
Abstract
Purpose:
Adolescents and young adults (AYAs) receiving cancer treatments that may impair fertility should receive counseling about risk of infertility and options for fertility preservation (FP) before treatment and/or during survivorship. Our objective was to define the AYA patient population referred to an on-site fertility consultation service within a comprehensive cancer center and determine factors associated with patients proceeding with FP treatment.
Methods:
We conducted a retrospective chart review of AYA women who completed a consultation at the MD Anderson Fertility Preservation and Family Building Service during the first year of service. Records of 154 referred AYA patients were reviewed for age, ethnicity, cancer type gravidity and parity, survivorship status, and decision to pursue FP treatment.
Results:
Patients (mean age 29.7) were Caucasian (55%), Hispanic (23%), and African American (10%). The majority of women (67%) were seen for FP before cancer treatment and the remaining sought options for family building while in survivorship. The most common cancer types were hematologic (29%), breast (25%), and gynecologic (23%).
Conclusions:
Patients referred to an on-site fertility consultation service were medically and ethnically diverse. Interest in fertility counseling and treatment was apparent in both survivorship pre- and postcancer treatment. Although the referral group was ethnically diverse, Caucasian women were most likely to pursue FP treatment compared to women of other ethnicities.
Background
T
Timely referral for FP consultation is paramount. Early consultation is associated with both lower decisional conflict 5 and increased likelihood of pursuing FP. 6 For breast cancer patients, referral before breast surgery, compared to postsurgical referral, is associated with earlier initiation of FP treatment and more ovarian stimulation cycles, 7 allowing optimal chances of cryopreservation of oocytes or embryos without delaying oncology treatment. FP options are especially applicable to AYA patients, who may have various reproductive concerns and fertility-related distress after treatment, 2 which may affect other areas of psychosocial functioning. Logistics of FP referrals can prevent timely consultation visits, with an average of 1 week between referral and a consultation visit with a reproductive endocrinology (RE) specialist. 8 Attempts to bridge this gap between oncology and reproductive clinics, as well as to offer the equivalent counseling to all women, have included providing FP training programs for oncology care professionals, 9 placing patient education brochures in waiting rooms, 10 and institutional policies for referral to FP services. 11 Thus, developing a rapid, integrated, on-site fertility consultation service within cancer care settings can decrease the burden on oncologists seeking to counsel patients regarding fertility options, while allowing patients to explore FP options in a time-sensitive manner.
Nationally, nearly half of all oncologists at academic medical centers reportedly do not routinely refer patients to RE specialists,11–15 further supported by the observation that half of patients in survivorship do not recall receiving reproductive health counseling at the time of cancer diagnosis.15,16 Barriers in pursuing FP consultation before oncologic treatments include the perceived urgent need for treatment, oncologist referral patterns, emphasis on survival over FP, psychological stress, and cost of FP.11,17,18 Demographic differences in oncology providers may influence referral rates; younger female physicians, gynecological oncologists, and physicians working in multidisciplinary environments are more likely to refer for FP and to have more positive attitudes and behavior toward FP.12,13,19 Published rates of FP treatment are quite variable, with rates of FP treatment ranging from 4% to 71%.15,20,21
An on-site FP center incorporated in a large cancer center may help alleviate the logistical burden of providing comprehensive, time-sensitive fertility counseling and, in turn, provide FP counseling and treatments to all AYAs interested. In recognition of these needs and challenges, MD Anderson Cancer Center, in conjunction with the Baylor College of Medicine, now provides an on-site fertility consultation service that offers same-day fertility counseling and treatment. Our objective is to describe the AYA patient population, referral volume, survivorship, and subsequent use of assisted reproductive technology (ART) for FP by patients referred to our fertility consultation service within a comprehensive cancer center during its first year of operation.
Methods
The study was approved by the MD Anderson Institutional Review Board. Medical records of patients referred and subsequently seen at the MD Anderson Fertility Preservation and Family Building Service in a 1-year period from 2013 to 2014 were reviewed. This on-site Fertility Preservation and Family Building Service was established by the MD Anderson impetus to meet the recognized need of proximate FP services, as ∼1700 AYA patients with a newly diagnosed malignancy are seen annually at the comprehensive cancer center. Consequently, with formation of the FP program, a reproductive endocrinologist was recruited to the faculty to fulfill this role. This collaborative effort was therefore designed to allow the patient's oncology provider and reproductive endocrinologist to provide a multidisciplinary approach to address the individual patient's FP needs before treatment or in survivorship. For our purposes, we included patients designated AYA according to the National Cancer Institute's defined age range of 15–39 years old.
The patient's physician (oncologist or nononcologist), physician assistant, or advanced nurse practitioner provides the initial referral for FP, and consults are seen within 24–48 hours, with a majority seen the same day. The FP consultation clinic is located within the outpatient cancer treatment center, and inpatient referrals are also provided if needed. All the patients received FP counseling from the same RE provider, who would also provide FP services at a facility located adjacent to the consultation clinic, if the patient elected to proceed. This clinic provides counseling for any women interested in discussing fertility-related outcomes of her oncologic treatment, follow-up during and/or after her treatment, as well as options for FP.
The initial consultation visit includes obtaining and reviewing the patient's medical, surgical, social, and obstetrical/gynecological history. An anti-Mullerian hormone level and pelvic ultrasound are obtained before the visit or on the day of consultation to enhance individual counseling of suitability for use of FP. The patient's oncologic diagnosis and planned treatment plans are available to the FP physician through electronic chart review or personal communication with the primary oncologist. In cases in which staging, final diagnosis, and treatment plans are contingent on a pending pathologic tissue diagnosis, the patient is counseled regarding options based on several possible treatment plans. Thus, patients whose oncological plan is not definite are seen at an initial consultation to discuss options and then counseled again after a treatment plan has been made.
During the initial consultation, the individualized risk of loss of ovarian function or future fertility is reviewed with the patient. All FP options are discussed, including no FP treatment, or ovarian stimulation for oocyte or embryo cryopreservation. The process of ovarian stimulation, ultrasounds, and oocyte retrieval is reviewed. The patients and family support members are given opportunity to ask questions and seek clarification on the counseling information. The costs of FP treatment are a combination of the patient's insurance provider, out-of-pocket, or through a national nonprofit organization, which may supply some or all of the medication or treatment for ovarian stimulation. In our FP clinic, patient information, including demographics, insurance, and obstetrical and medical history, prior oncology treatments, and cancer type and treatment plan were recorded. In addition, patients who decided to pursue FP were further described. Statistical analysis was performed with one-way ANOVA, followed by two-tailed independent sample Student's t-tests in R-Studio with the R commander package (R-Studio, Inc., Boston, MA). p-Values less than 0.05 were defined as statistically significant, and smaller p-values were denoted as such (*p < 0.005, ** p < 0.0005).
Results
Within this first 1-year period, a total of 154 AYA women were seen by our reproductive endocrinologist as a formal new patient consultation in the FP clinic. The mean age of the women seen was 29.7 years (SD ±6.2) with a range from 15 to 39 years (Table 1), with equal distribution across age ranges. The most reported ethnicities were Caucasian (55%), Hispanic (23%), and African American (10%). The most common cancer types represented were hematologic (44/154, 29%), breast (38/154, 25%), and gynecologic (36/154, 23%); however, the remaining 36 patients presented with more than 12 other types of cancer. The numbers of single and married/partnered women seen in consultation were nearly equal (48% vs. 46%, respectively), and a majority had no living children. Of the female patients referred, 104/154 (67%) were referred for discussions of FP options before cancer treatment. In addition, the three most common diagnostic categories had represented uniquely different age populations, with the mean ages for hematologic, gynecologic, and breast subgroups of 26.8, 30.6, and 34.1 years, respectively (all comparison p-values <0.005), as shown in Figure 1. Of all patients seen for FP consultation, a majority of patients (85%) were covered by private insurance, while 10% were uninsured/self-pay, and 5% had Medicaid/Medicare insurance, as show in Table 2. In addition, when insurance coverage within each ethnic group was examined, 97% of Hispanic patients had private insurance, followed by Caucasian (85%), Asian (83%), and African American (75%) patients.
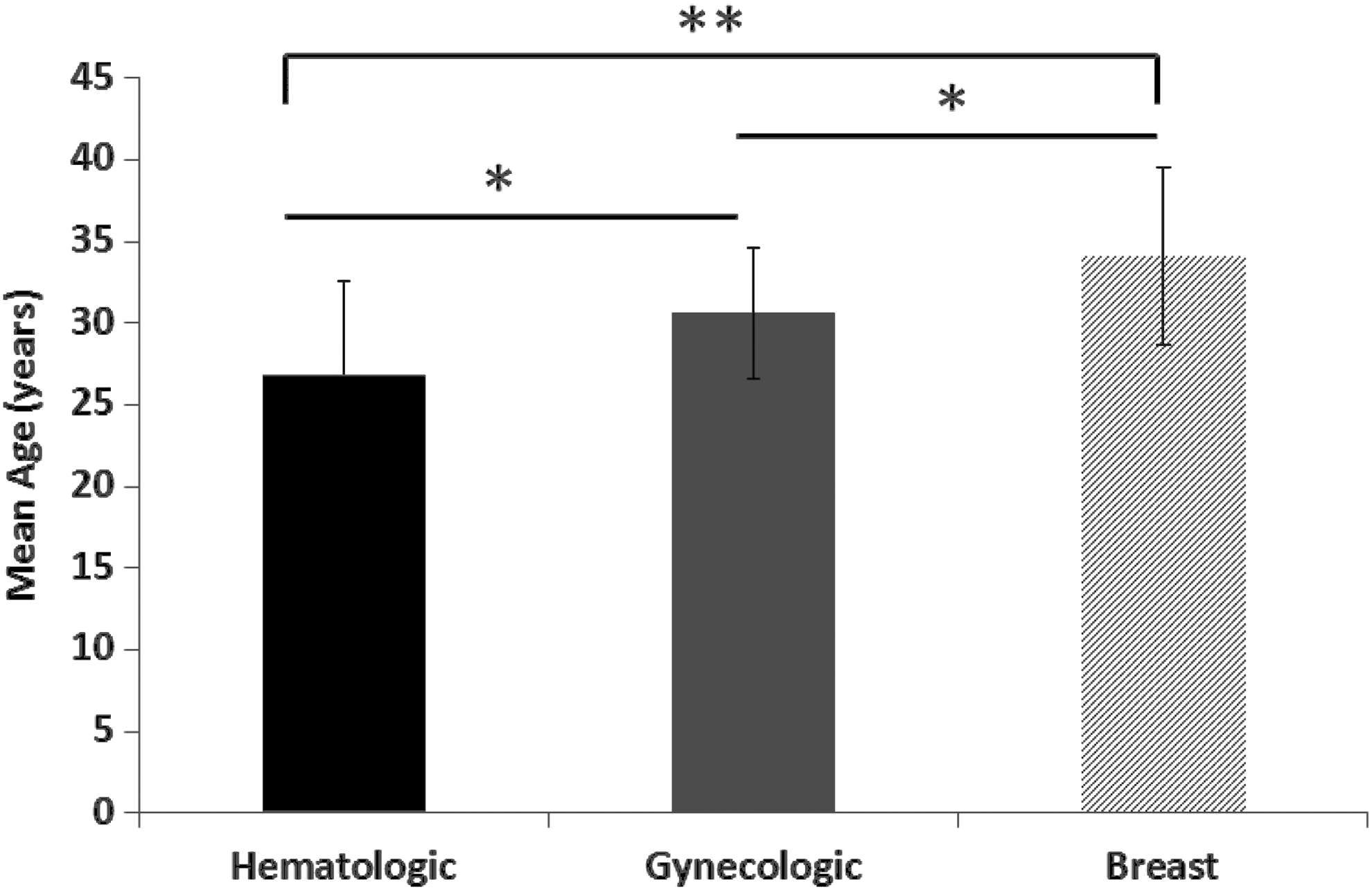
The mean ages of AYA patients within the three subgroups of most commonly represented oncologic diagnoses (hematologic n = 44, gynecologic n = 36, and breast n = 38) were determined, with mean ages of 26.8, 30.6, and 34.1 years, respectively (*p < 0.005, **p < 0.0005). AYA, adolescent and young adult.
FP, fertility preservation.
During this consultation period, 17 patients elected to preserve fertility through oocyte or embryo cryopreservation (Table 3). Within this subset of women electing to pursue FP, ages ranged from 21 to 38 years, with a mean age of 29.6 years. The most common diagnoses for women undergoing FP treatment were breast and hematologic malignancies. Of these patients, a majority (71%) had never been pregnant. Of women who pursued FP treatment, 82% were Caucasian; none of the 35 Hispanic women seen in our consultation clinic decided to pursue FP treatment.
Discussion
The AYA patients referred during the first year of an on-site fertility consultation service within a comprehensive cancer center represented an ethnically and medically diverse group of women. Over 150 AYAs received consultation during the initial year, highlighting patient interest in these services. This service allows women to participate in FP counseling and for them to make best personal decision whether to proceed with FP treatment. For women facing a new cancer diagnosis, knowledge of FP options is important to many women, 22 and the ability for coordination of care with same-day on-site access to counseling by an RE physician alleviates many of the logistical burdens and psychological stress associated with FP consultation.
Our AYA patients had a variety of cancer diagnoses, with the most prevalent being hematologic, breast, and gynecologic malignancies, which are consistent with prior published demographics of a similar patient referral population. 23 However, our patient population was more ethnically diverse, more likely to have living children, and less likely to be partnered than other cohorts described in FP referral clinics.8,23 More than a third of patients presented to discuss fertility and family building in survivorship, emphasizing the need for oncologists and other members of the healthcare team to readdress fertility concerns and to refer AYA patients even after treatment has begun or concluded. In addition, as age is a crucial prognostic factor for women wishing to preserve fertility, it is important to recognize that the three most commonly referred diagnoses in the AYA population (hematologic, gynecologic, and breast) represent women in distinct reproductive age groups. Women referred with a hematologic diagnosis are significantly younger than women with breast cancer diagnosis (26.8 and 34.1 years, respectively) and may therefore have uniquely different prognostic factors for FP outcomes, as well as social factors in their exploration of FP.
It is encouraging that patients referred for FP services were ethnically diverse. However, Caucasian women were more likely to pursue FP treatments compared to African American or Asian women. In addition, none of the 35 Hispanic patients who received FP counseling chose to pursue FP treatments. While racial disparities in fertility treatments and FP have been described previously,15,24,25 these inequalities were reported in access to care and referral rates. Our study is the first to describe continued ethnic disparities in FP treatment even when all AYA women are provided equivalent, timely FP consultation. In addition, although none of the Hispanic women pursued FP treatments, this group had the highest rate of private insurance coverage (97%) among all ethnic groups. While specific patient income parameters and socioeconomic status were unable to be recorded, the high rate of private insurance within our Hispanic population makes it less likely that there exists a significant monetary barrier in pursuing FP treatments compared to the other ethnic groups our clinic served. Future research specifically examining an individual's decision process for pursuing FP, especially in the context of cultural or social influences, would help elucidate important patient-specific concerns and allow improved discussion of FP options for all ethnicities. While ethnic disparities and individual cultural influence in FP treatment were not within the original scope of this research, these observational differences warrant further investigation into possible racial and ethnic factors contributing to the decision process in an individual's choice of FP treatment.
Even for patients who decide not to pursue FP treatments, consultation before oncologic treatment or in survivorship provides several benefits. Fertility consultations have been shown to improve quality of life in women of reproductive age, whether they pursue FP treatment or not.14,26 Given that young women are particularly at risk for emotional distress regarding fertility in situations of uncertainty and limited knowledge, 2 providing counseling, even in cases where patients do no pursue FP treatment, is beneficial. It establishes a connection between the patient and the program, who is encouraged to have follow-up after treatment is completed to reassess her fertility potential. As fertility-related anxiety remains for AYA women after they have moved past their cancer experience, 27 the importance of accessible FP services in survivorship permits options for women who consider building a family. Same-day referral and consultation provided by this program empower and enable patients to make timely informed decisions about family building, in the event that they suffer from a shortened reproductive window. This on-site service provides personal fertility assessment and information, which is often identified as an unaddressed desire for these young women in survivorship. 28
With the benefit of the on-site fertility program within the cancer center, patients are offered timely and comprehensive FP counseling, often within 24 hours of the oncologists' referral. Compared to other published reports of an average of 7 days between oncologist referral and consultation visit, 8 our referral system notably decreases the time between oncologist referral and consultation visit. Our on-site clinic permits most patients to be referred and seen on the day of their oncology visits, alleviating the logistical and time-sensitive barriers. This timely and collaborative approach allows for improved fluidity of the consultation process, direct communication between providers, and a system which provides long-term care for patients within one facility. The fertility counseling and services through the Fertility Preservation and Family Building program at MD Anderson provide rapid, streamlined interdisciplinary care that can assist patients with their family-building needs. Even at larger cancer centers with FP programs in place, oncologist referral rate may be subject to inherent physician bias such as perceived severity of diagnosis, necessity of FP, or lack of “clinical consciousness” in incorporating the referral into counseling. 11 Providing an integrated on-site FP program staffed by an RE physician may help eliminate the heterogeneity of the oncologists' referral preferences and patterns.
We conclude that establishment of an on-site fertility clinic within a comprehensive cancer medical center successfully serves a medically and demographically diverse population of AYA patients and survivors while reducing the logistical barrier of off-site referral systems. We believe that our findings further support the need, feasibility, and patient interest in on-site FP consultation services within comprehensive cancer centers that are able to provide timely FP counseling to the AYA patient population.
Footnotes
Acknowledgment
We gratefully acknowledge Ms. Carolyn Schum for editorial help with the preparation of this article.
Author Disclosure Statement
No competing financial interests exist.