
Abstract
Purpose:
Adolescent and young adult cancer (AYAC) survivors show an elevated risk of distress. Targeted psychosocial interventions for this distinct population are needed. This study examined the potential efficacy of a mindfulness-based intervention (MBI) to alleviate emotional distress and improve quality of life (QoL) in AYAC survivors.
Methods:
Participants were 16 AYAC survivors, aged 14–24, who had completed acute medical treatment. A two-baseline (8 and 1 week before the intervention), post- (1 week after the intervention) and 3 months follow-up within-subjects design was used. Each participant completed two baseline assessments, followed by an 8-week MBI. The primary outcome variables were emotional distress and QoL. Secondary outcomes were cognitive vulnerability factors and mindfulness skills.
Results:
Multilevel modeling showed (1) a significant reduction in emotional distress and improvement in QoL at 3 months of follow-up, (2) a significant reduction in negative attitudes toward self (i.e., a cognitive vulnerability factor), and (3) a significant improvement in mindfulness skills.
Conclusion:
MBI is a promising approach that is used to treat emotional distress and to improve QoL in AYAC survivors. Further research using randomized controlled trials is needed to generalize these findings. Trial registration information: www.trialregister.nl; NTR4358.
Introduction
M
Because of the multifaceted nature of the emotional distress involved, it is important to offer a transdiagnostic intervention. Transdiagnostic interventions target symptoms of stress, anxiety, and depression and aim at impacting common underlying vulnerability factors. 8 An example of interventions aimed at remediating the psychological vulnerability factors that contribute to emotional distress are mindfulness-based approaches. Mindfulness refers to a compassionate and non-judgmental moment-to-moment awareness of one's experiences. 9 Two common interventions to teach mindfulness skills are mindfulness-based stress reduction (MBSR) 10 and mindfulness-based cognitive therapy (MBCT). 11 Both programs follow a structured curriculum that is taught in a group format over 8 weeks. Participants develop specific skills in their capacity to become non-judgmentally aware of thoughts, feelings, and sensations, and they increase their capacity to replace automatic, habitual, and often judgmental reactions with more conscious and skillful responses. Alterations in negative thinking patterns such as rumination and worry, which are known cognitive vulnerability factors for depression and anxiety, are identified as potential mechanisms of change together with alterations in mindfulness and self-compassion.12,13
Over the past 25 years, mindfulness-based interventions (MBIs) have been found to reduce stress and symptoms of anxiety and depression in a wide variety of clinical and non-clinical populations,14–18 and there is supportive evidence of significant efficacy on alleviating symptoms of depression and anxiety and improving quality of life (QoL) in adult patients with cancer and survivors, with an overall moderate-to-large effect size.19–22 Randomized controlled trials investigated the efficacy and utility in managing persisting symptoms in adult cancer patients and survivors and found significant improvements in QoL, mood and well-being (breast cancer, age 55.5 ± 9.7), 23 levels of anxiety and depression (breast cancer, age 54 ± 10.3), 24 sleep disturbance (any type of cancer, age 51 ± 9.1), 25 fatigue (any type of cancer, age 53 ± 9.1), 26 and fear of cancer recurrence (breast cancer, age 57.5 ± 9.4). 27
Because of the empirically established benefits of MBIs among adult cancer survivors, the current study proposed to examine and establish the possible benefits of an MBI for AYAC survivors. To our knowledge, to date, only one study has examined whether an MBI has the same positive effects in AYAC survivors (aged 11–18 years) as in adult populations. 28 The authors assessed the feasibility and acceptability of an MBI by using a prospective quasi-experimental design with two groups (experimental versus no treatment). They found no significant differences in QoL, sleep, and mood between or within groups pre- to post-assessment and at follow-up. According to the authors, the validity of these results can be questioned because of the small sample size (n = 7 in each group), the absence of randomization, and the non-equivalence in showing interest in mindfulness of both the experimental and control groups. 28
More research is needed, and the aim of the current study was to investigate the potential benefits of an MBI for AYAC survivors of childhood and adolescent cancer. We focused on QoL and emotional distress as our primary outcomes. The inclusion of QoL endpoints has become an important outcome in oncology studies. This QoL includes not only the individual's physical well-being but also their mental well-being and role functioning. Our second primary outcome was emotional distress, which has a multi-faceted nature, including symptoms of depression, anxiety, and stress. We used a broad measure of emotional distress, taking into account the interplay of these different symptom clusters. We considered this emotional distress of equal importance as QoL.
We also explored potential mechanisms of change. We studied four cognitive vulnerability factors, being “cognitive reactivity,” “dampening of positive affect,” “negative attitudes toward self,” and “fear of cancer recurrence.” In addition, we measured “mindfulness skills” as a potential underlying mechanism. Cognitive reactivity refers to the reactivation of negative (often ruminative) thinking patterns when in a mild dysphoric state. 29 Previous research has shown that MBIs have a positive effect on cognitive reactivity.30–32 Dampening of positive affect is a cognitive response style that downgrades positive experiences. 33 Dampening thoughts focus, for example, on the negative aspects of positive experiences, and on the less fortunate aspects of life even when something positive comes along. 33 It is associated with elevated depressive symptoms in at-risk groups. 33 Negative attitudes toward self combines three potential self-regulatory vulnerabilities to depression: (1) holding overly high standards; (2) the tendency to be self-critical at any failure to perform well; and (3) the tendency to generalize from one specific negative experience or failure to a broader sense of self-focused worthlessness. 34 Such overgeneralization is a typical cognitive style in depression. 35 A previous study with adults has shown that MBI significantly reduced such overgeneralization. 31 Fear of cancer recurrence is viewed as a multidimensional phenomenon, including emotional components of anxiety and fear, and a cognitive dimension, including worry, preoccupation, and intrusive thoughts. 36 Research has shown that fear of cancer recurrence represents a risk factor for psychological distress, decreased QoL, and functional impairment. 37 In a study with adult breast cancer patients, fear of cancer recurrence was reduced after a 6 week MBI and mediated the effect on change in perceived stress and state anxiety. 38
We hypothesized that MBI would (1) improve QoL and reduce emotional distress (symptoms of depression, anxiety, and stress); (2) reduce underlying cognitive vulnerability factors; (3) and improve mindfulness.
Methods
Participants and recruitment
Between January 2014 and December 2015, recruitment was done via healthcare workers, posters and flyers, in four university hospitals in Flanders and via small advertisements in the local press. Inclusion criteria were (1) a histologically confirmed diagnosis of cancer; (2) primary treatment was stopped at least 1 month before enrollment in the study; (3) age between 14 and 24 years at the time of enrollment; (4) no evidence of an ongoing or lifetime severe mental illness (i.e., a clinically confirmed diagnosis, as defined by the Diagnostic and Statistical Manual of Mental Disorders—DSM 39 ), such as depression with suicide ideation, schizophrenia, psychosis, and personality disorders, which are not indicated with mindfulness interventions in general or with a short-term group intervention; and (5) proficiency in Dutch. No inclusion/exclusion criteria based on cancer type were set. AYACs willing to participate were invited to attend an information session, which was followed by an intake interview to determine their suitability for inclusion based on the eligibility criteria and their motivation and willingness to practice.
Due to the inability to know how many individuals received or read the study and because we are missing precise information on how many patients were invited to participate, it is not possible to calculate the response rate per se.
A total of 16 AYAC survivors volunteered to take part. Of the 16 individuals who participated, 10 were recruited by healthcare workers, 4 by advertisements in the local press, and 2 by the posters and flyers in the hospitals. All participants provided written informed assent and consent. Table 1 displays the baseline demographics and clinical characteristics of the participants.
SD, standard deviation.
Design and procedure
A two-baseline, post- and follow-up within-subjects design was used.i Participants completed four sets of self-administered questionnaires: at baseline (i.e., 8 weeks before the start of the MBI), pre-intervention (1 week before the start of the MBI), post-intervention (1 week after MBI), and follow-up (3 months after MBI). Participants received a festival ticket as incentive and were provided with compensation for their travel costs. The study was approved by the ethical committee of the four University Hospitals, with UZ/KU Leuven being the leading committee.
Measures
QoL and emotional distress
QoL was measured by using the total score on the Pediatric Quality of Life Inventory™ (PedsQL™ 4.0). 40 The adolescent and young adult self-report versions were used in this study.41,42 The 23-item PedsQL 4.0 Generic Core Scales encompasses four subscales: (1) physical functioning (eight items); (2) emotional functioning (five items); (3) social functioning (five items); and (4) school/work functioning (five items). Items are scored on a 5-point Likert scale and transformed into a 0–100 scale, with higher scores reflecting better QoL. The PedsQL 4.0 has good construct validity for measuring the QoL in AYAC survivors, 43 and good psychometric properties are reported for the Dutch version that was used in the present study. 42 The scale showed good internal consistency (α = 0.92) in our study sample.
Emotional distress was measured by using the total score of the Depression Anxiety Stress Scales (DASS-21).44,45 DASS-21 consists of 3 seven item scales measuring symptoms of depression, anxiety, and stress. Items are scored on a 4-point scale, where higher scores indicate higher levels of emotional distress. Good psychometric properties are reported for the original as well as the Dutch scale that was used in this study.45,46 The scale showed good internal consistency (α = 0.96) in our study sample.
Secondary outcomes
A short form of the revised Leiden Index of Depression Sensitivity (LEIDS-R) was used to assess cognitive reactivity.47,48 Participants are asked to report to what extent they displayed particular forms of thinking in response to low mood. The short form contains 17 items, which are scored on a 5-point Likert scale. Higher scores reflect higher levels of cognitive reactivity. The scale showed good internal consistency (α = 0.95) in our study sample.
The dampening subscale of the Responses to Positive Affect (RPA) questionnaire was used to measure the dampening of positive affect. 33 All seven items are scored on a 4-point Likert scale, with higher scores reflecting higher dampening of positive affect. Good psychometric properties are reported for the Dutch version that was used in the present study. 49 The scale showed good internal consistency (α = 0.90) in our study sample.
The total score of the Attitudes Toward Self Revised (ATS-R)50,51 was used to measure three cognitive tendencies that draw on a self-regulation model of behavior and are considered potential vulnerabilities to depression: holding overly high standards (three items), being self-critical in response to failure (three items), and generalizing from failure to the broader sense of self-worth (four items). All items are scored on a 5-point Likert scale. Higher scores indicate higher vulnerability. Good psychometric properties are reported for the Dutch version that was used in the present study. 51 The scale showed good internal consistency (α = 0.94) in our study sample.
Fear of cancer recurrence was assessed by using the Fear of Cancer Recurrence Inventory severity subscale (FCRI).52,53 This subscale consists of nine items and measures the presence and the severity of intrusive thoughts or images associated with fear of cancer recurrence. Items are scored on a 5-point scale. The item “How long have you been thinking about the possibility of cancer recurrence?” was dropped from the total score, since the end of acute medical treatment was less than 1 year for two participants. High scores reflect high fear of cancer recurrence. The scale showed good internal consistency (α = 0.93) in our study sample.
The Children's Acceptance and Mindfulness Measure (CAMM) was used as a mindfulness questionnaire.54,55 It assesses present-moment awareness and non-judgmental, non-avoidant responses to thoughts and feelings. The questionnaire consists of 10 items, scored on a 5-point Likert scale. Scores are reversed, and items are summed. Higher scores correspond to higher levels of mindfulness. Previous studies have demonstrated the CAMM to have good reliability and validity. 55 The scale showed good internal consistency (α = 0.90) in our study sample.
We also measured the level of engagement with homework. During post-treatment and follow-up assessment, participants could indicate with a number from 0 to 6 whether they did not practice (0), practiced less than once a month (1), practiced once a month (2), more than once a month but not on a weekly basis (3), once a week (4), more than once a week but not on a daily basis (5), and daily (6).
Intervention
The MBI program adhered to a standardized protocol developed from the MBSR 10 and MBCT manuals.11,56 The program was adjusted for adolescents and consists of eight 90-minute sessions that were held once a week for 8 consecutive weeks. During each session, guided experiential mindfulness exercises were taught (e.g., focus on the breath, body scan, breathing space, mindful yoga, insight meditation, walk meditation), combined with psycho-education (e.g., stress, depression, fear of cancer recurrence, self-care). Participants shared experiences of the exercises and reflected in small groups. Before the closing mindfulness practice, a review of home practices was carried out. The program is aimed at: (1) increasing present moment awareness and recognizing entanglement with one's thoughts and emotions; (2) teaching acceptance and mindfulness as an alternative strategy for dealing with problematic thoughts and feelings, and how these may be used to facilitate values-based actions. A brief overview of the session content is given in Table 2. The most important differences compared with the MBSR/MBCT manuals are: (1) formal exercises were shorter (e.g., bodyscan of 20 minutes instead of 40 minutes) and more repetitious—this is because it is more challenging for adolescents to focus attention on a single activity for longer periods of time; (2) a great deal of attention was given to informal exercises, adolescents are more likely to be engaged in frequent informal exercises throughout the day, as they incorporate these exercises in many of their daily activities (e.g., mindful listening to music); and (3) the psycho-education part was adapted to the world and language of adolescents. The training was supported by the use of homework assignments and audio material. Daily home practice was strongly encouraged.
Study participants could bring a friend, brother, or sister who also could attend the MBI. Accompanying people were not part of the study and did not complete questionnaires. During the study period, six groups of three to six participants (including the accompanying persons) were run. The sessions took place outside the hospital in a mental health center or in a monastery. The program was provided by a clinical psychologist who received extensive training in MBCT and was a certified trainer. Sessions were videotaped and reviewed for the validity of the intervention by an expert MBSR clinical psychologist, who confirmed that all curriculum objectives were met.
Data analyses
The intervention effect was tested by using a multilevel model. We used a piecewise model, in which change is described by using a discontinuous trajectory with separate slopes through two distinct phases of time. End of baseline (T2) was identified as the breakpoint to distinguish change before and after T2.
We first ran direct slope models to test whether there was a significant linear change on average before (Tslope1) and after (Tslope2) end of baseline. This was done for all outcomes. The model was specified as:
where Yij represents the outcome of the j-th participant at the i-th assessment time. The residual was represented by rij. The intercept (β0j), slope1 (β1j, before end of baseline; Tslope1 coded as −1 0 0 0), and slope2 (β2j, after end of baseline; Tslope2 coded as 0 0 1 2) were allowed to vary randomly across people. A Bonferroni correction for multiple comparisons was used (critical alpha = 0.0036).
Second, we used an alternative specification of the piecewise model, the slope and deviation slope model, to determine the difference between the linear rates of change before and after end of baseline. In this model, a single continuous linear slope is specified during the entire study period (via the time predictor −1 0 1 2) and a second piecewise slope is specified that turns on after end of baseline (coded as 0 0 1 2). In this case, the fixed effect of slope2 is the unique effect of treatment after controlling for the effect of time. The “lme4” package 57 in R, R Development Core 58 was used for the multilevel analysis.
Within-group effect sizes are calculated by using Hedges's gav, which incorporates the correlation between measurements and provides a more accurate estimate in small samples. 59 We also calculated the common language effect size, which gives an accurate description of the likelihood in correlated samples where measurements are paired. 59
Results
Preliminary analyses
A CONSORT flow diagram on enrollment of participants in the study is given in Figure 1. Of the 16 individuals who participated in the MBI, 2 dropped out and could not complete the training program due to illness. Both were men, aged 20 and 24, with diagnosis of aplastic anemia and brain tumor, and they both followed individual psychotherapy. They did not differ in any of the baseline characteristics from the other participants. For the 14 participants who completed all assessments, the median number of treatment sessions attended was 8 (range: 6–8). Correlations among variables at the start of baseline are given in Table 3. Fear of cancer recurrence was negatively associated with overall QoL. Emotional distress was positively associated with cognitive reactivity, dampening of positive affect, and negative attitudes toward self. Mindfulness skills were negatively associated with emotional distress and dampening of positive affect. Dampening of positive affect was also positively correlated with cognitive reactivity. Table 4 presents the detailed descriptive statistics of the outcomes at the four study data collection points. Figures 2 and 3 show the change in mean values of the primary and secondary outcomes, respectively.
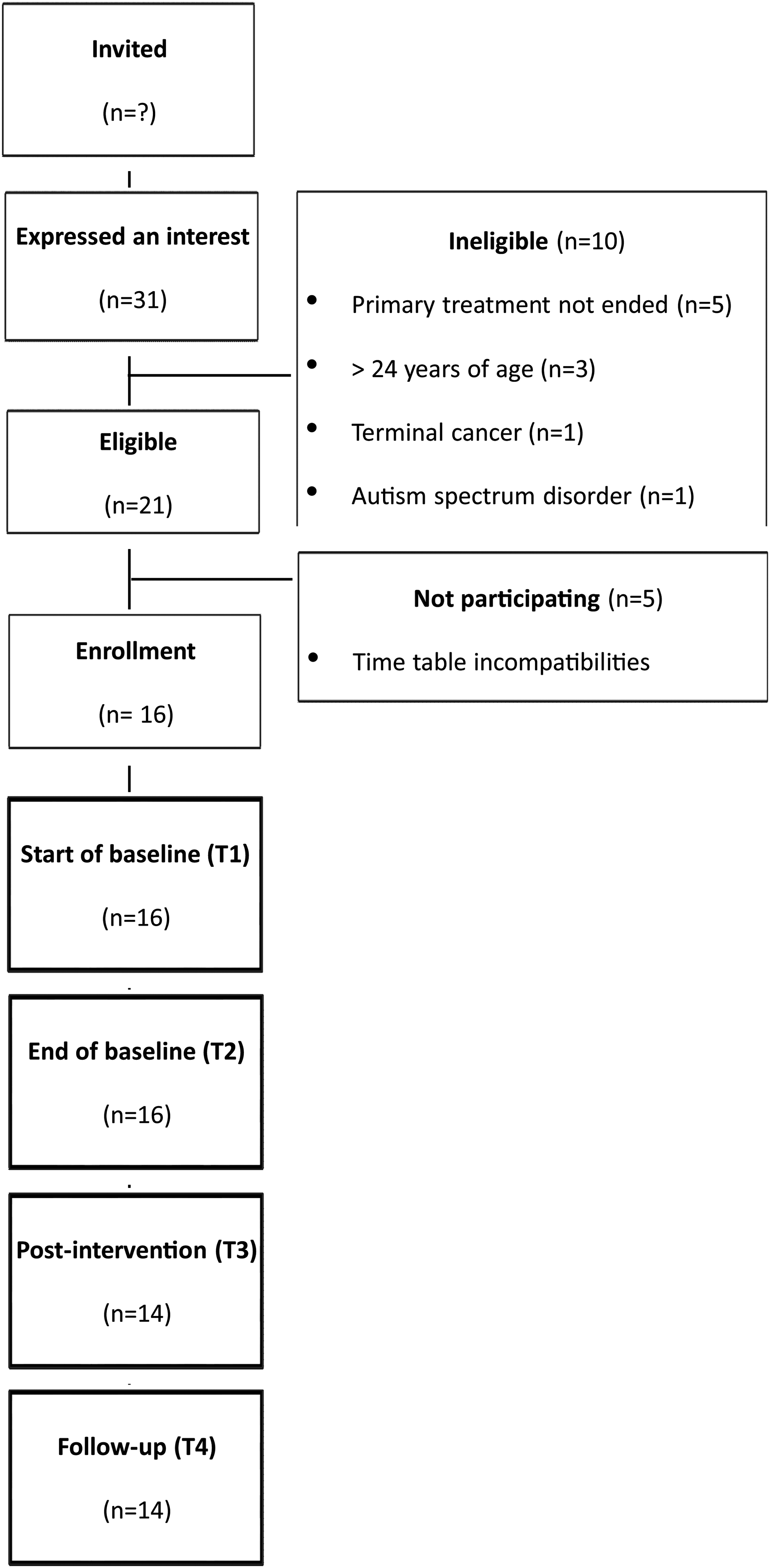
CONSORT flow diagram on enrollment of participants into the study.
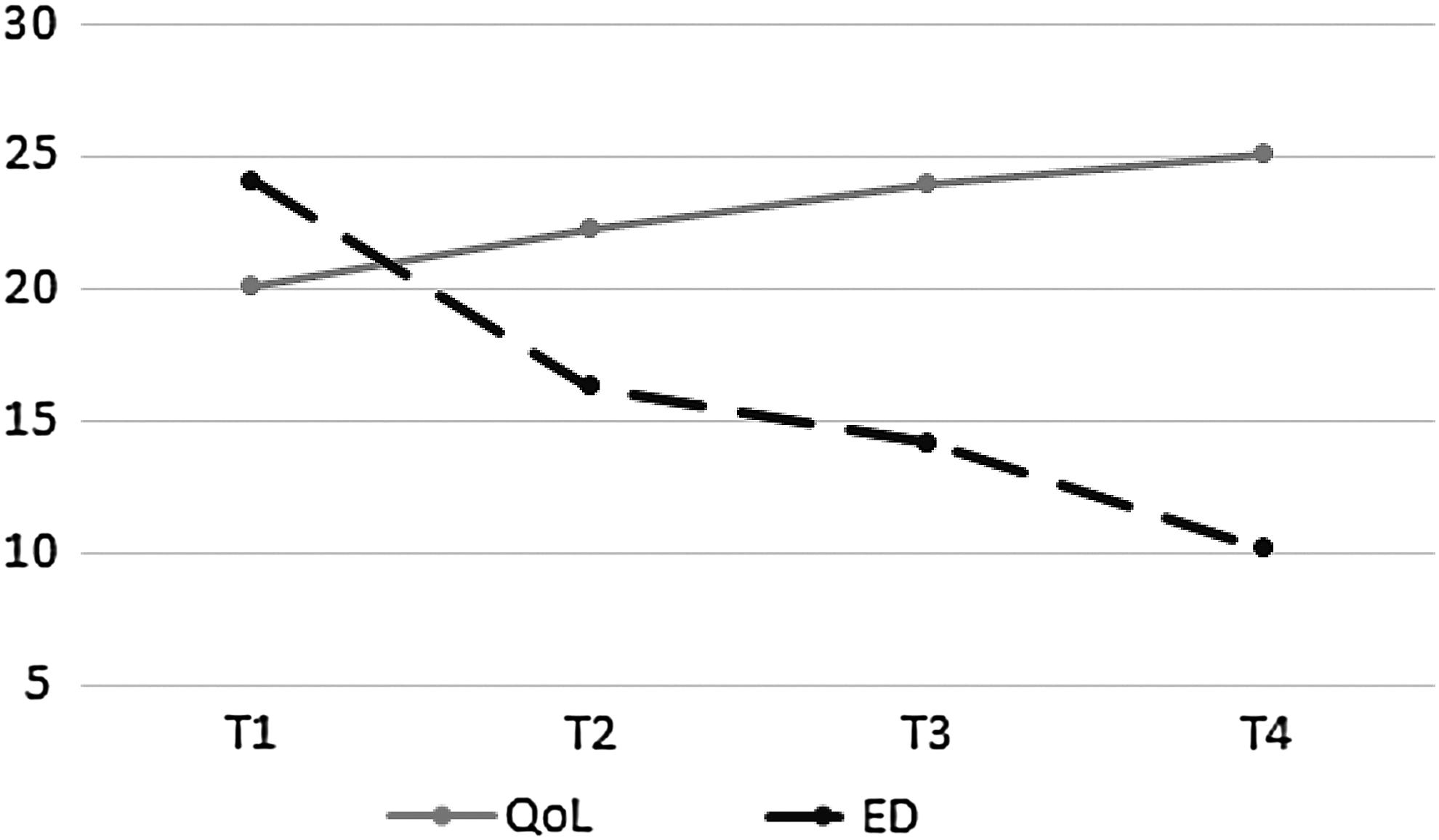
Change in mean scores of overall QoL and ED over T1 (start of baseline), T2 (end of baseline), T3 (post-intervention), and T4 (follow-up). Scores of QoL divided by 3 to fit scale. ED, emotional distress; QoL, quality of life.

Change in mean scores of the cognitive vulnerability factors and mindfulness skills over T1 (start of baseline), T2 (end of baseline), T3 (post-intervention), and T4 (follow-up). Scores of FCR and dampening plus 10 to fit scale; scores of ATS minus 10 to fit scale. ATS, attitudes toward self; FCR, fear of cancer recurrence; MFS, mindfulness.
p < 0.05, **p < 0.01.
QoL, quality of life; ED, emotional distress; CR, cognitive reactivity; Dampening, dampening of positive affect; FCR, fear of cancer recurrence; ATS, attitudes toward self; MFS, mindfulness.
CL, common language effect size.
Multilevel analyses
Is there a significant change before and/or after end of baseline?
The fixed effects of the direct slope models (Table 5) for overall QoL indicated that there was a significant improvement during baseline (slope T1-T2: B = 5.94, p = 0.04) and after the intervention (slopeT2-T4: B = 4.71, p = 0.002). Emotional distress significantly reduced during baseline (slope T1-T2: B = −7.15, p = 0.006) and after the intervention (slope T2-T4: B = −3.31, p < 0.001). After Bonferonni correction, the change in QoL and emotional distress was only significant after the intervention.
The coefficient of slope T2-T4 indicates the rate of change per time interval.
p < 0.05, **p < 0.01, ***p < 0.001; Significance level after Bonferonni correction p < 0.0036.
A significant change in the cognitive vulnerability factors dampening (B = −1.52, p = 0.007), and attitudes toward self (B = −3.54, p < 0.001) could be observed only after the intervention (slope T2-T4). Cognitive reactivity significantly reduced during baseline (slope T1-T2: B = −3.69, p = 0.04) and after the intervention (slope T2-T4: B = −3.51, p = 0.01). No significant change in fear of cancer recurrence could be observed. A significant change in mindfulness skills (slope T2-T4: B = 3.29, p < 0.001) was observed only after the intervention. Only the change in attitudes toward self and mindfulness skills after the intervention remains significant after Bonferonni correction.
Is this change observed after the intervention still significant after controlling for the effect of time?
The slope and deviation slope model showed a significant unique effect for attitudes toward self (B = −3.21, p = 0.023) and mindfulness skills (B = 3.15, p = 0.041).
Effect sizes
Start of baseline to end of baseline effect sizes (Table 4) were medium (0.51–0.71) and statistically meaningful for overall QoL, emotional distress, and the vulnerability factor cognitive reactivity. Controlling for individual differences, the likelihood that participants improved on overall QoL during the baseline period was 78%, and the likelihood that emotional distress and cognitive reactivity decreased was 80% and 83%, respectively.
End of baseline to post-intervention effect sizes were medium and statistically meaningful for overall QoL (0.53), and dampening of positive affect (0.58), and large (0.89) for attitudes toward self. Controlling for individual differences, the likelihood that participants improved on overall QoL was 72%, the likelihood that dampening of positive affect decreased was 75%, and the likelihood of attitudes toward self-improved was 95%.
End of baseline to 3-month follow-up effect sizes were medium (0.63–0.75) for overall QoL, cognitive reactivity, and dampening, and large (0.86–1.14) for emotional distress, attitudes toward self, and mindfulness skills. Controlling for individual differences, the likelihood that participants improved on overall QoL and emotional distress was 81% and 87%, respectively, the likelihood that cognitive reactivity and dampening of positive affect decreased was 77%, and the likelihood that attitudes toward self and mindfulness skills improved was 87% and 90%, respectively. No statistically meaningful effect sizes were found for fear of cancer recurrence.
Engagement with homework
The level of engagement with homework ranged from 3 to 6 at post-treatment (mean = 4.71, standard deviation [SD] = 0.55) and from 2 to 5 at follow-up (mean = 3.29, SD = 0.80). These measurements had no impact on the outcomes.
Discussion
A statistically significant improvement in overall QoL and a significant reduction in emotional distress were found from end of baseline to follow-up. Effects were the most obvious at 3-month follow-up, with a medium (0.75 for QoL) to large effect size (0.86 for emotional distress). Although these findings are in line with previous studies on the effects of MBIs for adult cancer patients and survivors,20,21 we have to interpret them with caution due to the small self-selected sample and the lack of a control group.
Participants also showed an improvement in overall QoL and a reduction in emotional distress between the two baseline assessments. This might be seen as a kind of placebo effect related to the expectancy of receiving training and/or a simple effect of the mere passage of time. Although these observed changes were not significant, they may explain the fact that we did not find a significant effect on QoL or emotional distress after controlling for time. It is known that being on a wait-list for treatment has a “holding” positive influence, decreasing the apparent effects of the intervention. 22
We also found a significant decrease in negative attitudes toward self and a significant increase in mindfulness skills even after controlling for time. The other cognitive vulnerabilities, cognitive reactivity and dampening of positive affect, were successfully modified in the expected direction after the intervention but not significant (Fig. 3). These positive effects are again the most obvious at 3-month follow-up, with a medium (0.63 for cognitive reactivity and 0.71 for dampening) to large effect size (0.90 for attitudes toward self and 1.14 for mindfulness skills). No differences in participants' scores for dampening, attitudes toward self, and mindfulness were found between the two baseline assessments, which increases confidence that the improvements we observed after intervention are related to the intervention rather than being a function of the assessment and/or passage of time. The positive effect on cognitive vulnerability processes (i.e., thinking patterns that predispose an individual to emotional problems) corresponds with earlier findings.31,60 Especially the significant changes in attitudes toward self and mindfulness are important findings, as both can be seen as core processes of MBIs.13,61
We could not find a significant change in fear of cancer recurrence nor could we detect a significant meaningful effect size. Studies by Lengacher et al. showed significant reductions in fear of recurrence in two randomized controlled trials with breast cancer patients (n = 82 and 84) while evaluating a 6-week MBSR program.27,38 We consider two possible explanations for the absence of a clear effect in our study. First, fear of cancer recurrence can be seen as a normal reaction to the cancer experience and did not reach a problematic or pathological level in our study population. The mean score at follow-up in our study sample was 15, which is comparable with scores measured in adult patients who survived different types of cancer 62 and lower than clinical scores (19.7) as measured in a population of adult cancer survivors.37,63 However, to date, there is a lack of consensus on the definition and characteristics of fear of cancer recurrence when it reaches a clinical level. 63 Second, we used a short version of the questionnaire only measuring the severity, which represents fear the most appropriately. 64 Therefore, a comparison with the studies by Lengacher et al.,27,38 who measured fear of cancer recurrence as a multidimensional construct, can be different due to another measurement approach.
In addition, our results show that MBI is feasible for AYAC survivors. We had a very low treatment dropout (only 12%), which was due to illness. For most of the participants, mindfulness was new and some participants mentioned that they did not know what to expect. Every participant had positive comments about the program and described it as helpful. Although several participants enjoyed some types of mindfulness exercises more than others, all participants found at least one type of exercise that they enjoyed and practiced each week. They were also pleased that MBI was different from support groups in that information, experiences, and advice regarding cancer are not provided per se. Some participants also expressed a desire to continue meeting as a group and to still maintain contact via Facebook. This finding is consistent with other studies of MBIs in adolescents. 65 A recent review of mindfulness-based approaches for children and youth found that studies investigating feasibility and acceptability of mindfulness interventions adapted for youth show that interventions are well tolerated, acceptable, and feasible, with no adverse effects reported in clinical and non-clinical populations. 66
Although this was a multi-site trial using a mixture of recruitment strategies (cancer registries from the hospitals, posters and brochures to announce the study, advertisements in newspapers, on social media and websites, incentives), we still experienced large difficulties recruiting participants. The specific difficulties we encountered in this study were mainly due to time-table incompatibilities and stigma. Most AYACs have a very busy life and are very active, and a commitment to follow 8 weekly sessions was a reason for non-participation. Therefore, the arrangement of 8 weekly sessions might need to be revised for the future. An alternative suggested strategy is the use of blended care with, for instance, only four group sessions and in-between online support to continue with practicing the exercises. This combination can become increasingly useful, as adolescents have been described as very open and responsive to the use of multimedia in receiving therapy. 6 Stigma is still one of the most common and major problems for the recruitment in this kind of trials. 67 Low-threshold interventions delivered outside a clinical setting may be a solution to this problem. There is also preliminary evidence that the broad social scope of MBIs may provide support for those who are more vulnerable in our society, such as ethnic minority groups 68 and people with a low socioeconomic status. 31
This study has several limitations. First, it was not a randomized controlled trial, participants were self-selected, and the sample size was small. In addition, because of the lack of an active control group, we cannot rule out that unspecific effects such as social support may explain a significant proportion of our results. It would also be useful to assess participants over a longer period of time to discover whether the benefits are maintained. Also, we only used self-report measures. Future studies should also look at biological and bio-behavioral parameters of stress reactivity and/or resilience, as these data might be particularly useful in understanding the onset and course of mental problems. No formal evaluation on feasibility and acceptability was conducted. Despite these limitations, this study contributes to the existing literature on psychological interventions for AYAC survivors by demonstrating the potential promise of MBIs for this target group.
Conclusion
This study provides potential promise of MBI in improving overall QoL and alleviating emotional distress in AYAC survivors. Changes in symptoms scores were associated with changes in cognitive vulnerability factors and mindfulness skills. Findings must be interpreted cautiously while considering our small sample size, the self-selection to participate, and the lack of a comparison group. Further research is needed to validate these preliminary results.
Footnotes
Acknowledgments
This research was supported by a grant from “Anticancerfund” www.anticancerfund.org and “Alexine Clarysse Fonds” ![]() . The writing of this article has been facilitated by KU Leuven Center for Excellence on Generalization Research (GRIP*TT; PF/10/005) and by KU Leuven Research Council grant GOA/15/003. Inge De Leeuw and Katharina Müllen adapted the MBI, with the assistance of Edel Maex and Jen Bertels. Inge De Leeuw delivered the intervention, with the assistance of Francisco Gazquez and Ineke Van Mulders. Jen Bertels did the supervision. The authors acknowledge the researchers who provided them with the questionnaires used in this study. The QoL study described in this article was carried out by using PedsQL, developed by Dr. James W. Varni. Fear of Cancer Recurrence was measured by using the Fear of Cancer Recurrence Inventory, developed by Dr. Sebastien Simard. The Dutch translation was provided by Dr. Marije van der Lee. The authors thank the personnel of the Oncology Departments at the four University Hospitals (UZ Leuven, Gent, Antwerp, and Brussels) who helped with the recruitment and sincerely thank all participants in this study. Special thanks go to Klara Rombauts, Lydie Meheus, and Benoit and Véronique Clarysse for their sincere and motivating interest.
. The writing of this article has been facilitated by KU Leuven Center for Excellence on Generalization Research (GRIP*TT; PF/10/005) and by KU Leuven Research Council grant GOA/15/003. Inge De Leeuw and Katharina Müllen adapted the MBI, with the assistance of Edel Maex and Jen Bertels. Inge De Leeuw delivered the intervention, with the assistance of Francisco Gazquez and Ineke Van Mulders. Jen Bertels did the supervision. The authors acknowledge the researchers who provided them with the questionnaires used in this study. The QoL study described in this article was carried out by using PedsQL, developed by Dr. James W. Varni. Fear of Cancer Recurrence was measured by using the Fear of Cancer Recurrence Inventory, developed by Dr. Sebastien Simard. The Dutch translation was provided by Dr. Marije van der Lee. The authors thank the personnel of the Oncology Departments at the four University Hospitals (UZ Leuven, Gent, Antwerp, and Brussels) who helped with the recruitment and sincerely thank all participants in this study. Special thanks go to Klara Rombauts, Lydie Meheus, and Benoit and Véronique Clarysse for their sincere and motivating interest.
Author Disclosure Statement
No competing financial interests exist.