
Abstract
Purpose:
This study aimed to establish teenage and young adult cancer survivors (TYACS') specific interest in receiving information on physical activity, diet, smoking, and alcohol consumption and their preferences regarding the delivery, format, and timing of such health behavior information.
Methods:
TYACS aged 13–25 years were invited to complete a questionnaire assessing the advice they had received in the past and their preferences on when and how health behavior information should be delivered.
Results:
A total of 216 TYACS (mean age: 20 years; mean age at diagnosis: 16 years) completed the questionnaire. Approximately 40% of TYACS received no advice on physical activity and diet, and more than half (54%) received no advice on weight management. The majority (>70%) reported receiving no advice on smoking or alcohol consumption. Interest in receiving lifestyle advice was high overall (71%) but varied across behaviors, with TYACS reporting a greater level of interest in receiving advice on health protective behaviors (physical activity and diet) than health risk behaviors (smoking and alcohol consumption) (∼85% vs. ∼15%, respectively). TYACS reported seeking health behavior information from health professionals and were most interested in information delivered online or in the form of a mobile app. Similar proportions (18%–29%) felt health behavior information should first be provided before, during, immediately after, and post-treatment.
Conclusions:
It is evident that there is a need to develop lifestyle interventions in a range of formats available to TYACS throughout the care pathway to address the health behavior information needs of young people with cancer.
Introduction
I
However, despite the numerous benefits of healthy lifestyle behaviors, cross-sectional survey data indicate that a large proportion (∼50%) of TYACS are inactive,8,9 overweight,10,11 regularly drink, 12 and consume unhealthy diets that are low in fruits, vegetables, and key nutrients such as vitamin D and calcium.13–15 Moreover, although the prevalence of smoking has dropped in the past decade, recent estimates indicate that 14% of TYACS are current smokers. 16
Lack of information or guidance on making a healthy lifestyle may partially explain the prevalence of poor health behavior among TYACS. In previous research, TYACS had cited the absence of relevant information resources as a barrier to making healthy lifestyle choices,17,18 whereas among colorectal cancer patients (n = 15,254) recall of being given advice on physical activity was associated with greater odds (OR = 1.90, 95% CI 1.75–2.09, p < 0.001) of meeting the national physical activity guidelines of 30 minutes of brisk activity per day. 19 Intervention studies conducted among TYACS have also shown promising evidence that health behavior information, specifically risk-based information, can improve young peoples' health behavior. 20 In reflection of this, the provision of timely and appropriate information on health behavior is increasingly being acknowledged as a key priority within TYA cancer care.21,22
However, the health behavior information needs of TYACS are often described as being unmet9,23 and in the past TYACS had explicitly described health promotion as being an “overlooked” aspect of their care. 24 One study of TYACS (n = 74, mean age: 22.9 years) in the United States found that only 55% had received exercise information following their cancer diagnosis, despite 85% indicating that they would have liked such information and support. 9 Very little is known regarding TYACS' specific interest in, or experience of, receiving information on more sensitive health topics such as weight management, smoking abstinence, or alcohol consumption. Qualitative evidence and general reports indicate that health professionals working with TYACS often face multiple barriers (including lack of time, resources, financial support, and referral options) when addressing the health behavior needs of young people who have had cancer. 25 Health behavior intervention resources, containing relevant information on physical activity, diet, smoking, and alcohol consumption, have the potential to not only directly improve TYACS health behavior but also support health professional to deliver information and engage TYA patients in conversation on these topics.
This study aimed to establish TYACS' interest in receiving information on physical activity, diet, weight management, smoking, and alcohol consumption and their preferences regarding the format, delivery, and timing of such information. Such data, gathered from a patient-centered perspective, is central to the development of health behavior change resources for young people with cancer. 26
Methods
Participants and recruitment
TYACS were recruited through the University College London Hospital (UCLH) or project partners CLIC Sargent (a UK cancer charity for children and young people) between May 2015 and April 2016. A Health and Lifestyle Questionnaire was advertised in patient waiting areas at UCLH and in the online forums and participation networks of CLIC Sargent. In alignment with the National Cancer Institute (NCI) definition 24 of a cancer survivor, any young person between the age of 13 and 25 years who had been diagnosed with cancer at any point in their lifetime was eligible to complete the questionnaire; this included those aged 13–25 years who had been diagnosed with cancer during their childhood (aged 0–12 years). The inclusion criteria were deliberately kept broad to capture a wide cross-section of TYACS' views on health behavior advice, rather than limiting to specific age or disease groups. TYACS were eligible to complete the survey regardless of their treatment status. TYACS who identified themselves as eligible had the option to complete the questionnaire either in electronic format online or in paper format. By completing and returning the survey, participants were made aware that they were consenting to their anonymous data being used for analysis. Ethical approval for this study was provided by the University College London Research Ethics Committee reference: 6206/001 and London Hampstead Research Ethics Committee reference: 15/LO/0764.
Measures
Questions contained within the TYACS Health and Lifestyle Questionnaire were adapted from a large-scale survey of adult-aged cancer survivors. 25
Demographic and health status
Participants were asked to report their age, sex, highest level of educational attainment, marital status, current living arrangement, ethnicity, type of cancer diagnosed with, date of diagnosis, current treatment status, and any health problems (other than cancer) they suffer from.
Health behavior information and advice received
Participants were asked to report if, since being diagnosed with cancer, they had ever received information or advice on five health behaviors (physical activity, diet, weight management, smoking, and alcohol consumption) from a health professional involved with their cancer treatment. Those who indicated that they had received health behavior advice were asked to provide specific details of the advice they were given and report who had provided the advice in an open response format. Participants were also asked to report whether they thought the amount of health behavior advice they had received was too little, too much, or about right.
Health behavior information and advice preferences
Participants were asked to report their level of interest in receiving information and advice on all health behavior topics covered within this study. Participants were also asked to indicate whether they would have taken up the offer of health behavior advice at the end of their initial treatment and whether they would take up the offer now. TYACS were also asked to report when they thought the best time to offer lifestyle information to young people with cancer would be and their level of interest in various advice formats. Participants were also asked to indicate the source(s) that they typically consult for health behavior information.
Statistical analysis
Littles Missing Completely at Random test was performed to evaluate the patterns of missing data. 26 Descriptive statistics were used to (a) characterize participants and to examine the cancer history and health status of the sample; (b) determine the proportion of TYA cancer survivors who reported receiving health behavior advice and their views on the amount of advice they were given; and (c) gauge TYACS' interest in lifestyle information and preferences regarding information delivery. Logistic regression models were used to explore associations between participant characteristics (age, sex, age at diagnosis, treatment status, and number of health problems) and both past experience of receiving advice (received vs. not received) and interest in advice (interested vs. not interested) on each behavior. Chi-square (χ2) analyses were performed to examine potential differences in TYACS preferences regarding the timing of information delivery. Open-response answers were coded line by line and analyzed according to Elo and Kyngäs' process of content analysis. 27 In total, 441 individual open-response comments were analyzed. Cohens kappa was run to determine the inter-rater reliability of the content analysis.
Results
A total of 294 TYACS started the Health and Lifestyle Questionnaire and provided at least one answer to a question contained within the survey; unfortunately, due to survey dropout, only 216 TYACS provided data on key variables required for this study. Within this study, any residual missing data points were deemed to be missing completely at random, as there were no systematic differences between missing and observed values (χ2 = 0.00, df = 0, p > 0.05), indicating no key demographic differences between completers and noncompleters. Any residual missing data were imputed based on simple means; a total of 40 individual data points (0.5% of the total data set) were imputed. There was a good level of inter-rater agreement on qualitative data (Cohens kappa >0.6, p < 0.005).
Sample characteristics
Participant characteristics are displayed in Table 1. Participants (n = 216) had an average age of 20 years (standard deviation [SD] = 2.85; range 13–25 years), were predominantly female (n = 130, 60%), White British (n = 183, 85%), and living at home with their immediate family (n = 163, 75%). Most participants (n = 91, 42%) reported still being in full-time education; however, 23% (n = 49) of TYACS within this study reported being either unable or too ill to work.
Where percentages do not equal 100%, this was due to participants selecting all that applied.
SD, standard deviation.
Table 2 outlines the health and treatment characteristics of all participants. The most common cancer diagnoses were hematological malignancies (lymphoma/leukemia) (n = 126, 59%), bone tumors (n = 22, 10%), and soft tissue sarcomas (n = 20, 9%). Average age at diagnosis was 16.8 years (SD = 4.0; range of age at diagnosis: 0–24 years). At the time of survey completion, the majority of respondents (n = 148, 69%) had finished cancer treatment, with just less than half reporting that they were more than 12 months from the end of treatment (n = 92, 44%). Two-thirds (n = 141, 65%) reported suffering from one or more health problems other than their original cancer diagnosis. Table 3 displays the range of health problems suffered by participants. The most common health difficulties were extreme fatigue (n = 66, 31%) and mental health problems (n = 40, 19%).
Where percentages do not equal 100%, this was due to participants selecting all that applied.
Health behavior advice received since diagnosis
Figure 1 displays the proportion of participants who reported receiving advice on each health behavior since their cancer diagnosis. Approximately 40% of TYACS reported receiving no advice on physical activity and diet, most (n = 117, 54%) reported receiving no advice on weight, and the majority (≥70%) reported receiving no advice on smoking or alcohol consumption.
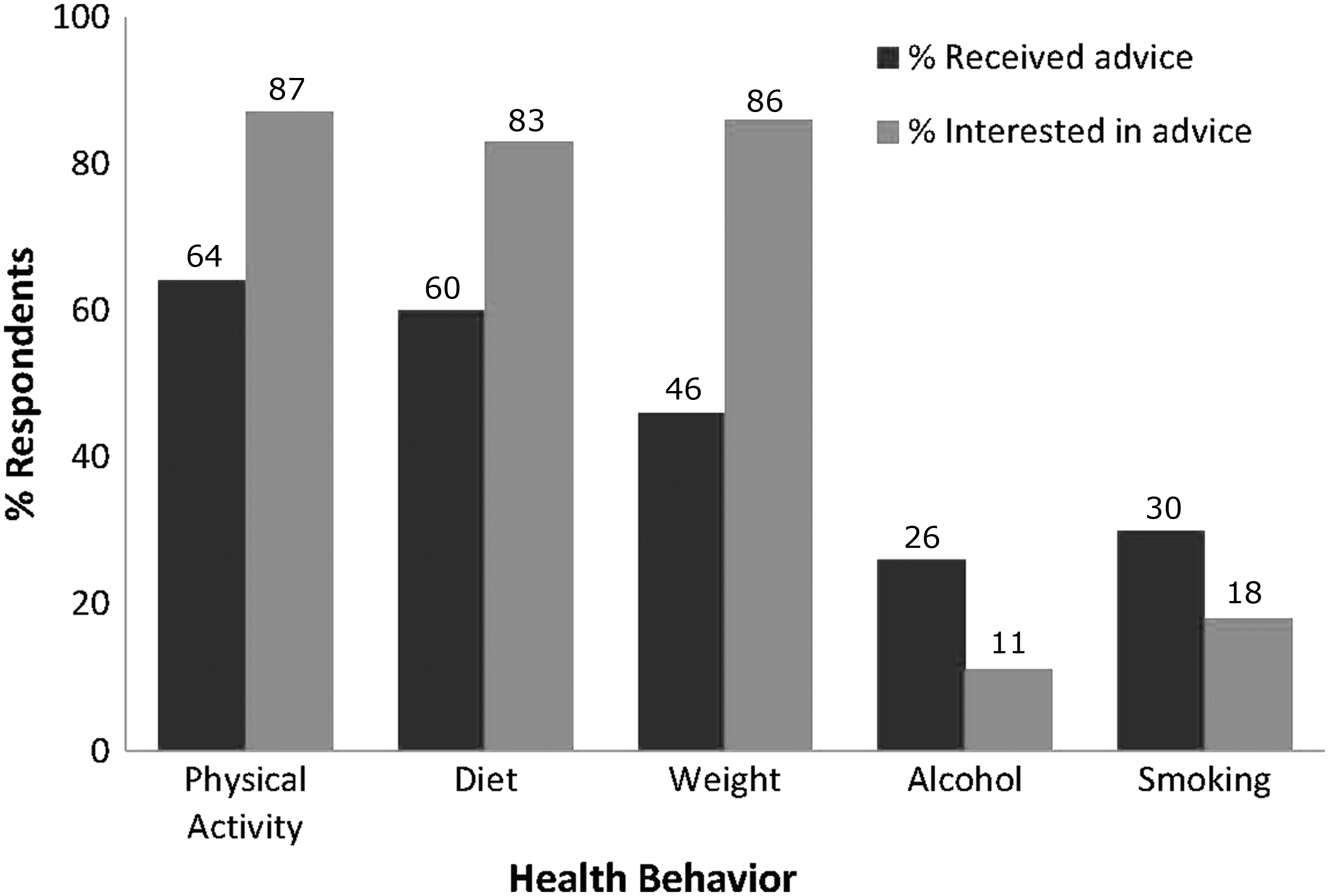
Proportion of TYACS who received health behavior advice since diagnosis and their interest in health behavior information. TYACS, teenage and young adult cancer survivors.
Primary treating physicians (oncologists) were the main source of information for TYACS on physical activity, smoking, alcohol consumption, and weight management, whereas most TYACS reported receiving advice on diet from a dietician. Participants' open-response answers describing the advice they had received in the past are shown in Table 4. Much of the health behavior advice that participants reported receiving was general advice about maintaining a healthy lifestyle; however, many participants reported receiving specific advice that was related to cancer management. Specifically, participants reported being told to remain active during and after their treatment to help with recovery and to manage cancer-related fatigue. With regard to diet, advice often centered on weight management, with many participants reporting that the advice they received was predominantly about calorie intake. Most TYACS reported that they were actively discouraged from smoking and that they were advised to either not drink or reduce the amount they drink.
Participant characteristics are displayed in brackets.
TYACS who reported being ≥18 years of age at diagnosis were more likely to report having received advice on diet (OR = 1.82, 95% CI 1.02–3.23, p = 0.04) and weight (OR = 2.61, 95% CI 1.435–4.754, p = 0.002) than those aged <18 years at diagnosis. Unsurprisingly, TYACS ≥18 years of age at the time of the study were more likely than TYACS aged <18 to report receiving advice on smoking (OR = 0.377, 95% CI 0.18–0.78, p = 0.009) and alcohol consumption (OR = 0.402, 95% CI 0.18–0.85, p = 0.018). There were no other significant relationships between participant characteristics and the receipt of lifestyle advice.
The majority (n = 170, 79%) felt that the amount of information they had received in the past was “about right.” Only 19% (n = 42) felt they had not received enough information, and 2% (n = 4) thought they had been given too much information.
Interest in health behavior information
Seventy-one percent of participants (n = 153) reported that they would take up the offer of health behavior information, advice, and support if given the opportunity. The most commonly desired topic of advice was physical activity (n = 188, 87%), closely followed by weight (n = 187, 87%), and diet (n = 180, 83%) (Fig. 1). Only 18% (n = 39) and 11% (n = 24) of TYACS surveyed reported an interest in advice on smoking and alcohol consumption, respectively.
TYACS aged >18 were significantly less likely than 13- to 18-year-old TYACS to report being interested in advice on diet (OR = 0.41, 95% CI 0.18–0.89, p = 0.024) and general lifestyle (OR = 0.42, 95% CI 0.18–0.96, p = 0.040), whereas women in comparison to men were more likely to be interested in advice on alcohol consumption (OR = 3.67, 95% CI 1.31–10.29, p = 0.013). There were no other significant relationships between age, gender, age at diagnosis, current treatment status, number of health problems, and interest in advice for each health behavior.
Sources from which TYACS seek health behavior information
Figure 2 outlines the range of sources that TYACS report consulting for information on each health behavior topic. TYACS typically seek information on physical activity and diet from online websites, whereas health professionals are the preferred source of information on weight, smoking, alcohol consumption, and general lifestyle advice. Very few TYACS (<15%) indicated that they would seek health behavior information from their friends, parents, telephone helplines, or YouTube. Nonetheless, a greater proportion of TYACS reported asking for advice or information from their friends rather than their parents about smoking (11% vs. 5%) and alcohol consumption (15% vs. 7%).

Sources that TYACS consult for information on each health behavior.
Preferences regarding health behavior information delivery
The vast majority of participants reported that they would prefer health behavior information to be available online (n = 190, 88%) or in the form of apps (n = 184, 85%) and indicated a preference for short information leaflets over longer booklets (78% vs. 66% respectively). Sixty-eight percent (n = 147) reported that they would be interested in one individual counseling session. Group counseling sessions and a telephone call from a health professional were found to be the least popular formats of advice and information delivery.
Seventy-six percent (n = 108) of TYACS who had finished their cancer treatment felt that if given the opportunity they probably would have taken up the offer of information and support on health behavior at the end of their main treatment. Table 5 displays TYACS' preferences on the best time to offer health behavior information to young people with cancer. Unsurprisingly, TYACS on treatment at the time of the study reported a greater interest in receiving advice during the treatment phase of the cancer continuum, particularly before treatment begins (35% vs. 21%, χ2 (5, N = 210) = 17.807, exact p = 0.002). No other participant characteristics were found to predict timing preference. As a collective sample, most participants (29%, n = 62) felt that health behavior information and advice would be best provided immediately after treatment; a similar proportion of participants felt that health behavior information would be best provided before treatment starts (n = 56, 26%), during treatment (n = 39, 18%), and 3–5 months after treatment (n = 45, 21%).
Data on treatment status missing for six participants.
TYACS, teenage and young adult cancer survivors.
Discussion
Interventions that contain relevant health behavior information have the potential to improve the physical activity, dietary, smoking, and drinking behaviors of TYACS by increasing knowledge and awareness of the importance of healthy lifestyle choices; improving positive attitude and intentions toward positive health behavior choices; and acting as a cue to positive behavior change. However, findings from this study indicate that TYACS often do not receive health behavior information or advice as a part of routine care, particularly on sensitive health topics such as weight management, smoking, and alcohol consumption. TYACS were predominantly interested in information on physical activity, diet, and weight management and reported seeking advice from health professionals and websites. No consensus was reached as to when information or advice on health behavior should first be provided, with fairly equal proportions of TYACS indicating that health behavior information should be provided before treatment, during treatment, and after treatment.
TYACS' high level of interest in receiving information on physical activity, diet, and weight management is encouraging and reflects findings from previous research exploring the long-term follow-up preferences and psychosocial support needs of young people with cancer.9,16,28 However, the finding that very few TYACS report past experience of receiving, or any interest in receiving, information on smoking and alcohol consumption is concerning given the well-established risks that these behaviors have on current and future health among TYACS. 29 Previous narrative reviews exploring the risk-taking behaviors of TYACS have acknowledged that counseling TYACS on smoking and alcohol consumption is a challenge given that experimentation with such behavior is often a standard part of youth culture. 30 A qualitative study exploring the late-effects information needs of adult-aged survivors of childhood and adolescent cancer identified ambivalence to receiving health risk information as a core theme. 31 Participants in the study indicated being passive toward the importance of receiving detailed information on late effects during adolescence, and they were only aware of the importance of being fully informed about health risks faced by TYACS in hindsight as adults. A similar notion may apply to information on smoking and alcohol consumption; young people with cancer may be unaware and uninterested in their need for the information on these health behaviors, but receiving such information may be crucial in prompting TYACS to make and sustain positive lifestyle choices. Previous intervention studies conducted among TYA-aged childhood cancer survivors have reported intensive late-effects counseling, containing explicit information on the risks of tobacco use, to be effective at improving health knowledge and lowering intentions to smoke. 32 As such, it is clear that despite TYACS' apparent disinterest in information on smoking and alcohol consumption, efforts to provide TYACS with such information should be continued.
TYACS within this study most commonly reported seeking information and support on health behavior from either health professionals or websites. This was to be expected given the close and trusting relationships that TYACS often have with health professionals 33 and the prolific use of the internet among TYAs in general. 34 A recent systematic review of technology-based lifestyle interventions piloted among childhood and TYACS found only six interventions that were delivered via digital mediums such as websites, mobile apps, emails, text messages, or games consoles, highlighting the paucity of the research within this area. 35 These intervention studies were generally found to be effective in promoting behavior change and were well accepted by young people with cancer. Increasingly, digital platforms of information delivery are being acknowledged as effective strategies to reach and engage young people with cancer 35 given the wide age range, geographical dispersion, and multiple competing demands (e.g., school, university, work) of the TYACS population. 20
Our finding that TYACS are interested in health behavior information throughout the cancer care pathway from diagnosis to survivorship strengthens the rationale for developing easily accessible, readily available, health behavior information resources for young people with cancer. However, it remains to be explored whether the precise moment at which a young person with cancer would be most receptive to health behavior information (i.e., the teachable moment) is related to current age, age at diagnosis, or treatment status. We were unable to find any association between these factors and interest in health behavior information, suggesting that the “teachable moment” for health promotion among TYACS may be governed by intra-individual factors. Even so, there is some evidence that health behavior interventions delivered to TYACS may be most effective in preventing the onset and development of health problems if delivered during treatment and in the early stages of survivorship care before the onset of treatment-related comorbidities or noted declines in health behavior. 36 Early introductions to health promotion efforts may trigger behavior change among some TYACS and prime intentions to change behavior among those who are not ready or unreceptive toward lifestyle change.37,38
This study highlights a number of key factors that should be considered when developing health promotion interventions for TYACS. It provides a useful insight into TYACS' past experience of, and overall interest in, receiving health behavior information. This study also presents some of the first data on how and when such information should be provided to young people with cancer. However, these results should be considered in light of several limitations. First, due to the nature of recruitment, it is not possible to gather data on nonresponders or use data submitted by TYACS who completed only small parts of the survey. Second, akin to the majority of existing health behavior interventions,20,35 and studies investigating the psychosocial support needs of TYACS,8,20 the sample within this study was predominantly white and aged between 19 and 25 years. The possibility of response bias within the sample is high, as it is likely that those who responded to the health and lifestyle survey are those who are already engaged in health promotion efforts. As such, coupled with the cross-sectional nature of the study design, our findings may not generalize to the TYACS population as a whole. Moreover, our study only investigated the information needs and preferences of TYACS with regard to physical activity, diet, smoking, and alcohol consumption. Many young people with cancer report a need for information and support on sexual health, fertility, and recreational drug use. Exploration of TYACS' past experience and preference for the timing, delivery, and format of receiving advice on these topics is a much-needed direction for future research.
The results of this study indicate that TYACS are highly interested in physical activity, diet, and weight management advice available in digital-based formats throughout the cancer pathway. It is likely that young people with cancer require additional support from health professionals on sensitive health topics such as smoking and alcohol consumption. Our findings regarding TYACS' preferences on health behavior information are important in informing the development and design of health behavior interventions strategies for young people with cancer and may overcome some of the existing barriers that TYACS face to participating in structured health behavior change programs.39–41
Footnotes
Acknowledgments
This work was supported in part by an IMPACT Award co-funded by University College London and CLIC Sargent awarded to G.P.
Author Disclosure Statement
No competing financial interests exist.