
Abstract
There are a number of barriers that result in cancer patients not being referred for oncofertility care, which include knowledge about reproductive risks of antineoplastic agents. Without this information, clinicians do not always make recommendations for oncofertility care. The objective of this study was to describe the level of reproductive information and recommendations that clinicians have available in clinical trial protocols regarding oncofertility management and follow-up, and the information that patients may receive in clinical trials patient information sheets or consent forms. A literature review of the 71 antineoplastic drugs included in the 68 clinical trial protocols showed that 68% of the antineoplastic drugs had gonadotoxic animal data, 32% had gonadotoxic human data, 83% had teratogenic animal data, and 32% had teratogenic human data. When the clinical trial protocols were reviewed, only 22% of the protocols reported the teratogenic risks and 32% of the protocols reported the gonadotoxic risk. Only 56% of phase 3 protocols had gonadotoxic information and 13% of phase 3 protocols had teratogenic information. Nine percent of the protocols provided fertility preservation recommendations and 4% provided reproductive information in the follow-up and survivorship period. Twenty-six percent had a section in the clinical trials protocol, which identified oncofertility information easily. When gonadotoxic and teratogenic effects of treatment were known, they were not consistently included in the clinical trial protocols and the lack of data for new drugs was not reported. Very few protocols gave recommendations for oncofertility management and follow-up following the completion of cancer treatment. The research team proposes a number of recommendations that should be required for clinicians and pharmaceutical companies developing new trials.
Background
I
In male cancer patients, chemotherapy may cause a reduction in sperm count or azoospermia depending on the dose of individual and combined drugs. 5 The effects of chemotherapy on the spermatogonial stem cells may compromise survival of the stem cells and their ability to differentiate, and this may result in permanent infertility. 5 If treatment is limited to the chemotherapy agents that do not kill stem spermatogonia, then normal sperm production can be restored months after the completion of treatment.5,6
In female cancer patients, chemotherapy may cause a reduction in the primordial follicles in the ovary and result in an increase in the decline of oocytes leading to primary or second ovarian failure and premature menopause. 7
Gonadotoxicity is multifactorial, but an important factor is the nature of individual chemotherapy drug and the dose, which may be different in male and female patients. The gonadal toxicity of many of the alkylating chemotherapeutic agents, platinum agents, and anthracyclines are well documented, but other drugs have a similar effect either individually or when combined in multimodality treatment and limited animal or human data are available. 5
Clinical trial protocols should document what the known risks on reproductive health are, for patients receiving chemotherapy treatment, but it is also important to document when data are not available or when potential risk exists based on the class of drug or mechanism of action of a drug.
In the United Kingdom, Australia, and United States, each country has their own requirements for how they report reproductive information in their respective product information (PI) documents; however, none of these countries has an absolute requirement to report effects on fertility, but guidance is given.
In Australia, the information required in the PI document is detailed in subsection 7D(1) of the Therapeutic Goods Act, 1989, which provides guidance for sponsors to document the effects of fertility in the precaution section of the PI form. The use in pregnancy should also be included in the PI using the categories in the Australian Pregnancy Categorisation (genotoxicity, carcinogenicity, use in lactation, and pediatric use). The interpretation of exactly what to include in each section is up to the sponsor. 8
In Europe, the Summary of Product Characteristics 9 fertility reporting suggests that possible effects of medicinal male and female fertility should be included if clinical data are available, and recommendations for the use of the medicinal product when pregnancy is planned should be included. If there are no fertility data at all, then this should be reported.
In the United States, the FDA replaced the five-letter system (A, B, C, D, X) on prescription and biological drug labeling in 2015 by the pregnancy and lactation labeling final rule (see Appendix 2), 10 which now includes narrative sections on the risks during pregnancy and lactation, as well as the risk to male and female reproductive potential.
Oncofertility is a subspeciality that focuses on the collaboration between cancer and fertility specialists to develop reproductive healthcare provisions for cancer patients, maximizing the reproductive health of cancer survivors by discussion, uptake of fertility preservation, and fertility-related psychosocial support, as well as developing new research to prevent infertility.11–13 There are a number of fertility preservation techniques, which are standard practices and recommended by international guidance documents on fertility preservation.14–18 These guidelines give clinicians recommendations about the oncofertility management of cancer patients receiving gonadotoxic risk treatment. Despite these guidelines, less than 50% of patients are currently informed of the reproductive risk of treatment.19–25
There are a number of barriers to delivering oncofertility care, 26 but one barrier that has not been reported on before is the lack of available information that is documented in clinical trial protocols about the gonadotoxic and teratogenic risk of treatment and recommendations for oncofertility care in clinical trial protocols. Clinicians and healthcare professionals look to these clinical trial protocols to guide the work-up, treatment, and subsequent follow-up of patients, and our research group was interested in defining how much information clinicians are given. The documentation about reproductive risks is an important factor that allows the translation of knowledge about reproductive risk into adequate oncofertility care, and the lack of this information may limit improvements in the oncofertility care of cancer patients.
Hypothesis
The reproductive complications of cancer treatment are poorly documented in clinical trial protocols, and limited advice on oncofertility assessment, management, and follow-up is provided to clinicians who are using these protocols.
Purpose
The aim of this study was to describe the level of reproductive information available to clinicians in clinical trial protocols and for patients in the information sheets or consent forms. The secondary aim was to describe the recommendations for oncofertility investigation and management documented for clinicians in the clinical trial protocols and compare these data with the available published literature on reproductive risk of individual chemotherapy agents.
Methods
The authors identified and reviewed 78 Australian, American, and European clinical trial protocols opened between 1996 and 2016. Ten protocols were excluded as they either did not use chemotherapy agents or only included nonchemotherapy drugs such as androgen inhibitors. The protocols were chosen as they have been used to treat pediatric patients or patients of a reproductive age (15–45 years of age) with either a hematological or oncological cancer diagnosis common in this age group, who are at risk of treatment-related infertility. Only studies with complete protocols were included in the review.
The full protocol, information sheets, and consent forms were reviewed by four researchers and data were collected documenting a number of variables:
(1) Type of protocol (disease treated, type of trial, and age of patients treated) (2) Recommendations on the gonadotoxic risk for each individual drug (3) Recommendations on the gonadotoxic risk of completed protocols (4) Recommendations about the teratogenic effect of chemotherapy and management (5) Recommendations on fertility preservation before or after cancer treatment given in the protocol or available on patient information sheets (6) Recommendation for reproductive follow-up following the completion of treatment (7) The usability of the protocol for oncofertility information
Four researchers then performed a literature review on the gonadotoxic and teratogenic risk of the 71 antineoplastic agents identified from the 68 protocols to look at current evidence on the gonadotoxic and teratogenic risk of treatment and compare the evidence from animal and human trials to what was reported in the 68 clinical trial protocols reviewed. Unfortunately, as limited data were available in the literature, the researchers also looked at the PI sheets and pharmaceutical websites for gonadotoxicity information.
Statistics
Descriptive statistics (percentages) were used to describe information associated with the level of gonadotoxic and reproductive information as well as recommendations provided in clinical trial protocols, and compare data that were available and documented in the literature. Data analysis was performed using STATA software, version 14.0 (StataCorp LP, TX).
Results
There were 68 reviewed protocols for infant, pediatric, adolescent young adult (AYA), and adult aged cancer patients. One of 68 (1%) was an infant protocol, 26/68 (38%) were pediatric and AYA protocols, 26/68 (39%) were adult protocols, and 14/70 (21%) were protocols that covered all age groups.
The protocols covered 30 different cancer types. Twenty-four of 68 (35%) were protocols for leukemia and lymphomas, 5/68 (7.35%) for brain tumors, and 39/68 (57%) for solid tumors. The protocols covered all clinical trial stages: 11/68 (16%) were phase 1 protocols, 7/68 (10%) were phase 1/2 protocols, 9/68 (13%) were phase 2 protocols, 3/68 (4%) were phase 2/3 protocols, and 38/68 (56%) were phase 3 protocols.
A literature review on the teratogenic and gonadotoxic effects of individual drugs did not provide much original research data; so the PI and prescribing information sheets were also reviewed. Of the 71 antineoplastic drugs, included in the 68 clinical trial protocols reviewed, 68% of the antineoplastic drugs had gonadotoxic animal data, 32% had gonadotoxic human data, 83% had teratogenic animal data, and 32% had teratogenic human data (Table 1).
5FU, 5-fluorouracil; AUC, area under the curve; BRAF, proto-oncogene B-Raf; CNS, central nervous system; FEC, fluorouracil, epirubicin, cyclophosphamide; FSH, follicle-stimulating hormone; IV, intravenous; LH, luteinizing hormone; mTOR, mammalian target of rapamycin; PARP, poly ADP ribose polymerase; PD-L1, programmed death-ligand 1; PD1, programmed cell death protein 1; PI3K, phosphoinositide 3-kinase inhibitor; VEGF, vascular endothelial growth factor.
A review of the 68 protocols showed that information about the gonadotoxic risks were only documented in 22 of the 68 protocols (32%). Forty-six of the protocols (68%) did not document the gonadotoxic risk of treatment in the protocol. The only available infant protocol did not have information on the gonadotoxic risk of the treatment. Ten out of the 26 (38%) pediatric and AYA protocols, 6/27 (22%) of the adult protocols, and 6/14 (43%) of the protocols covering the combined pediatric, AYA, and adult age group had information on the gonadotoxic risk of the treatment protocol.
Nine of 68 protocols (13%) were open during 2005–2008 and of these protocols, 5/9 (56%) had gonadotoxic information available, 18/68 protocols (26%) were open during 2009–2012 with 6/18 (33%) having gonadotoxic information included, and 39/68 protocols (57%) were open during 2013–2016, with only 9/38 (23%) having any gonadotoxic information available. There were only 2/68 protocols (3%) that were opened before 2005.
Gonadotoxicity data were available in 3/11 (27%) phase 1 protocols, 1/6 (14%) phase 1/2 protocols, 6/9 (66.67%) phase 2 protocols, 2/3 (67%) phase 2/3 protocols, and 10/38 (26%) phase 3 protocols.
Only 15/68 protocols (22%) documented the teratogenic risk in the protocol and 53/68 of the protocols (78%) did not have any information available regarding the teratogenic risks of treatment. However, 60/68 (88%) protocols had information on the recommendation for contraceptive management during treatment.
Nine of 68 (13%) protocols were opened during 2005–2008 and of these protocols, 2/9 (22%) had teratogenic information available. Eighteen of 68 protocols (26%) were opened during 2009–2012, of which 4/18 (22%) had teratogenic information. Thirty-nine of 68 (57%) protocols were opened during 2013–2016 with 8/38 protocols (21%) providing teratogenic information.
Teratogenic data were available in 4/11 (36.36%) phase 1 protocols, 2/7 (29%) phase 1/2 protocols, 2/9 (22%) phase 2 protocols, 2/3 (66.67%) phase 2/3 protocols, and 5/38 (13%) phase 3 protocols.
There were only 6/68 protocols (9%) that provided recommendations for fertility preservation before cancer treatment (4 pediatric and AYA protocols, 1 adult protocol, and 1 protocol covering the pediatric to adult age range). Three of 68 protocols (4%) gave recommendations for reproductive follow-up in the survivorship period. Only 18/68 protocols (26%) had a section in the protocol that had all the oncofertility information easily identified.
Seventy-one individual chemotherapy and antineoplastic drugs were classified into 19 classes of drugs (10 alkylating agents, 8 monoclonal inhibitors, 8 antimetabolite inhibitors, 6 tyrosine kinase inhibitors, 6 plant alkaloids, 4 immune checkpoint inhibitors, 4 antitumor agents, 4 anthracyclines, 4 poly (ADP-ribose) polymerase (PARP) inhibitors, 3 antineoplastic agents, 2 mechanistic target of rapamycin (mTOR) inhibitors, 2 topoisomerase inhibitors, 2 platinum agents, 2 Vascular endothelial growth factor (VEGF) inhibitors, 2 protease inhibitors and 1, phosphoinositide 3-kinase inhibitor (PI3K inhibitor), 1 proto-oncogene B-Raf (BRAF) inhibitor, 1 histone deacetylase inhibitor, and 1 hedgehog inhibitor).
In every class of drug, there was a significant reduction in the available gonadotoxic and teratogenic information in the clinical trial protocols compared to the available information in the literature (Figs. 1 and 2).
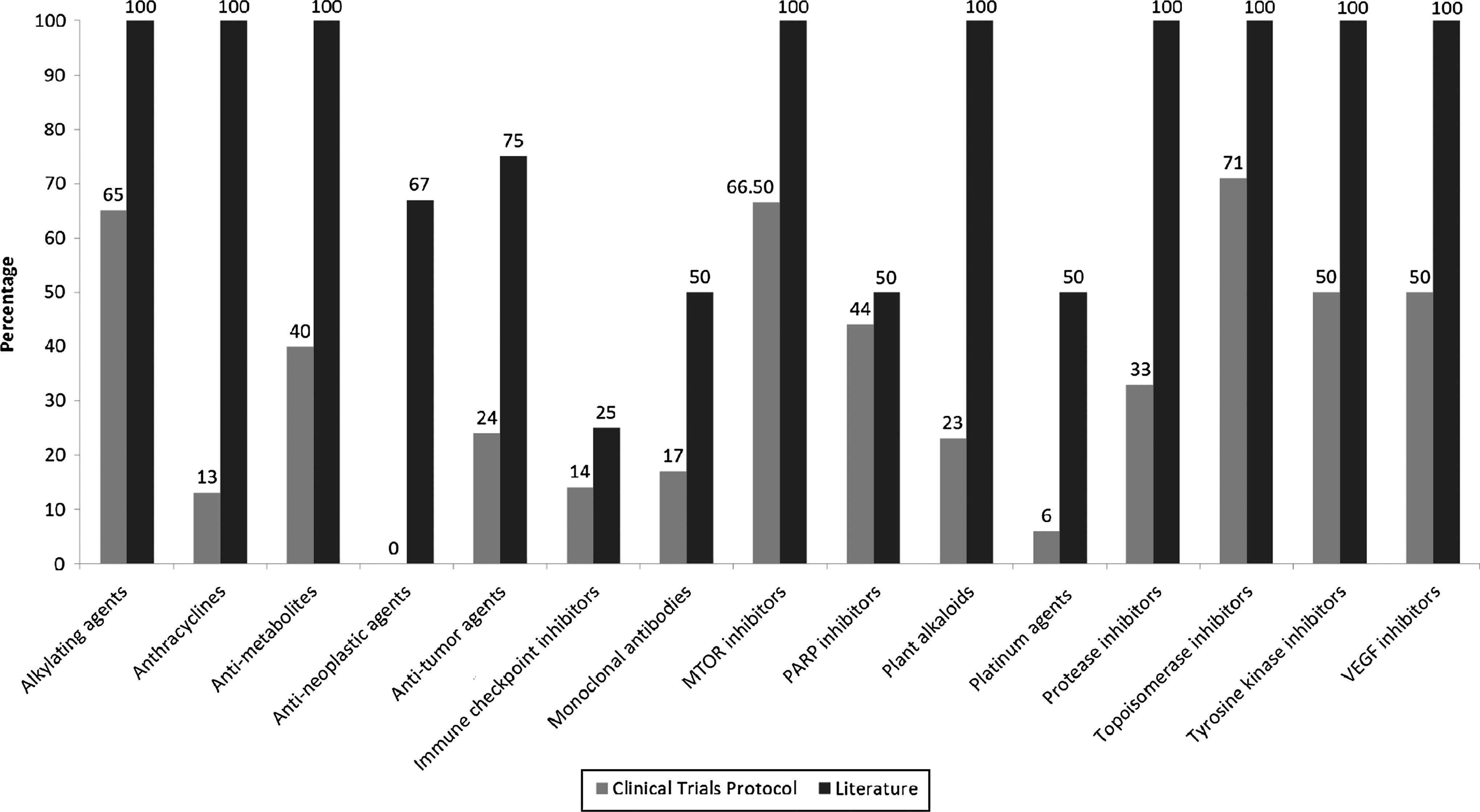
Comparison between gonadotoxic information available in the literature and in the clinical trials protocol.

Comparison between teratogenic information available in the literature and in the clinical trials protocol.
The research team did not demonstrate any difference in the documentation of reproductive risk in protocols from protocols of different countries.
Limitations
The researchers reviewed all open protocols available during the study time period, which were available in both pediatric and adult oncology units. The research group also reviewed International clinical trial protocols in English available from clinical trials group websites. This reflects a small number of clinical trial protocols used to treat cancer patients in these age groups. However, the results of this study demonstrate a clear lack of clinical care information across both pediatric and adult centers internationally. The researchers only reviewed the initial version of the study protocols; subsequent versions of the protocol were not reviewed.
Discussion
What is currently documented?
This research study has shown a significant difference between what is known about the gonadotoxic and teratogenic risks of treatment compared to what is reported in the literature or in published PI sheets. Data in this study showed that where information is clearly known about the gonadotoxic and teratogenic risk about drugs like alkylating agents, anthracyclines, and platinum agents, the gonadotoxic and teratogenic data are still poorly reported and this has not changed significantly over the past 15 years, despite an improved focus on survivorship care and fertility preservation. The available oncofertility information was often poorly organized within protocols rather than having a section on reproductive risk and management.
To gather clear information about the reproductive concerns of individual drugs required multiple different literature reviews to develop an understanding of the gonadotoxic and teratogenic risk of individual chemotherapy agents. The available data did not consistently follow either the old or new FDA nomenclature or country-specific nomenclature for defining what the risks are during pregnancy, breast feeding, or male or female reproductive potential. The gonadotoxic risks are usually not clearly defined in terms of low, intermediate, or high risk of causing infertility with the exception of the alkylating and anthracycline data, which make recommendations for fertility preservation very difficult.
Many of the novel agents do not have any human data on reproductive risks, but they do report animal data or post-marketing data highlighting a concern. Others have a proposed risk on reproductive health based on the mechanism of action. The clinical trial protocols reviewed do not contain adequate information to sufficiently advise clinicians, patients, and parents about the concerns of these new classes of drugs, and this is even more concerning as fewer clinicians would know the risks of new classes of drugs without reviewing the literature. It is important that either the unknown risk or the potential risk due to the mechanism of action or animal data are included in all clinical trial protocols with some recommendations about oncofertility care.
As more novel and immunotherapy agents are being developed and included in clinical trial protocols, it will be very important for information on the reproductive risk to be collected so that patients and clinicians can make informed decisions about choices of treatments based on the improvements in survival and well as side-effect profiles.
Understanding the risk of the whole protocol
A significant number of patients will have multimodality treatment with surgery, radiotherapy, or bone marrow transplantation, and the combined risk may be higher than the individual risk of individual chemotherapy drugs. Thus, it is important for protocols to give a risk projection for the whole protocol, not just for a component of the treatment regimen, unless the patient's survival does not depend on all phases of treatment. In cases when a treatment protocol has different phases, depending on risk stratification, the gonadotoxic and teratogenic risk of each component should be documented.
Precision medicine
Precision medicine is changing the way in which we treat cancers. Many patients will be taking targeted treatments for longer periods of time and patients will be living with their cancers as a chronic disease rather than being cured and ceasing treatment. Cessation of treatment at a later date, to allow patients to undergo fertility preservation, may not be possible, and even if there was a window of opportunity, it may not be long enough to reduce the teratogenic effects of prior chemotherapy. The patient may have also missed the window of opportunity to have fertility preservation. Therefore, clinicians should participate in international studies to collect fertility preservation data so that the short- and long-term risks of new treatments can be documented and clearer recommendations made about fertility preservation. 451
Oncofertility assessment and management
The reviewed protocols show that oncofertility assessment and management are not being incorporated consistently in the toxicity assessment of cancer patients who are post-pubertal and have fertility preservation choices. Fertility preservation in pre-pubertal patients is still experimental, however, clinicians, patients, and parents need to be aware of the potential risks so that appropriate follow-up can occur or timely consideration can be provided for referral for fertility preservation under research parameters.
What do our patients want?
Consumers have indicated that they would like more data on oncofertility-related risk, better communication, access to fertility-related decision aids, and the availability of oncofertility referral pathways. 452 The late effects of cancer treatment can impact survivorship immensely, and with increasing cure rates, we must make sure that patients and parents are well informed to be able to make choices for the future. Treatment decisions can be enhanced with the inclusion of more reproductive information and with warnings about the risks of infertility incorporated into the clinical trial protocols and informed consent documents.
It is important that pharmaceutical companies are made aware of the effects that reproductive complications may have on cancer patients and routinely collect information on the reproductive risk of new drugs in all phases of clinical development.
The data reported indicate that gonadotoxic and teratogenic information are not readily available across all phases of development, and phase 3 protocols do not provide any more data compared with early phase protocols. This may arise from the lack of data collected during pre-clinical and clinical development.
Conclusion
The actual or potential reproductive concerns of cancer treatment are poorly documented in clinical trial protocols and limited information is given about oncofertility assessment and follow-up. As these protocols are used by clinicians to base toxicity assessments and follow-up care, it is important for the clinical trials development team to include up-to-date information about reproductive concerns as well as recommendations about oncofertility care. Internationally, a number of guidelines are available that include standard oncofertility assessment, management, and follow-up of pediatric and adult cancer patients, which could be referenced or included in the clinical trial protocols.453–457 Better clinician knowledge about the reproductive risk of treatment may lead to an increase in discussion about reproductive risk and referral for oncofertility consultation and management.
It is also important for the clinical trial teams and pharmaceutical groups to collect data on the reproductive concerns of new novel agents, so that successful drugs, included in phase 2–3 studies, have animal and human data on reproductive concerns. Our study showed that reproductive knowledge about chemotherapy agents was not reported adequately in phase 3 trials. This is important as a large number of the new novel agents have limited data available in this area and are currently being used in phase 1 and 2 trials.
Recommendations
The research team proposes a number of recommendations that should be required for clinicians and pharmaceutical companies developing new trials. These recommendations will enable clearer information and recommendations for oncofertility care, which will lead to improved reproductive outcomes:
(1) The gonadotoxic and teratogenic risk of individual chemotherapy drugs and combined effect of the treatment protocol should be clearly documented in every new protocol that is developed as per the new FDA recommendations. (2) If gonadotoxic and teratogenic information are not available for individual chemotherapy agents, then this should also be documented and guidance provided regarding the class or mechanism of action of the chemotherapy drug. (3) Protocols should include recommendations for oncofertility management at diagnosis and follow-up within the toxicity assessment section of a protocol so that doctors can ensure that, when necessary, fertility preservation is included as part of follow-up and standard practice in the same way that audiology, echocardiograms, and glomerular filtration rate assessments are recommended based on the toxicity profile of a protocol. (4) Clinical trial protocols focusing on new drugs should collect short- and long- term data on the reproductive effects of treatment for all phases of clinical trials. This will help define the reproductive risks of treatment and will allow doctors to make recommendations on oncofertility assessment and management in the future. (5) Cancer clinicians should participate in the collection of oncofertility data so that the reproductive concerns of treatment can be documented consistently and data collected on the benefits of fertility preservation strategies.
Future directions
The researchers believe that the information from this study has significant relevance for both clinicians and researchers to address the gaps in oncofertility knowledge and care provided. The next phase will be to develop resources using our data for clinicians and patients so that information about the reproductive concerns can be identified quickly and recommendations made.
The researchers are also looking at the development of animal model trials for new novel agents to provide more extensive knowledge in this area.
Footnotes
Acknowledgments
The authors express their gratitude for the New York University at Sydney faculty, Ms. Sarah Naderi and staff at the University of New South Wales who made this internship possible. We also thank the FUTuRE Fertility Research team, Joanne O'Brien from the Prince of Wales Hospital Pharmacy, Dr. Dan Stark Adolescent Oncologist at St. James's Institute of Oncology, St. James's University Hospital, and Dr. Lorna Fern, NCRI Teenage and Young Adult Clinical Studies Group.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1. Old FDA Pregnancy Categories: 21 CFR 201.57 (c)(8)(i)
(A) Generally acceptable. Controlled studies in pregnant women show no evidence of fetal risk.
“If adequate and well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus in the first trimester of pregnancy (and there is no evidence of a risk in later trimesters).”
(B) May be acceptable. Either animal studies show no risk, but human studies not available, or animal studies showed minor risks and human studies done and showed no risk.
“If animal reproduction studies have failed to demonstrate a risk to the fetus and there are no adequate and well-controlled studies in pregnant women.”
(C) Use with caution if benefits outweigh risks. Animal studies show risk and human studies not available or neither animal nor human studies done.
“If animal reproduction studies have shown an adverse effect on the fetus, if there are no adequate and well-controlled studies in humans, and if the benefits from the use of the drug in pregnant women may be acceptable despite its potential risks.”
(D) Use in LIFE-THREATENING emergencies when no safer drug available. Positive evidence of human fetal risk.
“If there is positive evidence of human fetal risk based on adverse reaction data from investigational or marketing experience, or studies in humans, but the potential benefits from the use of the drug in pregnant women may be acceptable despite its potential risks (for example, if the drug is needed in a life-threatening situation or serious disease for which safer drugs cannot be used or are ineffective).”
(X) Do not use in pregnancy. Risks involved outweigh potential benefits. Safer alternatives exist.
“If studies in animals or humans have demonstrated fetal abnormalities or if there is positive evidence of fetal risk based on adverse reaction reports from investigational or marketing experience, or both, and the risk of the use of the drug in a pregnant woman clearly outweighs any possible benefit (for example, safer drugs or other forms of therapy are available).”
(NA) Information not available.
Appendix 2. The Pregnancy and Lactation Labeling Final Rule: 21 CFR 201.57 (c)(9)
Prescription drugs submitted for FDA approval after June 30, 2015, will use the new format immediately.
Labeling for prescription drugs approved on or after June 30, 2001, will be phased in gradually.
Medications approved before June 29, 2001, are not subject to the Pregnancy and Lactation Labeling Final Rule (PLLR) rule, however, the pregnancy letter category must be removed by June 29, 2018.
The A, B, C, D, and X risk categories are now replaced with narrative sections and subsections to include the following:
Pregnancy Exposure Registry
Risk Summary
Clinical Considerations
Data
Risk Summary
Clinical Considerations
Data
Pregnancy Testing
Contraception
Infertility