is possible that the life-threatening nature of cancer inspires different parental behaviors and brings families closer together, 66 which could affect attachment styles differently. While we do not have data on the attachment styles of children before diagnosis, during or shortly after treatment, we want to highlight that our sample had established attachment styles with their parents by the time of diagnosis (all were older than 5). Hence, cancer as a potentially disruptive life stressor, after attachment had been established, did not put survivors at greater risk for attachment insecurity in adulthood.
Confirming two processes suggested in the previous literature, 46 singles reported higher levels of insecure attachment (i.e., higher attachment-related anxiety and avoidance), and effects were much stronger for avoidance than anxiety (d = 0.91 vs. 24). Although survivors and controls did not differ on adult attachment, it appeared that partnered survivors reported particularly low attachment-related anxiety. This may be interpreted in light of qualitative studies that reported survivors feel more mature than their peers. 65 Along these lines, we speculate that survivors who engage in romantic relationships are thoughtful and conscientious in interpersonal interactions, and therefore, do not exhibit dysfunctional interpersonal behavior patterns, which are characteristic of insecurely attached individuals (e.g., needing a lot of reassurance, not turning to a partner in times of need).
The indirect effect of cancer on relationship status through parenting and adult attachment was only supported by 3 out of 12 models: Childhood cancer was related to greater emotional warmth in both parents and lower rejection in mothers (as experienced by survivors). Greater emotional warmth was then associated with less attachment-related avoidance, while lower mother rejection was related to less attachment-related anxiety. These pathways were ultimately associated with a greater likelihood of being in a relationship. Hence, childhood cancer may improve parent-child interactions,60–62 and foster more positive and meaningful interactions with others later in life. Generally, this corroborates research in healthy children wherein positive parent-child interactions predicted warm and supportive relations with romantic partners and greater relationship quality in adulthood. 67 Overprotective parenting did not mediate the relationship between childhood cancer and relationship status. However, as noted previously, long-term survivors may be less likely to identify overprotective parenting as such. Hence, the influence of actual parenting behaviors on adult survivors' outcomes should be tested prospectively.
Overall, the findings of this study should be regarded in light of its limitations. Our sample may be biased toward survivors who were comfortable and interested in answering questions about romantic relationships. However, our response rates were similar to other studies on related topics among adult survivors of childhood cancer (e.g.,4–6 ). In addition and as mentioned above, we tried to relate childhood experiences to adult outcomes based on cross-sectional single-informant data, and recall bias about parenting may be present. Although this is a limitation for the focus of this study, adults' memories of their childhood can have inherent value. However, longitudinal studies incorporating repeated and/or observational measures of parenting behaviors during cancer treatment and outcomes in long-term follow-up are needed to better understand our proposed associations.
Generally, our findings indicate that long-term childhood cancer survivors' romantic involvement is similar to healthy peers. Cancer appears to have influenced parenting in a positive way, as parents showed enhanced emotional warmth and less rejection. This had modest effects on attachment and romantic relationships in adulthood, but results might be subject to recall bias. Overall, this first case–control study offers new insights into novel topics in long-term childhood cancer survivors. Clinical implications include the importance of assessing or screening family functioning and social outcomes over time. If problems are indicated, interventions should occur as early as possible. However, it appears that many families already exhibit positive parenting/warm interactions, which healthcare providers should continue to facilitate, as it may promote long-term romantic functioning. Yet, our understanding remains limited, and more, preferably longitudinal, research should address additional underlying factors of survivors' romantic and general well-being.
Footnotes
Acknowledgments
This project was funded by the Dutch Cancer Society, RUG 2009-4442 (M.A.T.) and the Research Institute at Nationwide Children's Hospital, USA (V.L.).
Disclaimer
Parts of this article have been presented at the World Congress of the International Psycho-Oncology Society (IPOS) and the American Psychosocial Oncology Society (APOS) in Washington, D.C. in 2015. Other data (including body image and sexual satisfaction) using a smaller portion of this sample (n = 87) have been published previously. 21
Author Disclosure Statement
No competing financial interests exist.