
Abstract
Purpose:
Decisions surrounding fertility preservation (FP) in children, adolescents, and adults can be difficult due to the distress of a cancer diagnosis, time constraints for decision-making, and lack of efficacy data. This review examines the decision-making process of oncology patients and their parents (if patients are in the pediatric or adolescent population) to better understand experiences of decisional conflict and regret.
Methods:
Two electronic databases, Embase and Pubmed, were searched using the terms (Decision-making OR Conflict (Psychology) OR Decision regret) AND (Freezing OR Oocyte OR Ovarian tissue OR Semen preservation OR Fertility preservation OR Cryopreservation) AND (Neoplasms OR Cancer OR Chemotherapy OR Drug therapy OR Radiotherapy). Medical Subject Heading terms were utilized where possible. Included articles discussed FP decision-making from the patient's perspective.
Results:
Thirty-five articles discussing FP decision-making were included (24 in the adult population, 11 in the pediatric and adolescent population). Key themes from these articles included the following: factors considered in FP decision-making, decision-making in established procedures and experimental procedures, decisional conflict and regret, the perceived importance of information, adolescent involvement in decision-making, and ethical considerations in the pediatric population.
Conclusions:
Unique ethical issues arise in the pediatric and adolescent population. Considering that the decision to pursue FP is known to be difficult in the adult population, decisional conflict and regret may be greater for parents who are making the decision for their child.
Introduction
W
Due to the potentially detrimental effects of chemotherapy and radiotherapy on future fertility, international bodies, including the American Society of Clinical Oncology (ASCO) and the National Institute for Health and Care Excellence (NICE), recommend discussion of the risks of cancer therapy on fertility and options for preservation with all patients before initiation of any therapy.5,6
Fertility preservation (FP) includes discussion about future fertility risks and provision of strategies to minimize cancer treatment impacts on fertility. 7 Currently, the types of FP techniques available include the cryopreservation of ovarian tissue, testicular tissue, sperm or oocytes before treatment. 8
In children and adolescents, FP decisions pose unique challenges due to limited efficacy of the reproductive technologies (providing no guarantee of having a child), ethical and legal barriers, lack of models of care, cost, poor communication, and the triadic nature of discussions involving the clinician, parent, and young person.9,10
Therefore, it is important to examine the FP process to better understand experiences of uncertainty (decisional conflict) and regret in patients and parents, with the goal to improve clinical pathways and develop effective interventions that facilitate informed decision-making.
This review aims to elucidate the factors that reduce the risk of decisional regret and decisional conflict around FP decisions in oncology patients. Patient and family decision-making in the context of the ethical issues surrounding FP in children and adolescents will also be explored.
Methods
An electronic databases search was performed (using Pubmed and Embase) for articles published before September 2015 matching the following search terms: (Decision-making OR Conflict (Psychology) OR Decision regret) AND (Freezing OR Oocyte OR Ovarian tissue OR Semen preservation OR Fertility Preservation OR Cryopreservation) AND (Neoplasms OR Cancer OR Chemotherapy OR Drug therapy OR Radiotherapy). Medical Subject Headings were utilized where possible. Search results produced 95 unique publications. A further four publications were included as recommended by the authors. Literature reviews discussing decision-making, conference abstracts, and articles discussing ethical issues in the pediatric population were included. Guidelines, commentaries, articles that focused on FP in specific genetic mutations, conference abstracts, and pilot study data that were also reported in a published study already included in the review were excluded.
Results
The search results are shown in Figure 1. Thirty-five articles were included in this review. Studies were categorized according to the age of participants, as pediatric (<12 years), adolescent (12–18 years), or adult (>18 years). Of the 35 articles, 24 were in the adult population and 11 in the pediatric and adolescent population. All adult studies in this review discussed decision-making. Seven pediatric and adolescent studies discussed decision-making and four discussed ethical considerations surrounding the fertility decision.
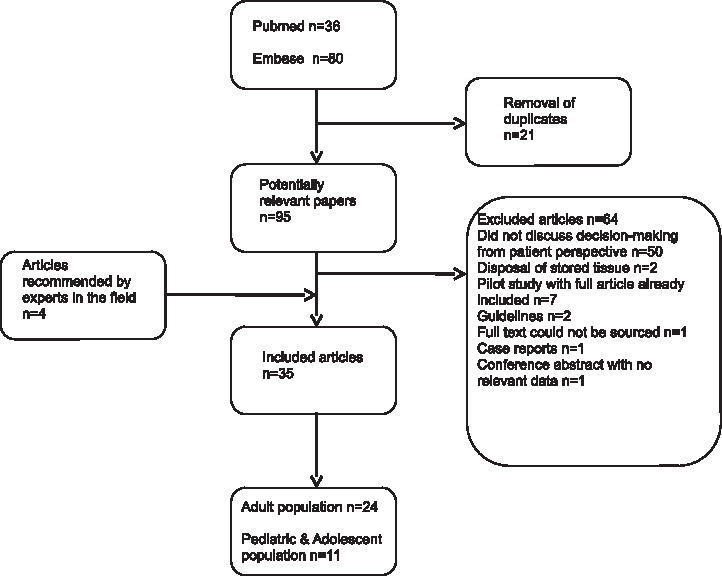
Criteria used to include and excluded potential research articles.
There were 24 cross-sectional studies, four cohort studies, three literature reviews, and four were ethical discussions in pediatric FP. Of the three literature reviews, two discussed FP decision-making in an adolescent population and one discussed sperm banking decisions in adult men.
Research in the adult population
Twenty-four articles investigated fertility decision-making in the adult oncology population. These can be found in Table 1. Articles have been grouped under the following themes: factors considered in FP decision-making,11–21 decisional conflict and regret in FP decision-making,22–25 and the importance of information in addressing decisional conflict and regret.22,23,26–34
FP, fertility preservation; N/A, not applicable; NS, not specified.
Factors considered in decisions to preserve fertility
Eleven articles discussed factors taken into account when making fertility decisions. Of these, 10 contained original data11–17,19–21 and 1 was a systematic review. 18 The effect of FP on the oncology treatment plan was a significant concern for both sexes.12,14,15,19 In women, delaying cancer therapy for oocyte harvesting was rated among the three most important concerns. 12
Potential infertility also was an important factor, with 51% of young women with breast cancer (n = 620) reporting some anxiety around the issue. 16 Furthermore, 26% considered or pursued suboptimal cancer treatment due to fertility concerns. 16 FP was perceived to be a type of “insurance” or “backup plan” and, gave young women with breast cancer a sense of power if they had ovarian failure post-treatment. 14 The intensity of the desire to conceive a child in the future and having a stable partner relationship are shown to play a key role in decision-making. 21
Patients were concerned about the invasive nature and possible side effects of FP and the potential harm to future offspring (risk of abnormalities from cryopreserved sperm).18,19,21 The financial costs associated with FP were also a major consideration, resulting in some women with breast cancer opting against FP.11–15
Personal or peer experiences of infertility were also a factor.13,14 Having a previous history of infertility or unsuccessful infertility treatment discouraged women from pursuing FP. 13 The opinion of doctors,14,17 partners,14,17,18,20 and family members18,20 also played a key role in patients' FP decision.
Decisional conflict (uncertainty) and decisional regret
Four prospective studies looked at FP-related decisional conflict and regret experienced by women with cancer.22–25 The FP decision was considered difficult by almost two-thirds of women with breast cancer, 25 a majority experienced moderate–high levels of decisional conflict around this decision.22,23 Long-term satisfaction with FP decisions was associated with low levels of decisional regret, even in women who decided against FP, suggesting that improving the quality of decision-making could reduce regret. 24
Importance of information
Better fertility knowledge was strongly associated with reduced decisional conflict in breast cancer patients. 23 Furthermore, all 111 participants reported that receiving information regarding FP is important. 23
Five studies investigated the impact of fertility counseling, showing direct effects on decisional conflict and regret.22,26–29 Referral to a reproductive specialist and undergoing FP both reduced decisional regret and increased satisfaction. 29 Decisional conflict and regret were lower in those who received counseling from more than one health professional.22,29 Inadequate information and lack of counselor support increased decisional conflict. 28 FP counseling experiences differed across genders—men commonly recalled having fertility discussions, whereas women did not. 27 Furthermore, women experienced inadequate discussions and information provision, 27 resulting in pessimistic feelings about options. 26 Women dissatisfied with the quality of fertility-related information provided were less likely to pursue FP and have greater decisional regret post-treatment. 33
Three studies found that written and visual information, in the form of decision aids, reduced decisional conflict and regret in patients making FP decisions.30,31,34 They improved fertility-related knowledge, 30 aided information retention,30,31,34 and was almost as helpful as FP counseling. 34
As which patients will pursue FP cannot be predicted, FP discussions should occur with all patients of reproductive age. 32
Research in the pediatric and adolescent population
Two original research articles reported on decisions to cryopreserve sperm in adolescents,35,36 three original articles reported on decision-making regarding testicular tissue cryopreservation in the pediatric and adolescent population,37–39 and two were systematic reviews of FP decision-making in adolescents.40,41 See Table 2 for details.
Decision-making in established FP procedures (sperm banking)
Some parents expressed doubt over involving their adolescent son in the decision-making process (concerns about sexual immaturity, inappropriate timing), however, oncologists disagreed. 36 A quantitative study found that adolescents and their parents made decisions together and both believed banking sperm had been the correct decision, even if the sample was inadequate. 35
Decision-making in experimental FP procedures
When faced with a hypothetical choice between testicular biopsy and no FP, 77 adolescent cancer survivors regarded possible infertility as the most important factor in the “decision.” 38 In another study, where adolescents and children were offered testicular tissue cryopreservation (collected while under general anesthesia for another procedure), families who consented to the procedure believed they made the correct decision. 37 Parents who declined felt more overwhelmed and tended to weigh the risks more greatly. 37 Consenting parents' personal beliefs and opinions influenced their decision on pursuing or foregoing fertility procedures. They placed greater importance on preserving future fertility, having biological children, and were more likely to believe that stored tissue could be successfully utilized in the future. 37 They also had a greater desire to minimize future infertility-related mental and emotional burden. 37 The experimental nature of the procedure did not deter parents in either group. 37 Some families were willing to preserve fertility at additional risk, such as subjecting their child to an additional standalone tissue collection procedure and postponing the commencement of cancer treatment. 37
Adolescent involvement in the decision-making process
Over 90% of parents with a son over 12 years of age considered their child capable of participating in the decision-making process. 39 In the same study, 73% of adolescent boys felt the fertility information presented to them was clear, 80% felt it was complete, and 90.9% felt it was understandable. 39 Two reviews identified that adolescents felt inadequately informed by their healthcare professional about the impact of treatment on fertility and FP options available.40,41 Most desired FP discussions to occur early. 40 Receiving inadequate information may have prevented adolescents from contributing to the decision-making process. 41
Ethical considerations in the pediatric populations relating to FP decisions
Four articles in the pediatric literature addressed the ethical issues around FP, specifically around informed decision-making, the consenting process, and risks of recurrence.42–45
At a time of extreme vulnerability, parents are making decisions about experimental FP procedures that carry risks. 43 These include bleeding and pain from the invasive procedures and the retention of malignant cells in the collected tissue, which may cause relapse when retransplanted.44,45 The risk can be reduced, but relapse is a real possibility, and this fear can influence decisions.42,44 Parents need to make these decisions with limited time, knowing that not all children become infertile after cancer treatment.43,45
Parents may consent to FP, believing it is the only option for their child to have a “normal future.” 43 However, parental desires for future grandchildren and personal experiences around infertility may override what is best for the child and raise issues around decision-making. 43
Discussion
Clinical practice guidelines recommend that oncology patients are informed of cancer-related infertility and the FP options available.5,6 This then puts them in the difficult and complex situation of having to make an FP decision.11,13,14,22 Although underresearched in a pediatric population, in adults, this has been found to be a time of severe physical and emotional stress.11,14,22 Having to make a decision about FP with limited time, while still coming to terms with a potentially life-threatening diagnosis, can cause patients to feel overwhelmed.11,13–15 A poor quality fertility discussion and inadequate information provisions may compound the feeling of being overwhelmed and contribute to feelings of regret in the future.26–29 Appropriate fertility-related discussions combined with written and visual information in the form of decision aids can improve the patient's fertility-related knowledge, aid information retention, and lessen feelings of anxiety surrounding the decision, leading to reduced regret.23,30,31,34
The three pediatric studies identified in this review indicate that FP is important, and the experimental nature of procedures is not a deterrent.37–39 Unique ethical issues arise in FP decision-making in this population, which are not relevant in the adult population. First, parents are making a decision for their children; therefore, “adult” factors are likely to have a role, such as desires for biological children. 37 The experimental procedures have uncertain outcomes and may leave both parties experiencing negative feelings in the longer term. Despite its importance, very little data about reproductive decision-making are available in the pediatric population.
In the absence of literature, we may be able to draw on the FP decision-making experiences of adult and adolescent oncology patients. Similarities include that children are also likely to have concerns about fertility16,35,41 and the delay of cancer treatment for FP.12,14,29,35 Factors such as costs of FP procedures, medical and family members' opinions, and personal experiences of infertility are more likely to be factors important to parents. Some decision-makers would be willing to risk compromising cancer treatment to pursue FP, such is the importance of fertility to them.16,35,37
Key differences in the FP procedures offered to children and adults may impact the decision. In adults and male adolescents, the procedures available have proven efficacy and are less invasive. However, gonadal tissue cryopreservation in children is invasive, experimental, and carries a risk of reimplantation of cancerous cells. Although FP using established techniques may have positive outcomes and increase satisfaction in adults, 35 this may not translate to the experiences of young children. Furthermore, the overwhelming feeling commonly reported among adult cancer patients making FP decisions may be more extreme for parents, as there is no guarantee of success.13,14
The factors adult cancer patients take into consideration may be vastly different to those considered by parents, who face the challenge of not allowing personal needs, desires, and beliefs to influence the decision. For example, parent's opinion on the likelihood of scientific advancements in the FP field significantly influences their decision to consent to a procedure for their child, with parents who are hopeful of scientific advancements being willing for their child to go through a separate operative procedure and exposure to anesthesia solely for FP. 37 Parents, as surrogate decision-makers, may not be able to separate their own desires and beliefs from the decision-making process. Despite being unable to consent legally, children should still be involved in discussions, taking into consideration their level of emotional and mental maturity. 46 However, this can further complicate the situation if disagreement occurs between the child and parent, or between parents. 46 In addition, parents may feel that it is wrong to refuse FP, because they have declined the opportunity for their child to resume a “normal” life in adulthood. 46 They may blame themselves if their child becomes infertile due to the oncology treatment they had consented to. 46 Other concerns that may factor into decision-making include risk of cancer inheritance or disability in future offspring.18,47
Compared to adults, pediatric FP counseling does not appear to differ by gender, but instead by pubertal status and patient age. A survey of 24 pediatric oncologists in Australia and New Zealand found that, while 88% discussed the risks of infertility with patients older than 12 years, only 42% discussed it with patients younger than 12 years. 9 FP was discussed with all post-pubertal patients before oncology treatment. However, only 68% and 78% of pediatric oncologists discussed FP with prepubertal boys and girls, respectively. 9 Low discussion rates in prepubertal patients may be a reflection of discomfort in advocating for procedures with limited efficacy data. Lack of access to experimental procedures and the absence of centre-specific FP guidelines may also affect discussion rates. 9 Over 95% of pediatric oncologists felt it was necessary to establish institutional FP protocols, with oncology providers being more likely to engage in FP discussions where protocols were in place. 9 Due to lack of efficacy data, pediatric FP is only recommended where there is stringent ethical governance. 5
Decisional conflict and regret have been shown to be high in adult cancer populations, but may be addressed by having a fertility specialist consultation and improving FP knowledge.23,28–30 Thus, the provision of good quality information regarding risks to fertility and possible FP is also likely to be important to decision-makers.12,14,22,41 Adolescent patients have suggested that receiving information and support throughout the whole course of cancer therapy, and guidance as to how to involve their parents in the decision-making process, would help. 40 Clinicians should not censor fertility-related information to prevent any perceived additional psychological burdens. 23 Time and timing are also likely to be important. FP discussions can occur too soon or too late and decision-makers can feel that there is insufficient time to decide.11,13,35 Parents of children receiving oncology treatment may also benefit from counseling with pediatric gynecologists and endocrinologists, who have a thorough understanding of the complexities of pediatric FP.
The articles reviewed have limitations. Sample sizes were small and tended to consist of highly educated, white American women of a moderate to high socioeconomic background, thus limiting the generalizability of findings to the pediatric population.11–14,22 Further research is required to determine whether parents of children receiving potentially gonadotoxic cancer treatment are at risk of FP-related decisional conflict and regret both in the short and long term. More research into the factors that parents consider when making the decision is required. In addition, satisfaction of childhood cancer survivors, are (once they reach adulthood) with the decisions their parents made, needs further exploration. They may be at risk of decisional regret due to the same factors identified in the adult population, especially as they may not have been included in the decision-making process.
Conclusion
For prepubertal children, cryopreservation of gonadal tissue is the only FP option available. Unique ethical issues arise due to the experimental nature of the procedures, as well as the relationship between parent and child. Considering the decision to pursue FP is difficult in the adult population, decisional conflict and regret may be greater for parents who are making this decision for a child. If further research identifies high decisional conflict or regret in parents, clinical pathways may be altered to manage this. The manner of FP referral may be modified or a decision aid tool, which has been effective in adult populations in reducing decisional conflict and regret, may be developed to help parents.
Footnotes
Acknowledgments
Michelle Peate is supported by a National Breast Cancer Foundation Early Career Fellowship (ECF-15-005). Yasmin Jayasinghe is supported by an early career grant from the Victorian Cancer Agency. The authors thank Lynn Gillam for her support and assistance.
Author Disclosure Statement
No competing financial interests exist.