
Abstract
Uncertainty associated with cancer can foster future-focused worry and ultimately diminish physical well-being, especially among young adult survivors. Stress perceptions might exacerbate the association of worry and physical well-being. Young adults with testicular cancer (N = 171) completed measures of physical well-being, perceived stress, and future cancer-related worry. Perceived stress and future worry were both negatively associated with physical well-being. Perceived stress moderated the relationship; more perceived stress was related to lower physical well-being in those with high worry. Interventions aimed at worry reduction might benefit from reducing global stress perceptions.
Introduction
T
Experiences of worry after cancer can take a variety of forms but typically centers around uncertainty about the future and fears of a cancer recurrence. Young adults are often focused on the attainment of educational, vocational, and relationship goals. Future uncertainty can emerge when cancer threatens or delays these future plans and goals. Consequently, young adults report uncertainty as a major concern across the cancer trajectory.6,7 Related is the worry that cancer will return, progress, or spread to other organs.8,9 Elevated fear of recurrence among young men with TCa is common and exacerbated by mental distress, poor coping ability, and low self-esteem. 5
Given the global nature of stressors faced by young men with TCa, perceptions of stress play a central role in the extent to which worry about the future is associated with negative physical consequences. In fact, TCa survivors concomitantly report life stress concerns and fear of cancer recurrence, which are also associated with lower physical well-being. 10 The extent to which perceived stress and future worries act independently or co-occur to influence physical well-being is unknown. It is likely that perceived stress, or appraisals that current demands exceed coping abilities, 11 thwarts available coping resources and emotion regulatory efforts aimed at controlling worry about the future. Indeed, high levels of perceived stress are associated with greater use of negative coping strategies (e.g., denial). 12 Thus, diminished self-regulation in the presence of future worry could hinder functional ability for everyday activities. In contrast, individuals with lower perceived stress might have more available self-regulatory capacity and approach-oriented coping skills13,14 to buffer against the negative aspects of lower physical well-being (e.g., lack of energy and having trouble meeting the needs of one's family) when confronted with worry about the future.
No study has examined future worry in the context of perceived stress in young adults with TCa. To address this gap, this study examined relationships between future worry, perceived stress, and physical well-being in a sample of young adult men with TCa. We hypothesized that perceived stress and future worry will be negatively associated with physical well-being; we further hypothesized that perceived stress will moderate the relationship between future worry and physical well-being. Specifically, higher levels of perceived stress will be associated with lower physical well-being among those with relatively high future worry.
Methods
Participants and procedures
Participants were 171 English-speaking young adult (between 18 and 29 years of age) men with TCa identified by a state cancer registry and asked to participate in a study on “health-related quality of life after testicular cancer.” To focus on post-treatment experiences, young adults with a history of TCa, rather than during diagnosis or treatment, were eligible to participate. This reflects a 59% response rate of invited men. Responders did not differ significantly from nonresponders on clinical or demographic variables. Participants were on average 25.21 (SD = 3.33) years of age and 2.7 (SD = 1.61) years from diagnosis (Table 1). Participants completed questionnaires by mail or in person and were compensated $50. All participants provided informed consent and procedures were approved by the university institutional review board.
Measures
Cancer-related worry
Future worry during the past week was measured using the two-item future perspective subscale of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire for Testicular Cancer (EORTC QLQ-TC26) 15 (e.g., Do you feel uncertain about the future and Have you been anxious about possible recurrence of the disease?). Responses are on a four-point scale from (0) not at all to (3) very much. Scores were linearly transformed to a 100-point scale with scores ranging from 0 to 100. Higher scores represented higher levels of future worry. Cronbach's alpha was 0.71.
Perceived stress
Perceived stress during the past week was measured using the 10-item Perceived Stress Scale, 16 which was designed to measure how unpredictable, uncontrollable, and overloaded individuals find their lives (e.g., How often have you felt nervous and stressed and How often have you felt things were going your way?). Respondents were asked to rate their agreement with items on a five-point scale ranging from (0) never to (4) very often. A total score was calculated as sum of all items. Higher scores indicated higher perceived stress. Cronbach's alpha was 0.90.
Physical well-being
Physical well-being during the past week was measured using the seven-item physical well-being subscale of the Functional Assessment of Cancer Therapy-General (FACT-G). 17 The FACT-G is a validated and widely used measure within the cancer context and during the survivorship phase.18,19 Respondents were asked to rate their responses with items on a five-point scale ranging from (0) not at all to (4) very much. Sample items included “I have a lack of energy” and “I have pain.” A total score was calculated as a sum of all items. All items were recoded so that higher scores indicate higher physical well-being. Cronbach's alpha was 0.86.
Data analysis
Descriptive statistics and bivariate correlations were examined. Demographic (age, ethnicity, partner status, income, education, and employment) and medical variables (treatment type and time since diagnosis) significantly correlated with the dependent variable were used as covariates in subsequent hypothesis testing. Multiple linear regression was used to test hypotheses. In the model, relevant covariates were entered in the first block, perceived stress and future worry in the second block, and the interaction term (perceived stress X future worry) in the third block. To avoid multicollinearity, variables were centered around the mean, and interaction terms were computed and probed in accordance with methods outlined by Aiken and West. 20 Simple slopes for the association between future worry and physical well-being were tested at low (−1 SD lower than the mean), average (mean), and high (+1 SD higher than the mean) levels of perceived stress. 20
Results
Descriptive statistics and identification of covariates
The mean total score for perceived stress was 14.47 (SD = 8.21) and the total mean score for future worry was 40.14 (SD = 29.23). The mean score for physical well-being was 23.98 (SD = 4.77). Perceived stress was positively correlated with future worry (r = 0.58, p < 0.01), suggesting that higher perceived stress is associated with more worry about the future. Perceived stress (r = −0.57, p < 0.01) and future worry (r = −0.48, p < 0.01) were both negatively correlated with physical well-being, suggesting that higher amounts of perceived stress and worry about the future negatively impact physical well-being.
Bivariate correlations of demographic and medical variables were computed. Education (r = 0.35, p < 0.001), income (r = 0.28, p < 0.001), employment (r = −0.30, p < 0.001), history of diagnosed clinical depression (r = −0.28, p < 0.001), and history of a diagnosed anxiety disorder (r = −0.30, p < 0.001) were significantly associated with physical well-being and so were included as covariates in the subsequent model.
Hypothesis testing
Regression models revealed that higher levels of perceived stress (β = −0.36, p < 0.001) and future worry (β = −0.16, p < 0.05) were associated with lower physical well-being [F(8, 159) = 16.27, R2 = 0.44]. These main effects were qualified by a significant perceived stress X future worry interaction (β = −0.17, p < 0.01), which explained an additional 3% of the variance beyond the main effects (Table 2). Simple slope analyses revealed that for young adult men with high (β = −0.05, p < 0.001) or average (β = −0.03, p = 0.05) levels of perceived stress, high future worry was associated with lower physical well-being. The simple slope was nonsignificant at low levels of perceived stress (Fig. 1).
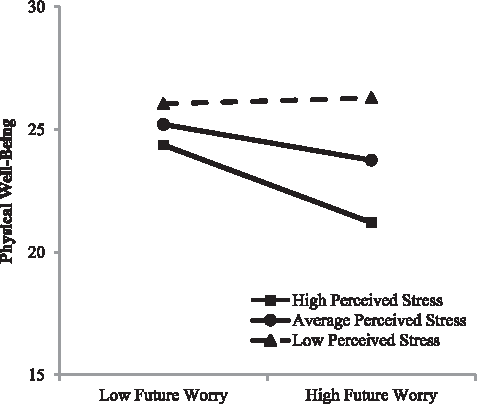
Perceived stress and future worry on indicators of physical well-being. Note: Simple slopes for the association between future worry and physical well-being were tested for low (−1 SD lower than the mean), average (mean), and high (+1 SD higher than the mean) levels of perceived stress. Dashed line indicates nonsignificant simple slopes.
Regression coefficients reflect values at the end of block 3, with all variables entered into the model.
p < 0.05; **p < 0.01; ***p < 0.001.
Hx, history; SE, standard error.
Discussion
This study revealed a negative association of future worry and perceived stress on physical well-being with support for the hypothesis that the context of stress exacerbates this relationship. Conceptual and empirical work on the regulation of repetitive thought processes, such as worry, suggests that worry requires self-regulatory effort and resources. 21 Thus, high levels of perceived stress might deplete critical coping resources necessary to regulate persistent worry in cancer groups. 22
As suggested by the nonsignificant simple slope, future worry was not related to physical well-being at low perceived stress. In fact, future worry exhibits increasingly stronger relationships with lower physical well-being as stress increases. These observations might reflect that more successful self-regulation is possible when perceived stress is low. Accordingly, sufficient coping resources may be more available at lower levels of perceived stress. It is possible that those with low perceived stress also experience less worry, as evidenced by higher physical well-being scores among those reporting low perceived stress and low future worry, than those reporting average or high perceived stress levels. In this study, worry and perceived stress were moderately correlated, suggesting they co-occur but are distinct psychological processes.
Future worry (M = 40.14, SD = 29.23) was lower than observations of other samples of TCa survivors, in which mean scores on the EORTC QLQ-TC26 future worry scale ranged from 48 to 59.3,15,23 However, these samples tended to be closer in time since active treatment, with some including patients engaged in active treatment at time of participation. Worry about the future likely declines for most patients over time. Notably, norms for the future worry subscale of the QLQ-TC26 are not yet available. 3
This study utilizes a diverse sample of young TCa survivors not well represented in health psychology research. However, some caution is needed in interpreting the current findings. These data were collected at a single point in time and so causal interpretations cannot be inferred. Although theoretically driven, our findings represent one set of possible relationships. It is also possible that physical health drives the psychological experience of worry and stress. Future studies should explore the longitudinal nature of the relationship between perceived stress, future worry, and physical well-being as it unfolds across time. The measures used in this study are self-reported, and although participants were reporting on recent experiences, recall bias could exist. Although our design allowed us to make observations among those in later survivorship phases when persistent problems may be more damaging, variability in time since treatment completion is notable. It is recommended that future research examines these relationships across the cancer trajectory. Finally, although no notable differences were detected between responders and nonresponders, it is possible that other biases related to selection exist.
These findings suggest that the high perceived stress presents a vulnerability that in combination with worry could present specific vulnerability to physical health. If so, future work should identify the mechanisms by which this unfolds to develop precise and targeted behavioral interventions. For instance, diminished self-regulation or impaired coping may be one possible pathway. This can be associated with patterns of emotional, physiological, and behavioral dysregulation that potentially has downstream physical health consequences. At present, few interventions have been developed or tested with young TCa survivors, yet this study highlights the need to identify patients at risk, reduce perceptions of stress, and control chronic worry. Other techniques to enhance self-regulation (e.g., emotion regulation, mindfulness, and behavioral activation) may also prove useful. More work that encompasses a multimethod approach by identifying biopsychological mechanisms of perceived stress and future worry is needed.
Footnotes
Acknowledgments
This work was supported by funds from the UCLA Cousins Center for Psychoneuroimmunology, the LIVESTRONG Foundation, and the National Cancer Institute (SC1CA187494).
Author Disclosure Statement
No competing financial interests exist.