
Abstract
Purpose:
Survivors of cancer may experience higher rates of psychological problems requiring pharmacological interventions than age-matched controls from the general population. This study compares prescription rates of antidepressants in survivors of cancer, diagnosed in childhood, adolescence, or early adulthood, to the rate in age- and gender-matched controls from the Norwegian population.
Methods:
Antidepressants prescribed to 5341 cancer survivors, diagnosed ≤25 years during 1965–2000, were studied in a population-based cohort by linking data from the following nationwide registries: the Population Registry of Norway, the Cancer Registry of Norway, and the Norwegian Prescription Database. For each survivor, three age- and gender-matched controls were randomly selected from the population. A Cox proportional hazard model was applied to estimate hazard ratios (HRs) of antidepressant prescriptions during 2004–2012 to the survivors with controls as referents.
Results:
Survivors had an increased risk of being prescribed antidepressants with crude rates of 26.9/1000 person-years compared with 22.5/1000 person-years in controls (HR 1.19; 95% confidence interval [CI] 1.12–1.28). The relative risk was highest for survivors of central nervous system tumors (HR 1.30; 95% CI 1.04–1.63), leukemias (HR 1.29; 95% CI 1.03–1.63), testicular tumors (HR 1.27; 95% CI 1.04–1.55), and “other tumors” (HR 1.42; 95% CI 1.10–1.84). No effect of age at cancer diagnosis was found.
Conclusion:
Certain groups of survivors of cancer in childhood, adolescence, or young adulthood have a slightly increased risk for being prescribed antidepressants than their peers. The results may indicate an increased prevalence of depression among these survivors, but diagnostic reasons for prescriptions need to be confirmed in clinical studies.
Introduction
I
Experiencing cancer at a young age is stressful, challenging, and disruptive to patients and their families. 2 There is a risk of psychological problems resulting from subjective discomfort, frequent hospitalizations, separation from friends and family, and insecurity regarding the future.3,4 As with any severe stressor, the way in which a child or an adolescent is affected by cancer and responds psychologically varies with age, biopsychological vulnerabilities, coping capacity, and social support. Adolescents, who are able to cognitively understand the seriousness of a life-threatening disease, may be the most vulnerable group. 5 There is also a risk of direct unfavorable effect of the disease itself or the treatment on the central nervous system (CNS), especially among the youngest patients. This may increase their vulnerability to subsequent psychological problems.2,6 Children and adolescents undergoing cancer treatment may therefore be at risk for developing depression, anxiety, and other psychological difficulties later in life. However, the empirical evidence to support this assumption has been equivocal.5,7–13
Examining the prevalence of depression in childhood, adolescent, and young adulthood cancer survivors (CAYAS) can be challenging. Patient-reported outcomes vary by content and validity, and their use is associated with a risk of selection bias. Clinical interviews are limited by the practicalities associated with achieving a sufficient sample size. 14 Population-based studies of health registry data have the advantage of including well-defined populations, thus eliminating self-selection or recall bias. 15
Antidepressants are a group of medications that are commonly prescribed for mental health conditions, primarily for depression, but also in some cases for anxiety disorders.16,17 Knowledge of prescriptions of antidepressants may yield information about the extent to which doctors perceive CAYAS to have a psychiatric problem requiring therapy with psychotropic drugs, and can thus be used as a proxy to measure the prevalence of such disorders in this group.
Only a few register-based studies have been published on the use of antidepressants among CAYAS.18,19 In a Danish study, Lund et al. showed an increased risk of having antidepressants prescribed among CAYAS diagnosed before the age of 20 years. 18 A recent study on antidepressant use among children and adolescents in the general population in Denmark shows a prevalence that is the double of what is found in Norway. 20 Deyell et al. also found a higher prescription rate among Canadian CAYAS than in the general population, based on data from a regional registry. 19
The main objective of the present study was to study the prescription rate of antidepressants among Norwegian survivors diagnosed with cancer at the age of 0–25 years compared to population controls. We also wanted to study if the prescription rate differed between CAYAS treated for different cancer types. Based upon previous studies of psychiatric morbidity among CAYAS, 21 we hypothesized that CAYAS would have a higher prescription rate of antidepressants compared to matched controls and that survivors of tumors in the CNS and bone tumors were at highest risk.
Secondary objectives were (1) to explore if the gender and age distributions of CAYAS being prescribed antidepressants were as in the general population, (2) to explore if age at time of diagnosis affected upon prescription rate among the survivors, and (3) to compare the prescribing physician's medical specialization in CAYAS versus controls.
Methods
The present study is based on data from the three following national registries: the Population Registry of Norway, the Cancer Registry of Norway, and the Norwegian Prescription Database (NorPD). Data were linked by the unique personal identification number, assigned to every Norwegian citizen.
Data sources
Population Registry of Norway
The Population Registry contains demographic information on all residents in Norway since 1960, including date of birth, place of residence, and date of migration or death.
Cancer Registry of Norway
The cancer registry has received nationwide data since 1953 on all patients diagnosed with cancer in Norway. The mandatory reporting is based on the four following sources of information: (1) copies of pathology and autopsy reports from all laboratories in the country, (2) registration forms filled in by clinicians reporting the localization of the cancer, extent of disease, and initial treatment, (3) copies of all death certificates that state neoplastic disease, and (4) all hospital discharge diagnoses. Relapses are not routinely registered. 22
Norwegian Prescription Database
From January 1, 2004, the Norwegian Institute of Public Health receives monthly electronic data on all filled prescriptions that have been dispensed from pharmacies to patients in ambulatory care. Both reimbursed and nonreimbursed drugs are included in NorPD. 23 Drugs are classified according to the Anatomical Therapeutic Chemical (ATC) classification system. 24
Study population
Cancer survivor cohort
The study aimed at including all patients in Norway diagnosed with cancer ≤25 years of age during 1965–2000. Survivors who were alive, still residing in Norway, and 18 years or older at start of follow-up for antidepressant prescriptions (January 1, 2004) were included. Secondary malignancy was not an exclusion criterion. A total of 5341 survivors were included in the analyses (Fig. 1).
Timeline of inclusion. CAYAS, childhood, adolescent, and young adulthood cancer survivors.
Cancer types were grouped into diagnostic groups according to the International Classification of Childhood Cancer (ICCC-3) 17 with a few exceptions. Due to different distributions of incidence rates, germ cell tumors were reported for each gender separately. Thyroid gland cancer and gastrointestinal cancers are classified as “other neoplasms” in ICCC-3, but as the incidences of these cancer types increase in young adults, they are reported separately in the analyses. In our material, a few survivors had been treated for liver cancer, and due to low numbers, these were included in the group “other tumors.”
Comparison controls
For each survivor, three age- and gender-matched controls without cancer at the time of the survivor's cancer diagnosis were randomly drawn from the Population Registry of Norway. All controls were alive, still residing in Norway, and 18 years or older when entering the study, but some had deceased or emigrated at the start of follow-up (January 1, 2004).
Thirteen controls were found to have had cancer younger than the age of 25 years and were therefore removed from the control cohort. Cancer after the age of 25 was not an exclusion criterion. A total of 14,855 controls were included in the analyses (Fig. 1).
Prescriptions of antidepressants and prescribing physician
Antidepressants are available only on prescription in Norway and are usually dispensed in an amount sufficient for about 3-month use. Information on all prescriptions for antidepressants in the ATC group N06A in the period of January 1, 2004–December 31, 2012, was obtained from NorPD. Antidepressants include selective serotonin reuptake inhibitors (SSRIs), serotonin–norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and atypical agents. TCAs are also frequently used as coanalgesics but in a lower dosage than for depression.
NorPD also includes data on the prescribing physician's medical specialization. The specialty was categorized into three groups as the following: (1) General practice, (2) Other specialty, and (3) No specialty.
Analysis strategy and statistical methods
Survivors and controls were followed from January 2004 until the first of the following events: initiation of antidepressant prescription (endpoint), emigration, death, or end of study period (December 31, 2012) (Fig. 1). The crude rates for antidepressant prescription per 1000 person-years were calculated for survivors and controls. Crude rates were calculated separately for men and women and for survivors of different cancer types. In the next step, a Cox proportional hazard model was applied to estimate the hazard ratios (HRs) with 95% confidence interval (CI) of use of antidepressants in CAYAS with controls as referents. Analyses were adjusted for age at start of follow-up (2004) and gender. We performed separate Cox analyses for each cancer type with controls as referents.
For the secondary analyses, the effect of age at cancer diagnoses was evaluated by using a Cox proportional hazard model with age as a continuous variable.
Physicians' medical specialty was investigated for the first prescription of antidepressant for survivors and controls. Chi-square statistics were used to test for significant differences in medical specialty when prescribing antidepressants.
Sensitivity analyses were performed by repeating analyses with two other definitions of antidepressant prescriptions: (1) only SSRI and SNRI were considered as antidepressants (i.e., TCA excluded) and (2) antidepressant prescription was defined after two prescriptions had been filled out on different dates.
Results
Participant characteristics
Out of 5341 participating survivors, 2764 (51.8%) were males (Table 1). Fifty-six percent of the survivors were between 18 and 25 years at time of diagnosis. The most frequent cancer types were skin cancer (mostly melanoma), lymphomas, and testicular cancer. At the start of follow-up in 2004, 20 years or more had passed since the time of cancer diagnoses for 43% of the survivors.
Crude rate for antidepressant use per 1000 person-years.
Users of SSRI or SNRI (users of only TCA excluded).
Defined as user if redeemed at least two independent prescriptions for antidepressants.
AD, antidepressants; CNS, central nervous system; SNRI, serotonin–norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Overall, 1088 survivors and 2596 controls had been prescribed antidepressants during the study period.
Rates for antidepressant prescriptions
Crude rate for antidepressant prescriptions was higher among survivors (26.9/1000 person-years) than among controls (22.5/1000 person-years) (Table 1). Differences were observed in both genders. Females were more often prescribed antidepressants than males in both survivors and controls. Survivors who had been treated for female genital cancer had the highest crude rates of being prescribed antidepressants, followed by thyroid cancer and soft tissue cancer (Table 1).
The Cox model showed an increased risk of antidepressant prescription among survivors overall (HR 1.19; 95% CI 1.12–1.28) (Fig. 2), and in diagnostic groups, leukemias (HR 1.29; 95% CI 1.03–1.63), CNS-tumors (HR 1.30; 95% CI 1.04–1.63), testicular cancers (HR 1.27; 95% CI 1.04–1.55), and tumors classified as others (HR 1.42; 95% CI 1.10–1.84).
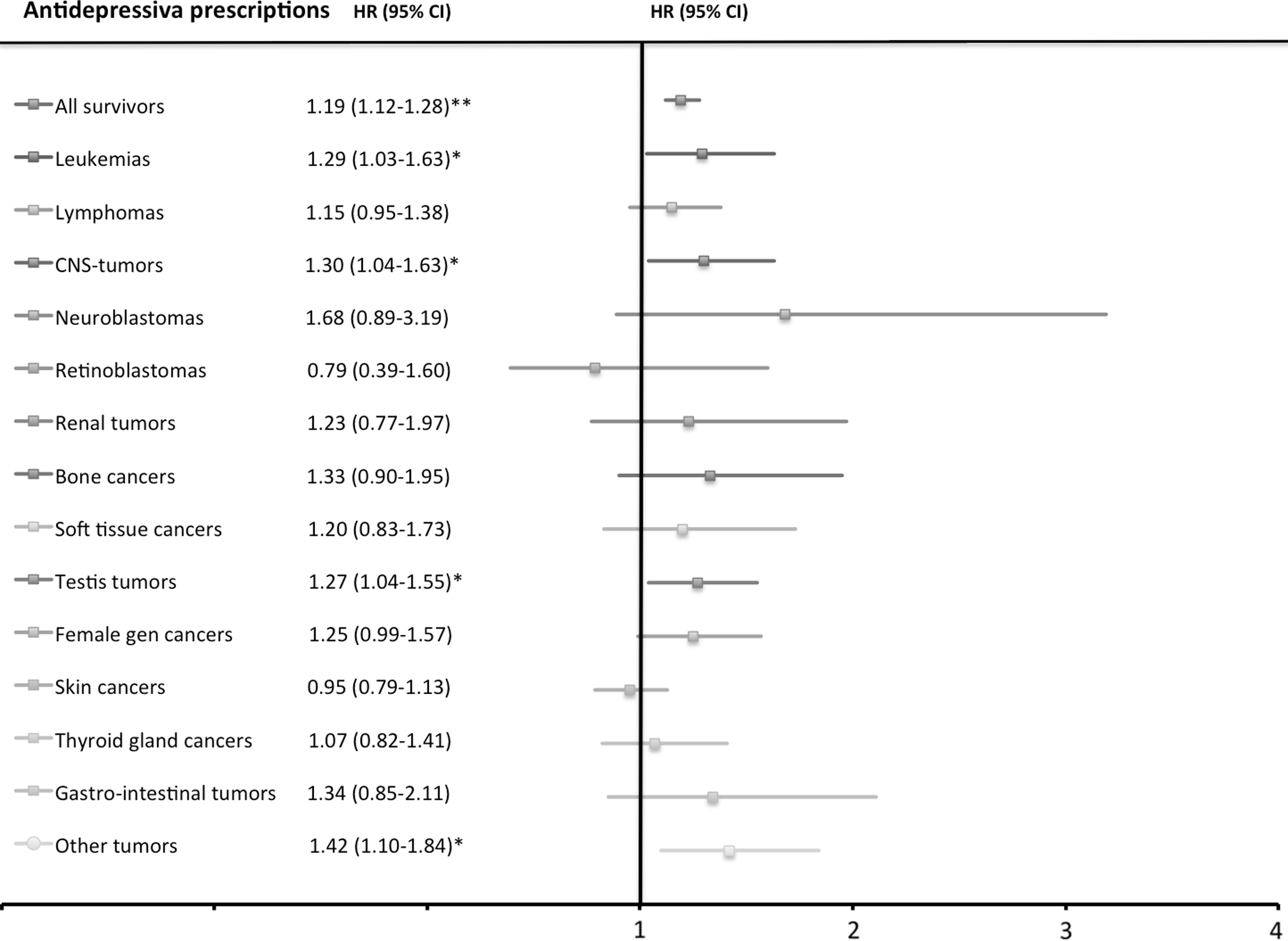
Forest plot of univariate hazard ratios of antidepressive prescriptions among CAYAS.
In the secondary analysis, we found no increased risk of antidepressant prescription by age at cancer diagnosis or after adjustment for gender and age attained at start of follow-up in 2004 (HR 1.05; 95% CI 0.97–1.14). Age at first prescription was similar in both groups. The physicians' specialties were associated with nonsignificant differences in prescription rates for the first prescription of antidepressants, as general practitioners had prescribed the first antidepressants to 60.5% of the controls and to 62.7% of the survivors. About 20% of the prescribing physicians did not have a registered specialty.
Analyses of prescriptions of SSRI or SNRI
In the sensitivity analysis of including only prescriptions of SSRI or SNRI (TCA excluded) the crude rate for antidepressant prescription for survivors was higher (22.4/1000 person-years) compared to controls (18.3/1000 person-years). In secondary analyses requiring at least two prescriptions of antidepressants, the crude rate for antidepressant prescription for survivors was higher (18.4/1000 person-years) compared to controls (15.0/1000 person-years) (Table 1).
Discussion
The results of the present study support the hypothesis of increased prescription of antidepressant medication to survivors of cancer in childhood, adolescence, and early adulthood, compared to a population-based control cohort.
In our study, the risk for CAYAS being described antidepressants was 20% higher than in the compared controls. The difference was smaller than anticipated but is comparable with the Canadian study. 19 This may reflect what is shown in several studies that many CAYAS have the capacity to adjust psychosocially.11,25–28 However, the difference was somewhat higher in the Danish study, in which there was a 38% increased risk. 18 Healthcare policies are similar in Norway and Denmark, but the inclination to prescribe antidepressants may still differ between the physicians. As previously mentioned, antidepressant use among children and adolescents in the general population in Denmark has been shown to be significantly higher than what is found in Norway. 20 Female survivors had a higher risk of being prescribed antidepressants than males in both survivors and controls, similar to what is found in the general population. 29
Several studies have shown that cancer in adolescence has a greater impact on later psychological health than if the disease strikes in preschool age.5,12,21,30 Adolescence is a period of rapid neurocognitive development and important milestones such as establishing one's identity and peer-relationships, setting future goals, as well as growing independence. However, age at diagnosis did not seem to have an effect on our results. This is concordant with the results in the Danish study. 18
Survivors of CNS-tumors, leukemias, testicular cancers, and “other tumors” carried a significantly increased risk of antidepressant prescription. The remaining cancer types except for retinoblastoma and skin cancer had point estimates (HR) above unity but not significant. The high risk among CNS survivors is in line with a recently published review article on survivors of pediatric brain tumor, where 8 out of 11 studies reported increased risk of depression among the survivors. 31 A large proportion of the CAYAS in our study that was treated for CNS tumor and for leukemia had, according to the treatment regimens used during 1965–2000, received radiotherapy and/or intrathecal chemotherapy as a part of their treatment. Both modalities have been associated with changes in brain development and neurocognitive impairment, leading to difficulties with social skills and decreased cognitive efficiency.32,33 More recent treatment protocols have improved with increased focus on possible late adverse effects of the anticancer therapy. In 1992, cranial radiotherapy was removed from the Nordic protocol for lower risk acute lymphatic leukemia, and from 2008, no cranial radiotherapy is included in the first-line treatment for leukemia. 34 Cranial irradiation is still used in treatment of CNS tumors, but the current protocols focus on lower radiation doses and smaller radiation fields. Testicular cancer survivors were also at increased risk of being prescribed antidepressants. That is not in concordance with results from a Norwegian study by Fossa et al. 35 In that questionnaire-based study, testicular cancer survivors reported lower scores of depression but higher scores of anxiety than the general population. However, antidepressants are often prescribed for anxiety problems.
The survivors received their prescription from the specialized health service to a similar degree as the controls. As more than 20% of the prescribing doctors did not have a registered specialty, it is difficult to interpret the data and to assume a larger degree of specialized follow-up among CAYAS due to late effects that have already emerged or the CAYAS concerns of possible late effects.
The use of population-based registries is a major strength of this study. As all Norwegian citizens have their unique ID number, they can be tracked in the registries by their encrypted ID number, which enables a comprehensive follow-up. By linking large administrative databases, it is possible to create a large cohort that can give more power to late effect studies among CAYAS.
We did not exclude CAYAS that had been treated for a relapse or a second malignancy, but separate analyses for these groups were complicated, as the date of the occurrence was not registered. Controls found to have had cancer before the age of 25 (i.e., had in fact cancer in childhood, adolescence, or young adulthood) were excluded, but they may have had cancer after the age of 25 years.
The major limitation of this study is that the NorPD was first established in 2004, and we do not have information on antidepressant descriptions before that time. Also, the indication for the antidepressant prescription was not available. Anxiety and neuropathic pain are other conditions that can be treated with antidepressants. 13 However, sensitivity analyses excluding TCA still showed similar differences. Other late effects such as chronic fatigue, pain, and reduced activities of daily living that may increase the risk of depression were not controlled for. Mild to moderate depression can be treated in other ways, such as psychotherapy and physical exercise.36,37 A possible selection bias cannot be excluded as disease- or treatment-related mortality may have resulted in a healthier cohort of cancer survivors with relatively few psychosocial problems. 38
Conclusion
The difference in antidepressant prescription rate was present but smaller than anticipated. Certain types of cancers seem to be associated with psychological problems that the physicians evaluate as indications for antidepressants. Their nature needs to be confirmed in clinical studies. Since depression is by far the most frequent indication for use of antidepressants, the findings might indicate an increased prevalence of this disorder. Understanding the predictors of antidepressant prescription to survivors of cancer in a young age is relevant knowledge for the follow-up care of CAYAS.
Footnotes
Acknowledgment
The South-Eastern Norway Regional Health Authority funded this study.
Author Disclosure Statement
No competing financial interests exist.