
Abstract
Nasal Type T/natural killer (NK)-cell lymphomas are rare clinical entities, highly aggressive with a very poor prognosis. We present a case of a 37-year-old immunocompetent man presenting with deep palatal ulceration and a 3-month history of symptoms, which appear to have been misdiagnosed by physicians. The final diagnosis was achieved by a 15-day diagnostic algorithm, during which time the clinical status of the patient worsened severely. In this article, we also provide a succinct update on the clinical and histopathological findings of Peripheral T/NK-cell lymphomas and propose that symptoms that are consistent with these clinical entities should be considered from the early stages to inform a suitable diagnostic pathway Because of their highly aggressive behavior, we suggest that early therapy of T/NK-cell lymphomas may be started before completing the specific diagnostic investigations.
Introduction
L
NK cells are a third lymphocyte lineage, in addition to B- and T-cells, that mediate cytotoxicity without prior sensitization. NK cells also have phenotypic and genotypic characteristics; they express the NK-related antigen CD56 and T-cell markers such as CD2 and CD3 epsilon, but their T-cell receptor locus is not rearranged. 1
Included in the NHL group are the Peripheral T-cell and NK-cell lymphomas (PTNKCLs), a wide family of lymphomas with different clinicopathologic features, which represent only 10%–20% of all NHLs in the Western world. 2
PTNKCLs are defined as angiocentric lymphomas in the revised European American Lymphoma (REAL) classification and include the “nasal” and the “nasal type” varieties, which are very rare clinical entities in the United States and Europe, but more common in Asia and Central America. 3 Nasal T/NK cell lymphoma is a distinct clinicopathologic entity that is highly associated with Epstein-Barr virus (EBV), with a very poor response to treatment and prognosis (5-year overall survival rate of 25%).3–6
Generally, a variety of cells ranging from small or medium-sized cells to large transformed cells can characterize the broad cytologic spectrum of this entity. Tissue damage is a common morphological feature of this form, due to both cytotoxicity of the T/NK lymphoma cells and angiocentricity.4,5,7
The characteristic immunophenotype of Nasal T/NK cell lymphoma is distinguished by a CD2 and CD56 positivity, but usually a negativity for surface CD3.
The presence of EBV in early diagnosis can be effectively evaluated by in situ hybridization.
The differential diagnosis includes lymphomatoid granulomatosis, blastic or monomorphic NK cell lymphoma/leukemia, CD56-positive peripheral T-cell lymphoma, and enteropathy-associated T-cell lymphoma. 4
Extranodal sites such as the skin, the subcutis, and the gastrointestinal tract can be affected by tumors with an identical phenotype and genotype. These extranodal forms should be referred to as nasal-type T/NK cell lymphomas. 4
Here, we present a rare case of a 37-year-old Caucasian man affected by nasal-type T/NK-cell lymphoma, referred to our unit 3 months after the development of the first symptoms.
The purpose of this study is to update data on the clinical and histopathological findings of this rare disease, pointing out how misdiagnoses are responsible for therapeutic delays and, consequently, of a worse prognosis for these aggressive forms.
Case Report
A 37-year-old Caucasian man was referred to our Oral Medicine Unit, Department of Head and Neck Diseases, Federico II University of Naples, in September 2014 with the main complaint of a wide symptomatic ulcerative lesion of the hard palate.
His family history encompasses three uncles who had died of different forms of cancer in recent years (two of lung cancer, and one of bowel cancer). The patient's medical history was negative, and he was in apparent good health except for a weak hypercholesterolemia.
His first referred symptoms were a moderate submandibular lymphadenopathy and weak fever starting more than 2 months earlier, for which reason he consulted the family doctor who requested hematological tests with the main suspicion of an EBV/CMV infection. The results of all the tests performed were negative and for 1 month the patient received symptomatic therapy. With no sign of improvement, 4 weeks later the patient started complaining of a sense of nasal obstruction, with breathing difficulty for which he consulted an otorhinolaryngologist who performed an endoscopic examination of the nasal cavities, finding suppurative exudate and inflammation of the nasal floor and lateral/medial walls. It was diagnosed as severe maxillary sinusitis and therapy with corticosteroids through an aerosol, and antibiotics were prescribed. After 1 month, without any improvement of the symptoms, the patient started complaining of the first oral symptom, pain due to swelling, and an ulcerated area in the median area of the hard palate. For this reason, he consulted his dentist who advised him to undergo an oral medicine consultation at our hospital. Our first examination was performed soon after, accordingly 10 weeks after the onset of the first symptoms, and the patient was presented with the clinical condition shown in Figure 1A.
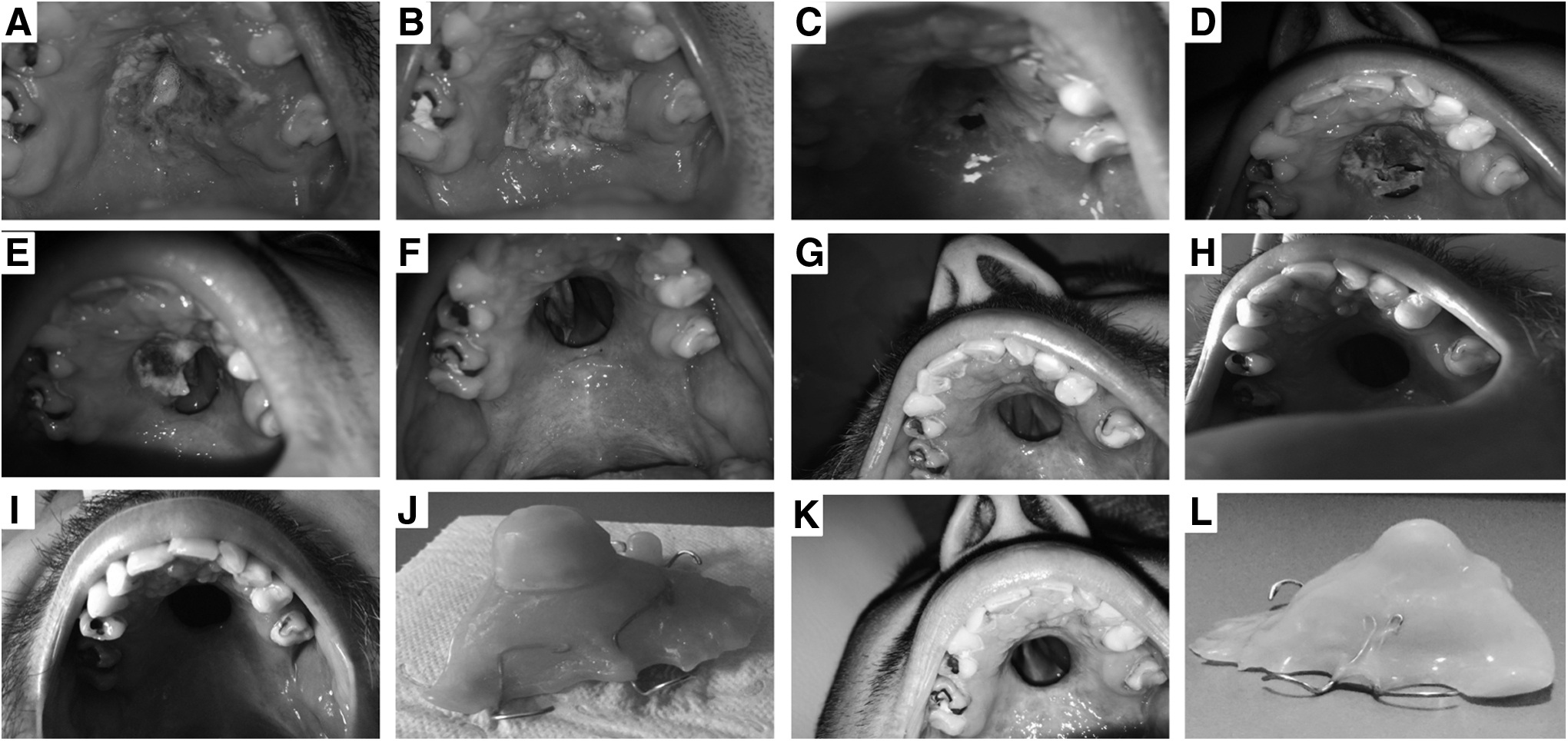
Intraoral clinical aspect at initial presentation in Oral Medicine. The hard palate and the alveolar process presented with an ulcerative and destructive lesion with an extensive zone of necrosis
The patient, after providing his written informed consent, was hospitalized and examined by routine hematological tests, which revealed a glucose level of 120 mg/dL (normal range, 60–110), a total cholesterol level of 200 mg/dL (normal value up to 190), a triglyceride level of 218 mg/dL (normal value up to 180), and an iron level of 49 μg/dL (normal range, 55–160).
The physical examination showed a widespread ulcerative and proliferative lesion involving the hard palate, and marginally the soft palate and the left maxillary alveolar process (Fig. 1A). The lesion measured about 4 cm at its maximum diameter and showed a central zone of deep and extensive necrosis, with a surrounding area of weakly brown-colored hyperplastic tissue. Two incisional biopsies of the lesion were performed.
After 2 weeks, while the patient was undergoing a diagnostic pathway, the lesion presented with a considerably worse clinical evolution, as shown in Figure 1B.
At histology, scanning magnification revealed a dense and diffuse proliferation of pleomorphic small and medium-sized lymphocytes within the entire chorion, with overlying extensive squamous epithelium ulceration. An angiocentric pattern of infiltration was evident. The predominant cell type was lymphocyte with round nuclei, one or more nucleoli, and a scant cytoplasm. Numerous mitotic figures were seen, and areas of necrosis were also present (Fig. 2A–C).

Extranodal NK/T-cell lymphoma, nasal type.
The neoplastic cells expressed CD2 and CD3; a weak expression of CD56 and granzyme B was observed (Fig. 2D). CD8 and CD30 were consistently negative. The tumor had a proliferative fraction (Ki-67/MIB1) approaching ∼70%–75%. The analysis of the presence of EBV was performed with the FISH (fluorescent in situ hybridization) technique (Dako PNA ISH EBERER PNA Probe) and revealed a widespread positivity for EBV.
A diagnosis of extranodal NK/T-cell lymphoma, nasal type was made.
The patient was immediately referred to the Hematoncology Department to complete the staging and start treatment of the disease. A head/neck and chest computed tomography (CT) scan and a total body positron emission tomography (PET) scan were negative except for the oral and left nasal cavity involvement. Chemotherapy following the SMILE protocol (Methotrexate 2 g/m2 IV, Dexamethasone 40 mg IV + leucovorin 15 mg × 4 doses/day IV + ifosfamide 1500 mg/m2 IV + etoposide 100 mg/m2 IV, and
The study was approved by the Ethics Committee of the University “Federico II” of Naples. Appropriate written informed consent was obtained from the patient included in the study.
Discussion
The head and neck is a common site of extranodal NHL. PTNKCLs are rare and heterogeneous forms of NHL that are usually characterized by a very poor clinical outcome. Furthermore, many subtypes are currently present in the World Health Organization (WHO) classification of PTCL. 8
Sequential chemotherapy and radiotherapy is the gold standard treatment for extranodal lymphomas at early stages (I–II), proved to be more effective in terms of 5-year overall survival and progression-free survival than chemotherapy or radiotherapy alone. For stage III/IV instead, chemotherapy is the mainstay of treatment. Conventional anthracycline-based regimens are ineffective. Since the advent of
As confirmed by this present case, the diagnosis of these forms is difficult for the general practitioner as well as for medical specialists, a difficulty compounded by the frequent underestimation/misdiagnosis of the first symptoms that are often non-specific and can mimic an inflammatory process. Each failure in a diagnostic step is usually followed by a delay of several weeks for the patient to achieve the correct diagnosis and to undergo the specific therapy. Given that the specific treatment strategy and related prognosis for a patient with NHL strictly depend on disease stage, this diagnostic delay can seriously impact patients' lives.
Because of the relative rarity of this condition, achieving the correct diagnosis can be a challenge, even for pathologists. In a recent study conducted before the most recent WHO classification, the overall diagnostic accuracy among experts was found to be ∼81%, with a value ranging from 67% to 95% depending on the specific subtype. 12
In our case, prompt biopsies and histopathological examination led us to a diagnosis in only 2 weeks, but unfortunately the patient had already undergone a 3 month delay since the first medical examination. We speculate that such extended delays could jeopardize a patient's life, and can surely contribute to the extensive damage to the nasal floor and surrounding structures, with a consequent permanent wound that is hard to manage and impacts the patients' quality of life.
The head and neck healthcare specialists may be considered the main actors in the diagnostic pathway of these rare diseases. Lack of response to first treatments must induce physicians to increase level of suspicion and to refer their patients for further examination as appropriate. The first observation/waiting period must be not longer than 2 weeks, and it should be followed by a histopathological examination in all uncertain cases.
In this case, the patient had been treated symptomatically for a persistent unspecified peripheral lymphadenopathy for the first 4 weeks without any improvement, and without performing any further investigations. Next, management of the patient by the ENT specialist for a further 4 weeks for an alleged sinusitis was even bordering on negligence. In such a patient, after the first 3–4 weeks of observation, lymph node biopsy was already required. It should be highlighted that imaging, for example, a simple head and neck ultrasound, could have been useful to identify node characteristics more accurately than the physical examination only. It is well established that a change in the long: short axis ratio of a node is a significant sign of lymphoma and metastatic cancer. Furthermore, fine needle aspiration cytology (FNAC) is a simple and safe procedure and is proved to be accurate in the diagnosis of reactive hyperplasia, infections, granulomatous lymphadenopathies, lymphomas, and metastatic malignancies. The accuracy of image-guided lymph nodes biopsy by FNAC in diagnosing lymphoma and metastatic cancer has been reported to be in the range of 76%–100% and 82%–96%, respectively. 13 Further examinations such as maxillofacial CT scan could have been useful to have initial staging of the disease since the first visits.
Based on this experience, it is arguably undesirable to wait even three days in respect of these forms of lymphomas in which the cytotoxicity and angiocentricity can produce such a fast and deep necrosis. The grievous impairment of the surrounding anatomical structures is the main complication that contributes to the already very poor prognosis.
Furthermore, in these highly aggressive forms, the possibility of starting a therapy before completing the diagnostic pathway should be evaluated. Starting an earlier therapy could make a significant difference in improving such poor survival rates.
Footnotes
Author Disclosure Statement
No competing financial interests exist.