
Abstract
Purpose:
The Fertility Attitudes and Cancer Treatment Study (FACTS) aims at better understanding the reasons and priorities of young adult cancer patients making decisions for fertility preservation (FP). Identifying the factors that center around a patient's fertility decisions will support the development of educational tools for providers and improve clinical care to meet patients' reproductive needs.
Methods:
An exploratory qualitative study was conducted of 27 newly diagnosed male and female cancer patients who had presented for an oncofertility consultation. Interviews lasted ∼30 minutes and were transcribed verbatim. A thematic analysis was conducted to explore the factors driving decisions for future fertility. Themes were grouped to address the following topics: reasons for/against FP, patient priorities, informational needs, support, wellness, and satisfaction with information. Strength of the theme was determined by examining the frequency of a response.
Results:
Patients who chose FP versus those who did not choose FP and men versus women proved to be more similar than different in their reasoning, priorities, and informational needs for FP decisions. Patients who chose FP identified a “concern for future fertility” as a top reason to do so and “parenthood” as a top priority. For those who did not choose FP, “cancer treatment” was identified as their top priority. For patients identifying financial barriers, 50% of them were able to overcome this to pursue FP.
Conclusions:
Reproductive-aged patients diagnosed with a new cancer should be referred to a reproductive specialist and provided the opportunity to come to a fertility decision on their own before initiating cancer treatment.
Introduction
W
For the majority of AYAs undergoing cancer treatment, traditional chemotherapy and radiation therapy can have irreversible effects on their fertility.3–6 Survivors have reported this loss of fertility as a devastating psychosocial effect and a decrease in their quality of life, suggesting a critical need for providing effective fertility preservation (FP) services to cancer patients.7–9 Patients of reproductive age have to now consider their priorities surrounding future parenthood. 10
In nearly 70% of young adults, the diagnosis of cancer does not change the desire for children; however, FP is often overlooked in a patient's clinical care.3,11 Survivor studies have identified the challenges that young adults experience with receiving adequate fertility information at the time of diagnosis: the urgency to start treatment, inadequate fertility information, and socio-demographic influences contribute to patients' access to FP services.12–24
Limited research has been conducted on patients at the time of diagnosis to explore how they make their future fertility decisions. The research on decision making thus far has been examined retrospectively and focused on the patients' experience with getting information and not on how patients prioritize factors contributing to their FP decisions.25–28 These studies support the need for services for AYA patients to receive fertility information or else risk these, losing their opportunity to be parents.
The Fertility Attitudes and Cancer Treatment Study (FACTS) is a two-phase study with the goal of improving our understanding of the complex factors that are involved with patients' decisions regarding future fertility. Phase 1 examined FP utilization rates and characteristics associated with FP decisions among a cohort of oncofertility patients. In phase 2, we conducted a qualitative study to better understand patients' reasons for choosing FP and to identify their priorities at the time of their diagnosis. As demonstrated in earlier studies, patients are often asked to make decisions about their fertility, with limited information about reproductive risks. Patients are left with making uninformed decisions about their future fertility.29,30 The following study examined how AYAs come to their fertility decisions only after receiving a fertility consultation.
The overall goal of this study was to understand the priorities and decision-making needs for newly diagnosed AYA cancer patients by exploring why some patients elect FP and others do not. To better understand the low utilization of FP, particularly among women, we compared men and women to note differences in priorities and reasons. Identifying the factors that center around patients' fertility decisions will support education for providers and improve clinical care to meet patients' reproductive needs.
Methods
Study design
The two-phase FACTS study incorporated a sequential explanatory mixed-method design. The results of the quantitative phase drove the topics analyzed in the second phase. In phase two, an exploratory qualitative study was conducted by using the principles of critical theory to explore the patient factors driving decisions for future fertility. The critical theory methodology explores explanations, or theories, of a group and examines differences between groups. Often, analysis is directed by existing theories about the population.31,32
Patients participated in a 30-minute semi-structured interview within 30 days following their fertility consultation. The interview script was developed by using premises from the literature, phase 1, and an initial pilot study to gather information on factors affecting FP decisions before cancer treatment (Supplementary Figure S1; Supplementary Data are available online at www.liebertpub.com/jayao). Interviews were audio-recorded and then transcribed verbatim. The transcripts were immediately coded by using Atlas.ti 7.0 to determine whether saturation had been reached. Approximately one-half of the interviews (14/27) were independently coded by two coders for internal reliability; the primary author coded the remaining interviews. The inter-coder reliability rate was 94.5%, with all disagreements being decided by the primary author. Two patients changed their FP decision after the interview and were analyzed per their final decision.
Recruitment
Recruitment was conducted at two reproductive medicine clinics in Denver, Colorado, from April 24, 2014 through July 9, 2015. All newly diagnosed cancer patients 18–45 years of age who received a fertility consultation by a study-trained reproductive specialist were eligible for recruitment. Those with a relapse, secondary diagnosis, in remission, initiated treatment, without testes or ovaries, pregnant at the time of diagnosis, or unable to conduct the interview in English were not eligible. There were no exclusions based on cancer diagnosis or stage. The Colorado Multiple Institution Review Board (COMIRB) approved the study for conduct.
The fertility consultation provided information to patients, including: their risk profile for fertility loss, FP options, baseline fertility assessments, options for nongenetic children, and risks of FP treatment. In most cases, patients had <72 hours to make a FP decision.
Analysis
Demographic data were analyzed by using Fisher's exact statistic for categorical variables and t-tests for continuous variables to determine whether the decision groups (yes FP and no FP) were characteristically different. The interview transcripts were synthesized by using a content analysis approach, specifically a summative thematic analysis (Fig. 1).33,34 Summative analysis allowed for the quantification of codes to explore the frequency of themes. Themes mentioned with a greater frequency were inferred to have higher priority among the study population. 34
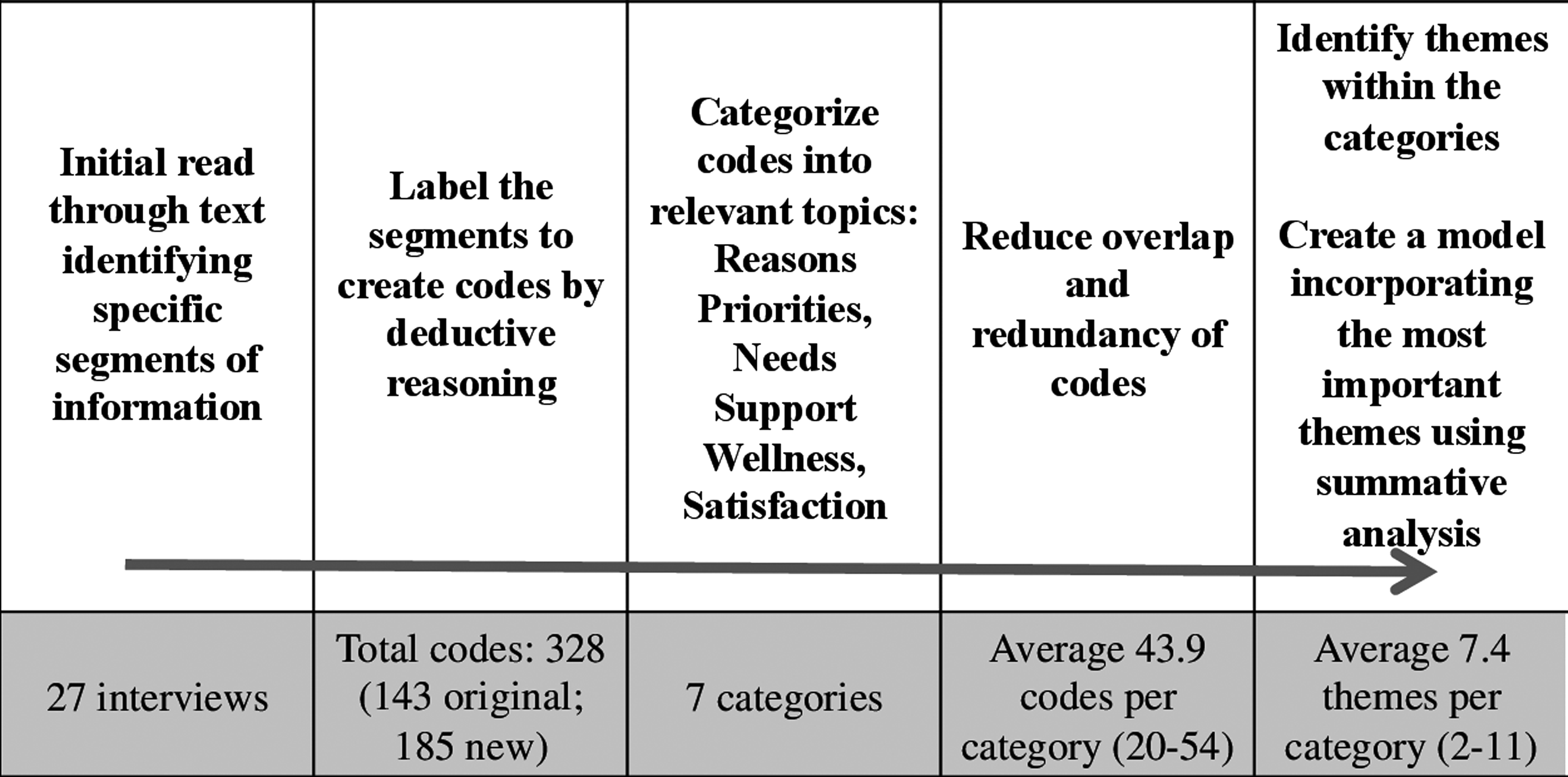
Synthesis of qualitative data: a framework for the synthesis of the qualitative data based on critical theory.
The initial topic areas and 143 codes were created based on findings from a literature review and the quantitative study.35,36 An additional 185 new codes were derived for a total of 328 codes. Codes were grouped deductively into themes emerging from the data. Themes were grouped to address the following topics: reasons for/against FP, patients' priorities, and informational needs. Themes were ranked based on how frequent a theme was reported.
Results
Study population
Thirty-one patients were approached for inclusion; 27 (87%) consented to participate in the study. The average age of participants was 30.3 (19–41) years old. Overall, 56% (15/27) of participants chose FP (sperm or embryo/egg cryopreservation) and 56% (15/27) were women. Among men, 67% (8/12) chose FP whereas 45% (7/15) of women chose FP. None of the demographic characteristics were significantly associated with FP decision (Table 1).
Blood: AML, CML, polycythemia vera; solid tumor: breast, colon, endometrial, ewing Sarcoma, non-Hodgkin's lymphoma, lymphomas, renal cell, synovial sarcoma, testicular; skin: melanoma.
FP, fertility preservation.
Reasons for FP
Respondents were asked about their reasons for considering FP, and eight themes emerged (Fig. 2). The reasons to choose FP did not differ between the decision groups (yes FP, no FP) or gender groups (men, women). All groups ranked “concern about their fertility risks” as the top reported theme. This included patients' concern about their current reproductive health status and for conceiving after undergoing cancer treatment. Participants discussed concerns that their fertility status would be irreversible after cancer, FP assured a chance for fertility, their fertility risk was unknown, and securing their future fertility as a priority. Fertility concerns were mentioned on average 5.4 times per patient among those who chose FP and 1.3 times per patient for those who did not choose FP.

Ranking of patients' reasons for and against considering FP; a side-by-side comparison. (N = 27). FP, fertility preservation.
When looking at gender, men mentioned this concern 51% of the time when discussing reasons to consider FP, whereas women provided it 37% of the time. A female patient opting for FP said: “From what we heard from our doctors, there is not a great chance that there will really be any fertility left after my treatment. So I feel like [egg banking] is our only one option.”
The second most frequently mentioned theme for choosing FP was patients' “access to FP information and services.” Participants mentioned education, feeling informed, accessibility of FP services, and provider referral when discussing FP information and services influencing their decision. This was similarly ranked second for all groups (yes/no FP, men/women).
A man who elected FP noted: “It was something that once I read there was a chance for infertility, [sperm banking] was something that I wanted to do. The doctors were good at giving me the information very quickly and very easy for me to understand.” Participants also mentioned a fear of future regret, social pressures, financial support, knowledge of assisted reproductive technologies, survivorship quality of life, and cultural beliefs as reasons to consider FP. These themes occurred less than one time per patient.
Reasons against FP
Respondents were asked about their reasons for not considering FP, and eight themes emerged (Fig. 2). The groups did differ in their reasons for not considering FP. For those who underwent FP treatment, “financial concerns” was reported most frequently (43% of the time) as a reason to not consider FP. Financial concerns included: financial support, the cost of FP, cancer treatment costs, cost of raising a child, insurance coverage, and borrowing money. A woman who ultimately elected FP stated: “None of the parts [FP procedure] that we have done right now have been covered by insurance. So that is definitely a con and I think that is the biggest negative aspect.” Despite being the top reason to not consider FP, these patients ultimately overcame the financial obstacle to undergo FP. Interestingly, “financial concerns” was the fourth ranked reason given by those who did not elect FP.
For AYAs who did not elect FP, “concerns about fertility risks” was the top reason given. Participants reported being concerned about the FP procedures and medications, birth defects for future children, their reproductive health being hindered by their diagnosis, poor fertility assessments, their age, passing along a cancer gene, having a low or unknown risk for fertility loss, and conceiving on their own after cancer among their concerns for not electing FP.
Men and women did not differ in their reasons against FP. “Concerns about fertility risks” was reported as the top ranked reason for not choosing FP for both genders, followed by “financial concerns.” For 50% of the patients with financial concerns, this barrier was overcome. This was similar in both men and women.
Patients' priorities and concerns
Participants were asked to discuss their current priorities and concerns in regards to considering FP, and 11 themes emerged. Patients' priorities and concerns were different for those who chose FP and those who did not. For those who chose FP, “prioritizing parenthood” was the top priority or concern. This theme included AYAs mentioning: Parenthood was important, banking gametes was important, the fear of losing their fertility made them consider children, and the risk to their fertility affected them more than their cancer diagnosis. One man mentioned: “The biggest concern was can we still have kids. And once that was over it was like how we go about it wasn't a huge deal.” Patients infrequently discussed adoption and nongenetic children as desirable options.
For those who did not choose FP, the top priority was “focus on cancer treatment.” This theme included a focus on their health, cancer treatment, and survival as priorities. As one woman described: “[Fertility] was kind of an afterthought. My first thought was I have cancer, let's get rid of that first and we will deal with [fertility] later.”
A “fear of future regret” ranked second among priorities for both decision groups. A fear of future regret included patients reporting: keeping their options open, needing fertility risk information, FP providing a security for future children, the risk of being infertile being scary, and that the fertility decision be their own choice. Other priorities and concerns for AYA patients included survivorship quality of life, concerns for having future children, finances, and cultural and social pressures but were reported less frequently (Table 2).
The table is a complete list of the themes and codes identified among a sample of AYA newly diagnosed cancer patients considering fertility decisions. The themes are in reference to patients' priorities at the time of decision making and are ranked in order of frequency from top to bottom. The codes are represented by a sample of direct quotes obtained during in-person interviews after a fertility consultation and are ranked within each theme.
AYA, adolescents and young adults.
Among men and women, the same three themes (parenthood, fear of future regret, and cancer treatment) were ranked among top priorities and concerns when considering FP. Men mentioned “prioritizing parenthood” as the top priority when considering FP, whereas women ranked “fear of future regret” as their top priority. Participants did not bring up considering pressure from their oncologist or their relationship status when discussing their priorities when considering FP.
Informational needs for FP decision making
In discussing patients' informational needs for FP decision making, 10 themes emerged. Between both decision groups, participants similarly agreed that the top informational need was the consideration of their “desire for children,” which was reported 30% of the time. This theme included mention of wanting children, adoption, actively trying to conceive, and conception after cancer.
Patients ranked “desire for FP services” second among informational needs. This included patients discussing: desiring a fertility assessment, oncofertility care after cancer, and options for FP treatments.
Among men and women, the same top informational needs were reported. “Desire for children” was the top reported informational need in considering their FP decision, and the “desire for FP services” was second. One female patient who did not elect FP stressed the importance of having fertility information to make her decision: “For someone that doesn't want to have kids, to be able to talk to doctors and not have them judge you for that decision is great, and to still be given all the information… there is a lot of information that I didn't know.”
Discussion
The FACTS study explored differences in decision making for FP among AYA cancer patients, particularly looking at differences between men and women. Overall, we found that the groups were more similar than different in their reasons, priorities, and informational needs, highlighting the importance of providing information to reproductive-aged newly diagnosed cancer patients. These AYAs expressed a high importance of parenthood after cancer and a fear of future regret without the opportunity to consider FP options. For those who did not choose to undergo FP, their main priority was to focus on their cancer treatment; however, these patients also expressed a fear of future regret and a desire for children.
Parenthood was the most frequently occurring theme when discussing reasons to choose FP and patients' priorities, suggesting that the threat to one's fertility is a critical factor to consider when managing AYA cancer patients. It is the factor that is the most relevant to AYAs choosing FP, even overcoming financial concerns. For our patients, the fertility consultation provided information and a forum to discuss the patient's feelings about parenthood and FP options. The AYAs represented in our study demonstrated coming to terms with their feelings toward future parenthood to come to a harmonious decision. A majority of patients mentioned a fear of regret if they did not pursue FP, whereas patients did not express regret in their final FP decision.
We expected to see AYAs indicate that their oncologist and/or their relationship status were influencers in their FP decisions, as indicated in previous studies.18,25,37–41 However, the interviewed participants did not mention either of these as influencers or priorities in their decision making, leading us to believe that decisions for FP were made independently and that patients came to a decision after weighing their desires and concerns for future fertility.
The major barriers to FP treatment among AYA patients were their concerns about their fertility potential followed by their financial concerns. One-half of patients with financial concerns overcame financial barriers to pursue FP treatment. Only one patient noted having insurance coverage for a portion of the FP procedure. For patients who did not undergo FP, they also identified a lack of access to FP information/services and not prioritizing future children as top reasons against choosing FP. Reproductive-aged patients were the most likely to overcome the barriers for FP when prioritizing future children and by having appropriate access to information and services for FP treatment.
Earlier survivor studies similarly identified that patients' urgency to start treatment, cost, inadequate fertility information, and socio-demographic influences contributed to patients' access to FP services, particularly among women.12–24 In our study, time, age, gender, cultural beliefs, and social pressures had little influence on patients' fertility decisions. When consulting AYAs with a new cancer diagnosis, providers need to be aware of the patient's desire for parenthood and concerns about their future fertility and avoid making referrals based on socio-demographic characteristics or cost concerns.
Strengths and limitations
To our knowledge, this is the first study to look at patients' decision making for future fertility at the time of diagnosis. Often, patients are studied after they lose the opportunity to consider FP or without all the information for considering FP treatment. We have demonstrated in both phases of the FACTS study that FP utilization is increased when patients are provided a fertility consultation. Another strength was our inclusion of both men and women. We know that men are more apt to utilize FP42,43; however, in our study, we have demonstrated that there are few differences in reasoning, priorities, and informational needs between men and women who choose FP and those who do not choose FP.
It is possible that patients in the FACTS study were biased because they received a fertility consultation. Our study sample, however, included patients who were both interested and not interested in future parenthood. Another potential bias is that patients may have received information or opinions about FP before their consultation and were not open to hearing information otherwise. 44 For example, patients still expressed a concern for birth defects or success rates with using assisted reproductive technologies, despite information otherwise. This internal bias, or congeniality bias, 44 suggests that preconceived notions may contribute as to why more patients are not choosing FP.
Conclusion
Young cancer patients who chose FP and those who did not choose FP were so similar in their reasoning and priorities that providers need to consider oncofertility services for all AYA cancer patients. Our study demonstrates the importance of a FP consultation for all patients so that they may contemplate their reasons and priorities for future parenthood. Patients have expressed a desire to participate in their fertility decisions and to receive information regardless of their desire for children or financial concerns. Patients have also demonstrated making independent decisions about their future fertility.
All reproductive-aged patients diagnosed with a new cancer should be referred to a reproductive specialist and provided the opportunity to make their own future fertility decisions before initiating cancer treatment. Informed decision making will lead to AYAs feeling content with their fertility decision and alleviate feelings of regret and frustrations later in life.
Footnotes
Acknowledgments
The authors acknowledge the contributions of Jeanelle Sheeder, Sarah Schmiege, and Allan Prochazka in the design, implementation, and analysis of the FACTS study. This study was funded in part by NIH/NCATS Colorado CTSI Grant Number UL1 TR000154 (DMF), NIH WRHR Award 5K12HD001271-13 (LAK). The content of this article is the authors' sole responsibility and does not necessarily represent official NIH views.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.