
Abstract
Purpose:
Orthotopic liver transplantation (OLT) is curative for hepatocellular carcinoma (HCC). HCC is typically a disease of older adults (OAs); therefore, characteristics and outcomes of OLT for young adults (YAs) (ages 18–40) are not described. The objective of this study was to assess the characteristics and outcomes of YAs with HCC receiving OLT and compare these to OAs (ages >40 years).
Methods:
YAs with HCC who had OLT from the United Network for Organ Sharing (UNOS) database were included in this study. As a comparison group, OAs with HCC were matched 4:1 to the YA group. Descriptive statistics of demographics, comorbidities, and outcomes were generated. Kaplan–Meier product limit estimates were used to assess patient and graft survival. Conditional logistic regression and Cox proportional hazards frailty models were used to compare the groups.
Results:
A total of 464 YAs received OLT for HCC. The most common underlying liver diseases were hepatitis C virus (21.3%), hepatitis B virus (HBV, 15.5%), and autoimmune/cholestatic disease (12.3%). An increased number of YAs received OLT for HCC after implementation of model for end-stage liver disease scoring. One thousand two hundred eighty OAs served as the comparison group. Post-transplant 5-year survival was 73.1% in YAs with a retransplantation rate of 7.8%. In OAs, survival and retransplantation rates were lower (68.6% p = 0.093; 4.3% p = 0.001).
Conclusion:
Four hundred sixty-four YAs with HCC received OLT in the UNOS database. Compared to the older population, survival and retransplantation rates were higher. HBV, which is vaccine preventable, is a frequent contributor to HCC in YAs.
Introduction
H
HCC continues to have a very poor prognosis. Worldwide, the ratio of mortality to incidence is 0.95. 6 Similar to incidence rates, mortality rates also vary by ethnicity, in the same order as incidence. 3 In addition to lower incidence rates of HCC for females compared with males, female sex appears to be protective against mortality, especially in the younger age ranges. 7 Over recent years, there has been greater increase in the rate of diagnosis of earlier stage disease compared to regional and distant disease, postulated to be due to surveillance programs. Despite earlier diagnosis at earlier stages, there has not been a corresponding increase in use of curative therapies and subsequent improvement in mortality. 8
Treatment options for HCC continue to be limited to patients with local disease. Historically, curative therapy included only surgical options, including resection and transplantation. In more recent years, radiofrequency ablation has offered a nonsurgical cure. 9 In patients with intermediate- to advanced-stage disease, only life-prolonging therapy, such as transarterial chemoembolization and sorafenib, rather than curative therapies are typically pursued.
Before the 1990s, HCC was a contraindication for orthotopic liver transplantation (OLT). Following a landmark retrospective study, the Milan Criteria was established, making OLT a treatment option for patients with unresectable HCC for solitary lesions <5 cm in size or up to three lesions each <3 cm. 10 Curative resection is not an option for some patients with HCC, and low model for end-stage liver disease (MELD) scores precluded the qualification for OLT in many patients. Therefore, in 2002, MELD exception points were granted to patients with HCC to increase the availability of OLT for patients with HCC. 11 These have been adjusted over the years to optimize the use of transplanted livers.
Because of the relative infrequency of HCC in the young adult (YA) population in the United States, most epidemiologic studies do not report the YA (<40 years) age group separately in large Surveillance, Epidemiology, and End Results program studies. In HBV endemic areas, the outcomes of YAs with HCC have been shown to be worse than in older patients.12–14 However, these outcomes are thought to be due to the higher stage of disease at diagnosis, and when adjusted for stage, YAs with lower stage disease have been actually shown to have a survival advantage. 15 In studies comparing YA and older patients who underwent partial hepatectomy, disease-free survival and event-free survival were not shown to be statistically different.16,17 No studies comparing outcomes of YA patients and older adult (OA) patients outside of HBV endemic areas exist to our knowledge.
Given the lack of curative treatment options for patients with HCC and the paucity of data surrounding OLT for YA patients with HCC, understanding the clinical and disease information in the YA population and OLT outcomes for this group is especially important. The objective of this study was to perform a comprehensive analysis of a large national transplantation registry in the United States to assess the characteristics and outcomes of YAs with HCC receiving OLT and compare these to older subjects >40 years with HCC receiving OLT.
Experimental Procedures
Study population
The study population included all YA patients between the ages of 18 and 40 with a diagnosis of HCC, who underwent liver transplantation from a cadaveric donor and had no previous liver transplants from the 1987 to 2012 United Network of Organ Sharing (UNOS) and Organ Procurement and Transplantation Network (OPTN) database. This is a retrospective analysis of de-identified data, and therefore, our local institutional review board was contacted for approval to complete this analysis and approval was granted. Diagnosis of HCC from the database was defined if the primary or secondary diagnosis at time of listing or the diagnosis at time of OLT indicated HCC or if there was an active MELD exception for HCC.
The liver transplant outcomes for the subset of subjects who received their transplantation following the implementation of MELD scoring were assessed. For the case–control analysis, a control group of patients older than 40 with a diagnosis of HCC (OA group) were matched on a basis of 4:1 to the post-MELD YAs with HCC (YA group) based on gender and MELD score (±1) using a greedy algorithm. 18 With the greedy algorithm, the YA subject was selected and matched with four OA control subjects with the closest propensity score based on defined covariates. Once a match was made, it was not reconsidered. All demographic data, laboratory values, MELD scores, and graft and patient survival were obtained from the database.
Statistical analysis
Data are presented as mean ± standard deviation or median [25th, 75th percentiles] for continuous variables and N (%) for categorical factors.
Patient/graft survival and retransplantation rates
Kaplan–Meier product limit estimates and Cox proportional hazards frailty models for clustered data were used to assess patient and graft survival. 19 Retransplantation was evaluated using competing risks analysis for clustered data as death precludes retransplantation. Time of follow-up was defined as months from transplant to event; subjects were censored at time of last visit and follow-up was truncated at 5 years.
Robust sandwich covariance matrix estimates were used to account for intracluster dependence due to matched pairs.
Case–control analysis
The study group (YAs with HCC) was compared to the control group (OAs with HCC) by univariable analysis to assess differences; because the groups were matched, conditional logistic regression and mixed linear regression analyses were used. Binary factors (two level) such as obesity or presence of diabetes were modeled using conditional logistic regression; separate models were built and each factor was modeled as the outcome with age group (YAs vs. OAs) as the independent variable. Similarly, mixed linear regression was used to assess differences in continuous variables such as age and body mass index (BMI). This was done using a natural logarithm transformation for the outcome variable and a variance component correlation matrix to model the intracluster correlation.
All analyses were performed using SAS version 9.4 (The SAS Institute, Cary, NC), and a p-value <0.05 was considered statistically significant.
Results
Patient demographics and secondary diagnoses
A total of 464 YA patients with HCC who received their first cadaveric liver transplant from 1987 to 2012 were found in the UNOS database and included in the analysis. The number of cases undergoing transplant increased dramatically in 2002, following the initiation of MELD-exception points (Fig. 1). Table 1 presents a summary of patient characteristics, including demographics, comorbidities, laboratory findings at the time of transplant, surgical information, and antirejection therapy following transplant. Rates of transplantation increased with increasing age (Fig. 2). The majority of patients were male (64%) and of white race (51.9%), followed by black. The majority of patients were of normal weight (55.2%). Few patients had diabetes (8.6%) or hypertension (6.0%). The most common underlying liver disease was hepatitis C (21.3%), followed by HBV (15.5%), and autoimmune/cholestatic disease (12.3%). The most common causes of autoimmune/cholestatic disease were autoimmune hepatitis (47.4%), primary sclerosing cholangitis (31.6%), primary biliary cirrhosis (12.3%), and secondary biliary cirrhosis (7.0%). Metabolic disease occurred in 2.8% of patients, including glycogen storage disease type 1 (38.5%), alpha-1-antitrypsin disease (30.8%), tyrosinemia (15.4%), primary oxalosis/oxaluria (7.7%), and Wilson's disease (7.7%). Few patients (5.8%) had alcoholic liver disease.
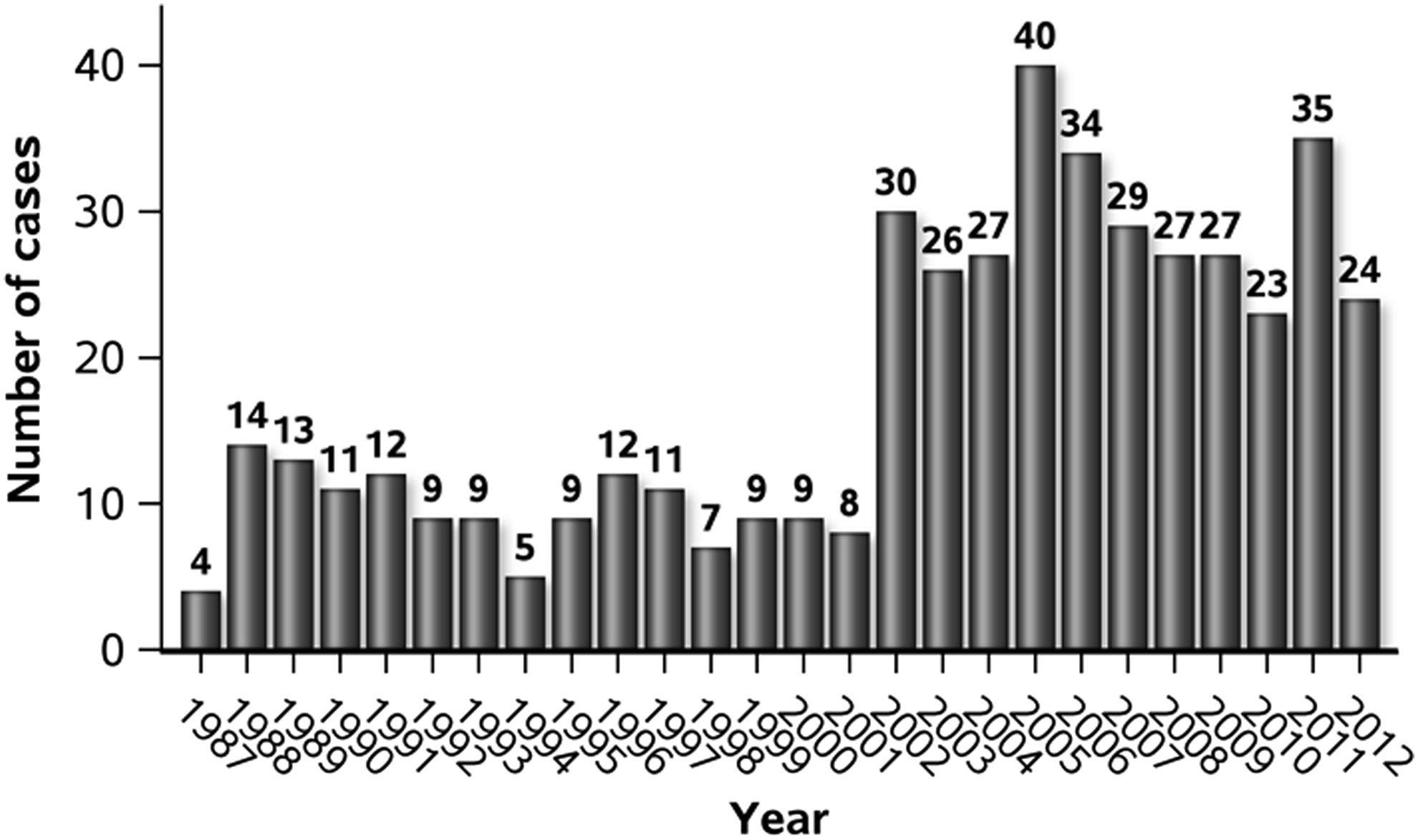
Number of liver transplants done in young adults for HCC. Analysis of the United Network for Organ Sharing database 1987–2012. HCC, hepatocellular carcinoma.

Age distribution of young adults undergoing liver transplantation for HCC.
Values presented as mean ± SD, median [P25, P75], or N (column %).
SD, standard deviation.
Comparison of patient characteristics for YAs with HCC who were listed and received transplant and those listed and did not receive transplant
A total of 639 YAs were listed for OLT from 1987 to 2012. Of those 639 patients, 175 (27.4%) did not receive an OLT (Table 2). There was no statistically significant difference in the gender, age, or BMI of the two groups. There was a difference in race, where patients of white and black race were transplanted more frequently than Hispanic or other race (p = 0.005).There was no statistically significant difference in comorbidities, including diabetes and hypertension. Associated liver diseases were similar between the two groups with more cholestatic liver diseases being in the transplanted group. Of the patients who had not been transplanted, 34.3% were still on the waitlist at the time of this data collection, 53.7% were removed from the waitlist, and 12.0% died while listed for transplant.
Statistics presented as mean ± SD, median [P25, P75], or N (column %).
Pearson's chi-square test.
Analysis of variance.
Fisher's exact test.
BMI, body mass index; MELD, model for end-stage liver disease; WL, waiting list.
Outcomes after first and second OLT for HCC in YAs
The outcomes of liver transplant in YAs with HCC from 1987 to 2012 are described in Table 3. In terms of survival, 58.8% of patients were alive or lost to follow-up without need for another transplant following their first OLT (235 patients alive and 38 lost to follow-up), 9.7% of patients required another transplant, and 31.5% of patients were deceased. The median survival time was 31.4 months. The most common reason for retransplantation was HCC (29.3%). In terms of the patients who died, the most common cause of death was malignancy (45.2%), followed by graft failure (16.4%) and then infection (11.0%).
Values presented as mean ± SD, median [P25, P75], or N (column %).
LT, liver transplant; OLT, orthotopic liver transplant; FU, follow-up.
Of the 45 patients requiring second OLT, 51.2% were alive or lost to follow-up (20 patients alive and one lost to follow-up), 12.2% required another OLT, and 36.6% were deceased. The median patient survival time was 47.7 months. The reason for retransplantation for the five patients requiring another OLT was acute liver failure, autoimmune/cholestatic disease, hepatitis C, and HCC. The most common cause of death was again malignancy (26.7%) followed by infection (20.0%).
Comparison of patient characteristics undergoing OLT for HCC between YA and older patients
Three hundred twenty YA patients were transplanted in the post-MELD era (after 2/27/2002). This group of patients was compared to OAs (41+ years). Table 4 presents the comparison of YA and OA characteristics of HCC transplant recipients. Compared to OAs, the YAs had significantly lower BMI (p < 0.001) and less diabetic comorbidity (<0.001). Race was also significantly different, with the older population having a larger white population, with less black and other race (p < 0.001). The underlying liver diseases between the two groups significantly varied. There was a higher frequency of HBV in the YA group (19.1% vs. 5.5%, p < 0.001), as was autoimmune/cholestatic disease (16.3% vs. 3.7%, p < 0.001), metabolic disease (3.4% vs. 1.3%, p = 0.012), and other tumors/cancer (4.4% vs. 1.3%, p = 0.002). The OAs had a higher amount of alcoholic liver disease (6.9% vs. 11.7%, p = 0.012), hepatitis C (23.3% vs. 56.6%, p < 0.001), and nonalcoholic steatohepatitis (NASH, 1.9% vs. 7.8%, p < 0.001).
Values presented as mean ± SD, median [P25, P75], or N (column %).
Conditional logistic regression was used to compare binary factors between the groups. Mixed linear regression was used for the continuous variables using a natural logarithm transformation; a variance component correlation matrix was used to model the intracluster correlation.
HBV, hepatitis B virus; HCV, hepatitis C virus; NASH, nonalcoholic steatohepatitis; DRI, donor risk index; LOS, length of stay.
At the time of transplant, YA patients had lower serum creatinine and higher albumin, with similar total bilirubin. Median patient survival time was similar, 29.4 months in the YA group and 26.0 months in the OA group (p = 0.46).
Comparison of survival and retransplantation outcomes after first OLT for HCC between YA and older patients
Figure 3 presents the 5-year survival and retransplantation cumulative rates comparing the YA and OA groups. Patient survival was higher in the YA group, but this did not reach statistical significance, with the risk of survival being 74.4% in the YA group and 68.6% in OA group (p = 0.093) (Fig. 3A). Graft survival was not different between the two groups, 66.3% in YA group and 65.4% in the OA group (p = 0.79) (Fig. 3B). The rate of retransplantation was significantly higher in the YA population (9.2% vs. 4.3%, p = 0.01) (Fig. 3C).

Five-year survival and retransplantation cumulative rates in the post-MELD era (2002–2012). Patient and graft survival values presented are survival estimates (95% CI) and are obtained from Cox proportional hazards frailty models for clustered data. Retransplantation values are cumulative incidence (95% CI) obtained from competing risks analysis for clustered data.
Discussion
This study is the first to address survival outcomes specifically for YA patients with HCC following therapy with curative intent in the United States. The principle findings of this study are (1) proportionally underlying liver disease leading to HCC is different between the YA and OA populations; (2) YA HCC patients had lower rates of comorbidities, including obesity, diabetes, and hypertension; and (3) survival outcomes were better, although not statistically significant, in the YA population and the rate of retransplantation was higher.
Curative treatment options for patients with HCC are still very limited, but advances in management bridging to transplant have allowed decreased dropout rate during the mandatory waiting period. 20 In addition, patients are being diagnosed at an earlier stage, potentially allowing for increased curative therapy. 8 There is hope that the incidence of HCC will decrease significantly because of improved hepatitis C virus (HCV) therapy. 21 This therapy is likely to delay the onset of HCC by halting continued inflammation against the virus, but is not projected to stop the progression of fibrosis eventually leading to HCC. 22 Although HCV is the most common underlying liver disease leading to HCC, proportionally HCV is less prevalent in the YA population. Because of this, the effect of improved therapies for HCV may have a less effect on transplants in YAs. HBV is more prevalent in the YA population when compared to the OA both in the United States and in HBV endemic countries, while the rate of HBV-associated HCC is much less in the United States than in other countries with endemic HBV. The YAs included in this study during the post-MELD era should have been offered vaccination, as HBV vaccination has been available in the United States since 1981. Therefore, the importance of vaccinating against this cancer-causing virus should be stressed with all families.
Metabolic risk factors such as obesity and diabetes are associated with HCC development, and although not seen in the majority of the patients in this study, the obesity epidemic and increased rates of diabetes in children, adolescents, and YAs will likely impact HCC in this younger population. Prevalence of pediatric nonalcoholic fatty liver disease (NAFLD), a known consequence of metabolic syndrome, has more than doubled over the last 20 years and is expected to continue to rise. NAFLD and NASH can progress to liver cirrhosis and subsequently lead to HCC. The yearly cumulative incidence of HCC in patients with NASH cirrhosis has been estimated at 2.6% per year compared to 4.0% in patients with HCV-induced cirrhosis. 23 With children developing NAFLD and NASH at younger ages, an increase in HCC in these populations can be expected. This is also concerning because NASH has been shown to recur in transplanted livers in YAs, and patients transplanted for NASH have higher retransplantation rates in this age group than other liver diseases requiring transplant. 24
Survival outcomes in YA patients with HCC in HBV endemic countries have been thought to be worse than OAs. This has been postulated to be due to advanced stage at diagnosis and in patients with lower stage disease, the outcomes after hepatectomy have been reported as slightly worse or equal to OAs.15–17 This is the first study to evaluate OLT outcomes of HCC and the first to report better survival outcomes in the YA age group compared to OAs. Because of the younger age and better survival, there are potentially more life-years saved in transplanting a younger patient.
The main strength of the study is the use of a large nationally representative OLT database, which allowed evaluation of the characteristics and outcomes of HCC as an indication for OLT in YA patients and compared this group to OAs. The study has several limitations mainly inherent in the use of large registry database studies. The assignment of HCC as the primary indication for OLT cannot be confirmed by an independent mechanism and errors in coding can occur. In addition, pertinent clinical information, including portal vein invasion, portal hypertension, size and number of tumors, presence of metastatic disease, and tumor histology, is not consistently reported to the database. Also, no data regarding bridging locoregional or systemic therapy are available in this database.
Although HCC is typically a disease of OAs, 464 YAs with HCC received OLT in the UNOS database from 1987 to 2012. Compared to the older population, the YA group had higher survival and retransplantation rates. HBV, a vaccine preventable illness, was more frequently associated with HCC in younger patients. The MELD-exception for HCC has allowed an increased number of YAs with HCC to receive OLT who would have otherwise had little hope for long-term survival.
Footnotes
Author Disclosure Statement
No competing financial interests exist.