
Abstract
Verrucous carcinoma (VC) is a very rare variant of squamous cell carcinoma of the cervix, difficult to point out in histology because of its benign appearance. We present the case of a 29-year-old woman with a locally advanced cervical VC who underwent radiotherapy followed by radical hysterectomy. After local relapse and despite pelvic exenteration, her condition deteriorated. Treatment of choice in VC is surgery, because of the risk of anaplastic transformation under irradiation, raising the chances of distant spread and converting this rather benign-like type of cancer to an aggressive cancer.
Introduction
V
Case Report
A 29-year-old female patient, with no family or personal tumor-related history, was addressed in April 2016 to the gynecology department for genital hemorrhage, pelvic pain, and dyspareunia lasting for 6 months. Clinical examination found a mass confined to the uterine cervix, and multiple excisional biopsies revealed a well-differentiated VC (Fig. 1).
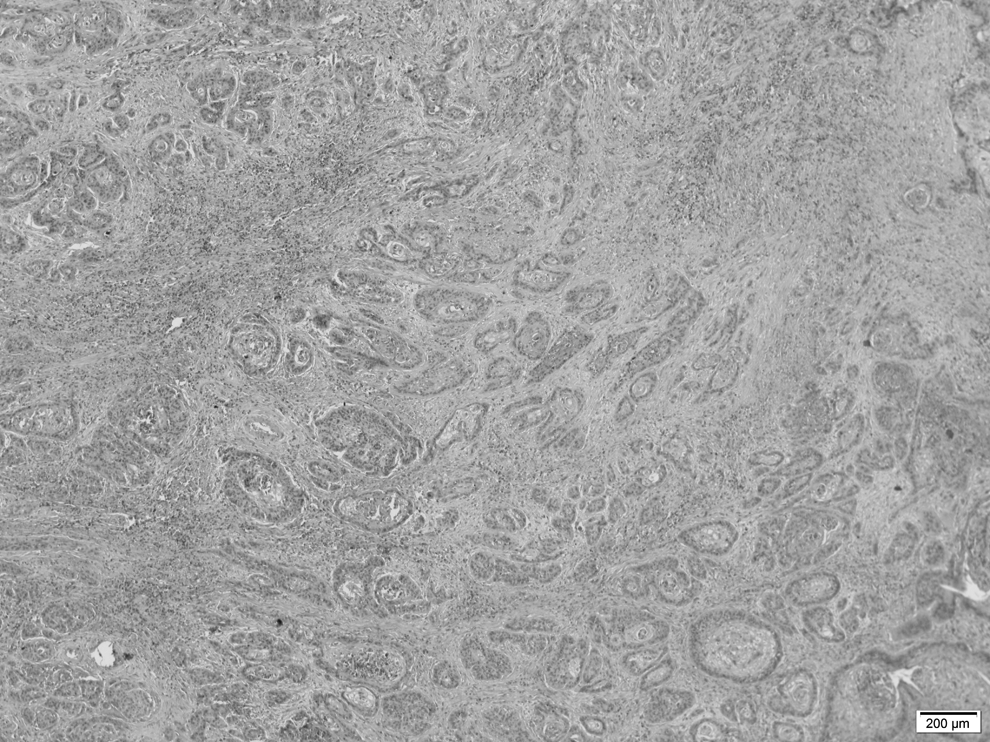
H&E stain showing highly differentiated squamous cell carcinoma with hyperkeratotic, undulating, warty surface that invades the underlying stroma in the form of bulbous epithelial pegs with a pushing border. Tumor cells have abundant cytoplasm and nuclei show minimal atypia.
The abdominal and pelvic magnetic resonance imaging (MRI) showed a 64 × 58 × 57 mm uterine cervical tumor with parametrial invasion, without involving the lower third of the vagina or the urinary bladder and two pathological lymph nodes, obturator right and left of 24 × 15 × 9 and 20 × 12 × 9 mm, respectively, in diameter (Fig. 2).

Axial T2-weighted image reveals a high signal intensity mass confined to cervix, with parametrial invasion and pathological lymph nodes.
The stage of the disease was assessed as IIB according to the seventh edition AJJCC classification and she was referred to the Institute of Oncology to “Prof. Dr. Alexandru Trestioreanu” Bucharest for additional workup and specific treatment initiation. 8 The cystoscopy and rectoscopy complementary performed found no sign of extension through the urinary bladder or the rectal mucosa.
Owing to the extensive tumor, neoadjuvant chemoirradiation was the first therapeutic step recommended. The axial computed tomography (CT) scan for external beam radiotherapy (EBRT), 4 weeks after the MRI examination, found the tumor measuring 79 × 67 mm in diameter.
After 5 days of irradiation and only one infusion of cisplatin for 40 mg/m2, the treatment had to be discontinued for severe pelvic pain and grade 2 gastrointestinal toxicity, expressed by vomiting and dehydration. Radiotherapy was restarted after a 2-week pause and pursued until total dose of 50.4 Gy for 46 days. No concomitant systemic treatment was further provided and no additional brachytherapy was recommended because of the patient's low tolerance.
The patient was later referred to the surgery department and, despite preoperative treatment, the radical hysterectomy resulted in an R1 resection with right parametrial and posterior invasion (Fig. 3). The pathological stage was ypT2bN1, IIIB according to International Federation of Gynecology and Obstetrics (FIGO) staging, without any lymph nodes' capsular rupture, and the histopathological type was a G2 keratinizing squamous cell carcinoma. 9
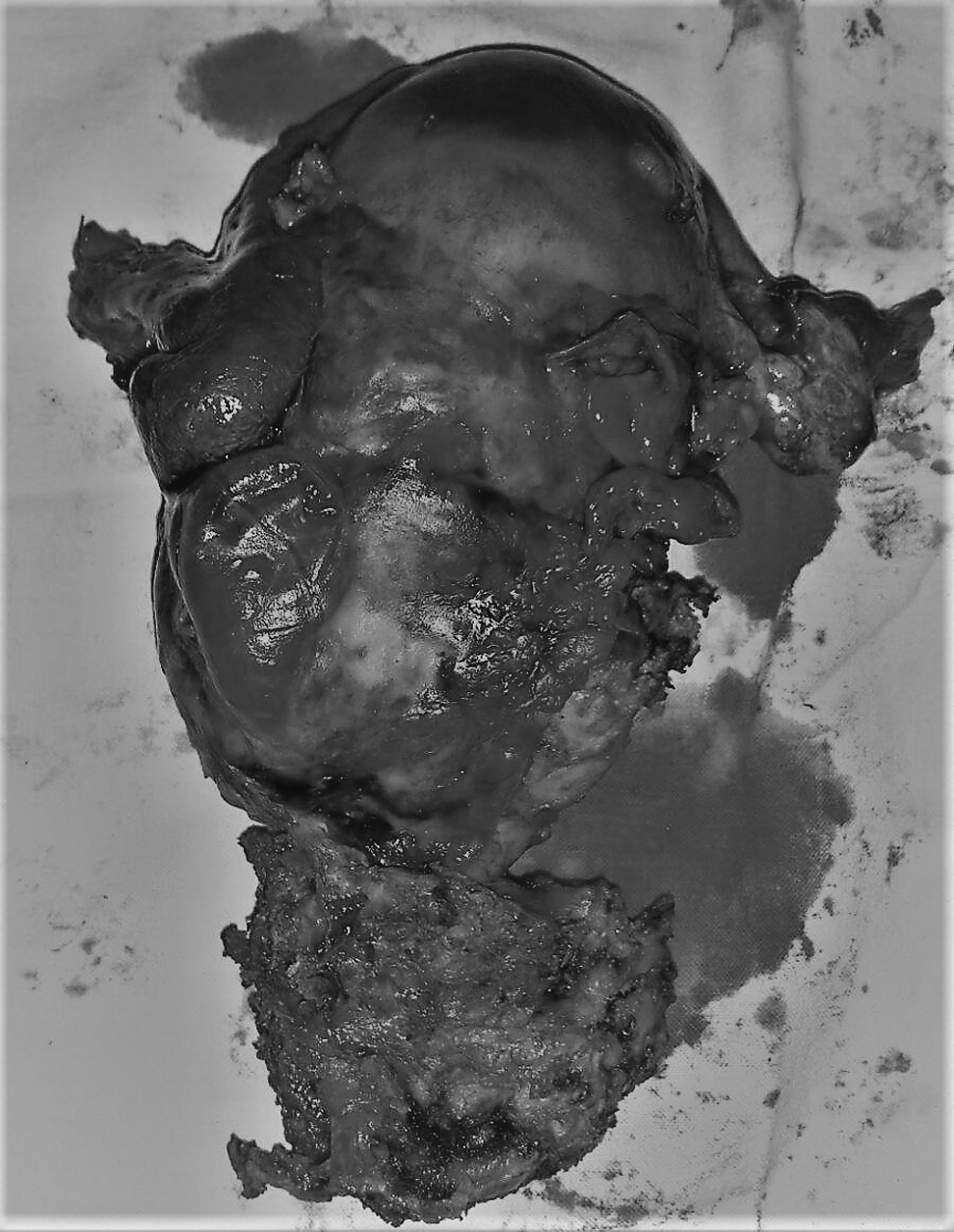
Radical hysterectomy surgical specimen.
After only 2 months since the tumor resection, a follow-up CT scan showed grade II–III bilateral hydronephrosis, lomboaortic adenopathies of 16 × 8 mm in the greatest diameter and dilated small bowel loops. A pelvic exenteration was decided and histopathology examination found a tumoral mass extended to the pelvic wall, involving the bladder, rectum, and appendix, ypT4Nx of keratinizing squamous cell carcinoma. No reirradiation was proposed because the probability of high toxicities and risk of fistula. Two weeks after surgery, the patient called to the hospital for grade III fatigue, dyspnea, and anorexia.
A CT scan reassessment showed pleural and peritoneal effusions and multiple pulmonary secondary lesions. After 1 week of supportive treatment, due to the lack of improvement, the patient was referred to a palliative care center. Considering Eastern Cooperative Oncology Group three performance status, any oncological active treatment was prohibited.
Discussions
In cervical VC, which represents less than 1% of the uterine cervical malignancies, multiple clinical, histological, and treatment-related factors predict the survival rate; disease-free survival exceeding 4 years in isolated cases has been described in the literature.1,5,7
VC is characterized by a densely keratinized outer layer covering a papillomatous tumor, composed of well-differentiated squamous epithelial cells pushing the adjacent stroma rather than invading it, unlike squamous cell carcinoma that is much more infiltrating in the basal layer. 10 This benign histological appearance and similarity with epithelial hyperplasia make the superficial biopsy insufficient for the diagnosis and lead to misdiagnosis.2,6
In a small series of patients with VC receiving radiotherapy, anaplastic transformation was observed at an interval ranging between 2 and 8 months after therapy completion in ∼30% of patients. In most of the cases, the transformation was announced by a rapid enlargement of the tumor, and in patients without anaplastic transformation, recurrent disease occurred after irradiation.1,7,11 An accurate reassessment of pathological specimens of a large number of VCs of the oral cavity exposed to irradiation has found anaplastic transformation in only 7% of the cases. 12
In our case, the primary biopsy showed VC, but the histology result after the first and second surgeries was in favor of an invasive carcinoma that might be explained by the initial coexistence of the two entities in the same tumor. Dedifferentiation to a more aggressive form or the development of anaplastic disease could be an explanation for the postradiotherapy fulminant evolution with local invasion and metastasis.2,7,13
Type III radical hysterectomy, perfected by Meigs, consisting in large parametrial excision, uterosacral, and cardinal ligaments removal as close to their insertion as possible, along with the upper half of the vagina and routine pelvic lymphadenectomy, is considered the elective surgical treatment for patients with FIGO stage IA2-IIA cervical cancer.14,15 It can also be suggested in cases beyond stage IIA, for example, if radiochemotherapy is not available or in specific histologies like VC even in large tumor burden. 16 In one review of 35 cases of cervical VC reported until 1999, the cure rate for surgery was 50% versus 38% for radiotherapy. 17
Considering the proximity of the tumor to vascular and nervous structures, radiochemotherapy was the initial treatment option decided by the oncology tumor board, considering the current standard of care (SOC) in cervical cancer. 18 Despite a total dose of 50.4 Gy EBRT administered, local response was disappointing, according to the posthysterectomy pathology report. Even after neoadjuvant treatment, an R0 resection was not technically possible because of the invasion of the rectum and obturator fossa. Although the rectum wall was partially resected, the tumor was adherent both to the right obturator nerve and to the artery, resulting in a suboptimal intervention. The possibility for total/posterior pelvic exenteration was not taken into consideration and the patient did not give her consent for this type of intervention, as the initial staging was IIB with no signs of invasion at cystoscopy or rectoscopy. Adjuvant brachytherapy was proposed, but the patient did not tolerate this procedure.
Total pelvic exenteration, which represents en bloc resection of the pelvic organs, bladder and rectum included, with external derivation of urinary and digestive conducts first developed with palliative intent for advanced pelvic tumors and gradually shifted to curative purposes either in primary invasive tumors or in recurrences. As in all extensive procedures, the reported rate of complications and morbidity reached up to 70%, but with the advances of new surgical techniques and postoperative management, intraoperative death rates decreased from 21% to close to 0, whereas 5-year survival rates increased from 20% to 73%.19–21
In our patient, we had to proceed to ultraradical surgery because the response to radiochemotherapy was poor; the resection after classical hysterectomy was with the microscopic invasion of the margins and the histological type was a mainly surgical one.
After the pelvic exenteration, the patient progressed very soon to systemic disease. Because of the patients' frail condition, it was decided upon no systemic treatment. There is no evidence-based option for the treatment of metastatic VC of the cervix, and guidelines for recurrent and metastatic cervical cancer should be followed. 8 An option would have been platinum-based chemotherapy with paclitaxel or topotecan if the status permitted.22,23
Chronic pelvic pain was the main complaint in our patient. It was immediately exacerbated by radiotherapy and was not attributable to any infectious or inflammatory causes. Pain control was poor even under level III opioids and coanalgesics and persisted after pelvic exenteration. Literature data regarding causes of pelvic pain in similar cases are scarce. Recurrent pain after exenteration makes its cause a dilemma; a hypothesis could be the involvement of the inferior hypogastric plexus. 24 The direct invasion of the plexus was not described in any of the surgery protocols cited here.
Conclusions
Based on case reports, the recommended first choice treatment in locally advanced VCs is surgery as far as that is feasible. It is difficult to establish an SOC based only on isolated cases and small case series, and the guideline of treatment based on the main histological type has to be applied.
Anaplastic transformation after irradiation in a verrucous subtype of squamous cervical carcinoma might be an explanation for the distant metastasis fulminant evolution, difficult to identify histologically; R1 resection and verrucous natural history have already created the premises of local recurrences.
Reporting cases of rare tumors provides support for an international database and helps to draw specific SOCs.
Footnotes
Author Disclosure Statement
The authors declare their responsibility for the content of this publication. All authors contributed to the conception and content of the article and approved the final version as well as for submission. No competing financial interests exist.