
Abstract
Purpose:
To identify the utility and issues associated with the use of decision trees in oncofertility patient care in Japan.
Methods:
A total of 35 women who had been diagnosed with cancer, but had not begun anticancer treatment, were enrolled. We applied the oncofertility decision tree for women published by Gardino et al. to counsel a consecutive series of women on fertility preservation (FP) options following cancer diagnosis. Percentage of women who decided to undergo oocyte retrieval for embryo cryopreservation and the expected live-birth rate for these patients were calculated using the following equation: expected live-birth rate = pregnancy rate at each age per embryo transfer × (1 − miscarriage rate) × No. of cryopreserved embryos.
Results:
Oocyte retrieval was performed for 17 patients (48.6%; mean ± standard deviation [SD] age, 36.35 ± 3.82 years). The mean ± SD number of cryopreserved embryos was 5.29 ± 4.63. The expected live-birth rate was 0.66.
Conclusions:
The expected live-birth rate with FP indicated that one in three oncofertility patients would not expect to have a live birth following oocyte retrieval and embryo cryopreservation. While the decision trees were useful as decision-making tools for women contemplating FP, in the context of the current restrictions on oocyte donation and the extremely small number of adoptions in Japan, the remaining options for fertility after cancer are limited. In order for cancer survivors to feel secure in their decisions, the decision tree may need to be adapted simultaneously with improvements to the social environment, such as greater support for adoption.
Introduction
F
Gardino et al. created male and female FP decision trees for United States healthcare providers to help them counsel cancer patients about the FP options. 3 In the female decision tree, in vitro fertilization is presented as an FP option if controlled ovarian hyperstimulation (COS) is not contraindicated and if there is time before the start of chemotherapy. If COS is contraindicated or chemotherapy cannot be delayed, FP options include gonadotropin-releasing hormone analog or antagonist treatment, ovarian transposition, ovarian shielding, ovarian tissue cryopreservation, and immature oocyte retrieval. Options for female patients who do not opt for FP or who are unable to achieve live birth after FP include the use of donor embryo/eggs, gestational carriers, adoption, and attempting a natural pregnancy. The decision trees make it easier for both patients and healthcare providers to understand the treatment process and what FP options are available to them.
The practice of oncofertility in the United States differs from that in other countries, including Japan, in various ways; for example, there are different rules regarding egg and sperm donation and differences in the frequency of adoption in the United States and Japan. Therefore, it is unclear whether the decision trees used in the United States are also useful for FP decision-making in other countries. The utility of the decision trees in Japan has yet to be investigated; this study aimed to identify issues regarding the use of the female FP decision tree for women with cancer in Japan.
Subjects and Methods
Subjects
The study included 35 women who had been diagnosed with cancer, but had not begun anticancer treatment associated with ovarian toxicity (chemotherapy or radiation therapy) and who underwent outpatient oncofertility counseling at our hospital between July 1, 2011 and December 10, 2015. Patient characteristics are shown in Table 1. This study was approved by the Institutional Review Board Committee at the Jikei University School of Medicine.
SD, standard deviation.
Methods
We documented the decision-making processes of patients who were presented with the female FP decision tree before undergoing cancer treatment. Oocyte retrieval that was performed after outpatient oncofertility counseling, but before the first round of chemotherapy or gonadal exposure to radiation, was considered to be FP for the purposes of this analysis.
For patients who chose to undergo oocyte retrieval and embryo cryopreservation, the patient age, number of oocyte retrievals, type of COS, and number of cryopreserved embryos were determined. Based on the 2012 age group-specific Assisted Reproductive Technology Data from the Japan Society of Obstetrics and Gynecology, 4 realistic expected live-birth rates were calculated using patient age and number of cryopreserved embryos with the following equation: expected live-birth rate = pregnancy rate at each age per embryo transfer × (1 − miscarriage rate) × No. of cryopreserved embryos. The mean expected live-birth rate was calculated with rates exceeding 1 treated as 1. These rates were used to estimate the probability of a live birth achieved after FP.
Based on how many patients chose to undergo FP or not and the calculated live-birth rate for those who decided to undergo FP, we evaluated the applicability of the FP decision tree for helping patients make decisions about their future fertility and the issues that may arise among women with cancer in Japan.
Results
Decision-making results
Of the 35 patients enrolled in the study, 23 were married. Among married patients, 17 (48.6% of the total patient number) opted for FP and were candidates for oocyte retrieval and embryo cryopreservation (Table 1 and Fig. 1). None of these 17 patients chose to undergo oocyte or ovarian tissue cryopreservation. Of the 12 unmarried patients, 4 opted for FP and wished to undergo oocyte cryopreservation. These patients were referred elsewhere because this procedure was not available at our hospital at the time.

Patient disposition following fertility preservation (FP) counseling. Of the 35 patients enrolled in the study, 23 were married. Among married patients, 17 opted for FP and were candidates for embryo cryopreservation. None of the 17 patients selected either oocyte or ovarian tissue cryopreservation. Of the 12 unmarried patients, 4 opted for FP and wished to undergo oocyte cryopreservation.
FP results
The mean ± standard deviation (SD) age of the 17 patients who underwent embryo cryopreservation was 36.35 ± 3.82 years, with 76.7% aged 35 years or older (Table 1). Oocyte retrieval was performed 27 times in these patients (mean ± SD, 1.59 ± 0.8 times per patient). The number of cycles with each COS type was as follows: natural cycles, 5; short protocol, 9; antagonist protocol, 4; and aromatase inhibitor plus follicle-stimulating hormone, 9. A total of 90 embryos were cryopreserved, of which 64 were early embryos and 26 were blastocysts. The mean ± SD number of cryopreserved embryos per patient was 5.29 ± 4.63. Using these data, the expected live-birth rate was calculated to be 0.66. A total of six patients (35.5%) had expected live-birth rates ≤0.5 (Fig. 2).
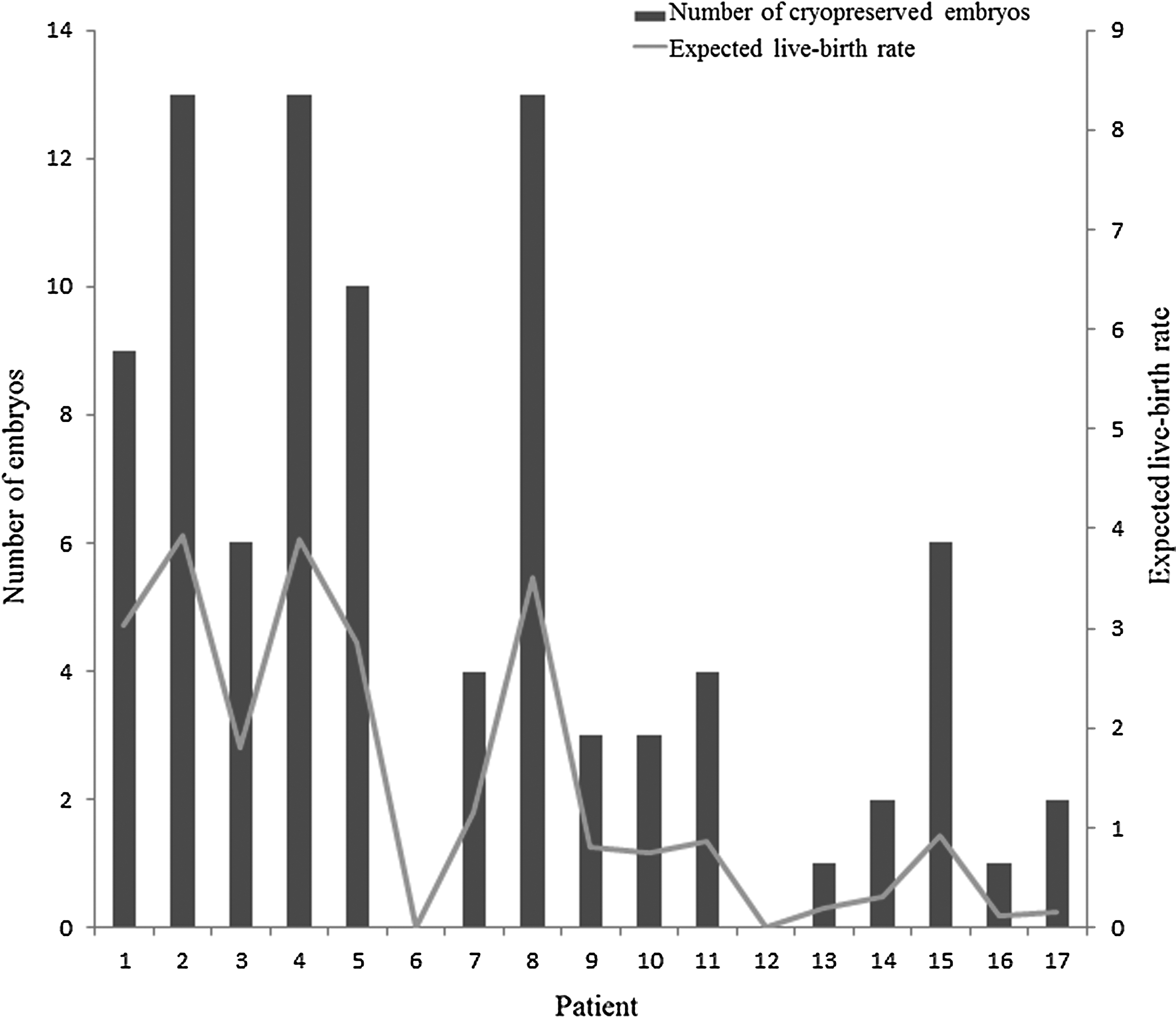
FP results and expected live-birth rates. Expected live-birth rates were calculated for each patient who opted to undergo oocyte retrieval and embryo cryopreservation. Live-birth rates were calculated based on the 2012 age group-specific Assisted Reproductive Technology Data from the Japan Society of Obstetrics and Gynecology using the following equation: expected live-birth rate = pregnancy rate at each age per embryo transfer × (1−miscarriage rate) × No. of cryopreserved embryos. Of the 17 patients who cryopreserved embryos, 6 (35.5%; Patient 6, 12, 13, 14, 16, 17) had an expected live-birth rate of ≤0.5. The six patients were between 35 and 42 years.
Options for patients not opting for FP or unable to achieve live birth with FP
In addition to the 14 patients (40%) who chose not to undergo FP, we estimated that 35% of patients who did choose FP (oocyte retrieval and cryopreservation) would not achieve a live birth. According to the decision tree, these patients would have four options: use of donor embryos/eggs, use of a gestational carrier, adoption, and attempting a natural pregnancy. Because the use of donor embryo/eggs and gestational carriers is not permitted in Japan, the only available options for these women are adoption and attempting natural pregnancy.3,5
Discussion
In 2010, Gardino et al. created male and female FP decision trees for healthcare providers counseling cancer patients in the United States. 3 This study clarified that, although the decision tree is a useful decision-making tool, the expected live-birth rates among those who opted for FP were not high, and 40% of the patients in our study did not choose to undergo FP at all. The patients did not choose FP mainly due to the economic reason or the higher priority for cancer treatment. According to the decision tree, patients not opting for FP or unable to achieve live birth with FP have four options: donor embryo/eggs, gestational carrier, adoption, and attempting natural pregnancy. 3 However, the use of egg donation and gestational carriers is not permitted in various countries, including Japan. 3 Therefore, the only available options for these women in Japan are adoption and attempting natural pregnancy.
Rates of gonadal dysfunction, loss of fertility, and premature ovarian insufficiency (POI) after cancer treatment are high. The incidence varies depending on patient age and anticancer agent type and dose, but it is reportedly between 20% and 100%.6,7 According to the risks by therapeutic strategy reported by the American Society of Clinical Oncology in 2006 and 2013, ≥80% of ovarian insufficiency cases occurred after hematopoietic stem cell transplantation, ovary exposure to radiation, and alkylating agent-based chemotherapy in breast cancer patients aged ≥40 years.6,7 The lifetime natural pregnancy rate in POI patients is 5%–15%.8–10 According to Tartagni et al., estrogen administration may improve fertility in POI patients. 11 However, the patients in that study were younger, with a mean age of 32.9 years. 11 Poorer treatment outcomes can be expected for the patients in our study, who were older (mean age, 36.35 years) at the start of the study and thus would be even older after cancer treatment.
Adoption possibilities for cancer survivors vary by country. For example, adoption is not permitted for patients with diseases affecting life expectancy, including cancer, in China or for persons with “various forms of cancer” in Moldova. 12 Adoption standards are also often unclear in many countries, including Japan and the United States. Gardino et al. investigated adoptions by cancer survivors through 27 domestic and international agencies in the United States. 12 Only 1 of the 27 agencies responded that a history of cancer affected the decision to approve an adoption application. There have been reports of cases where adoptive parents were cancer survivors, although these represent less than 2% of all adoption cases. Two issues have been highlighted with regard to adoptions in Japan: the small number of adoptions that take place and the lack of clarity regarding possibilities for adoption by cancer survivors. The number of annual nonrelative adoptions in Japan is much lower than in the United States: ∼500 in Japan versus ∼60,000 in the United States.13,14 Therefore, the adoption system itself needs to be improved. Further research is required regarding the current state of adoptions by cancer survivors in Japan, which has not been reported to date.
Conclusions
These findings suggest that the restrictions on the use of donor embryo/eggs and gestational carriers, and the extremely low rates of adoption in Japan, limit the utility of the current decision tree for helping patients make decisions about FP and ensuring that their wishes are taken into sufficient consideration. To resolve these issues and for cancer survivors to feel secure in their FP decisions, improvements to the social environment, such as the adoption system, need to be investigated.
Footnotes
Acknowledgments
The authors would like to thank Teresa K. Woodruff, PhD, and Stacey C. Tobin, PhD, for their review of the article.
Author Disclosure Statement
No competing financial interests exist.