
Abstract
Background:
The increased incidence of physical and psychosocial adverse health outcomes (AHOs) in childhood lymphoma survivors (CLSs) is well known, but these AHOs' association with self-reported general health is rarely described.
Aim:
We explored this association among long-term CLSs.
Methods:
In 124 CLSs (Hodgkin: 81; non-Hodgkin: 43; median age: 33 years), physical AHOs were graded based on slightly modified common toxicity criteria for adverse effects (CTCAE)-4 recommendations (Grade 0–3). Psychosocial AHOs (pain, work inability, fatigue, and mental distress) were mainly assessed by validated patient-reported questionnaires (Grade 0–2). The results were related to contemporary self-reported general health. Statistical significance: p < 0.01.
Results:
At least one physical AHO was found in 120 CLSs, being of Grades 1, 2, and 3, respectively, in 43, 43, and 34 survivors. The prevalence of psychosocial AHOs (Grades 1 or 2) was 63%, being Grade 2 in 62 CLSs. The CLSs described their general health as significantly reduced compared with controls, with the greatest reduction for survivors in whom physical AHOs were combined with moderate to severe psychosocial AHOs.
Conclusion:
Psychosocial more than physical AHOs impact on CLSs' current self-reported general health. Clinicians responsible for follow-up of CLSs should be aware of the strong reduction of contemporary general health by Grade 2 psychosocial AHOs. The study challenges the use of the physician-assessed CTCAE-4 categories in long-term cancer survivors and emphasizes the need to develop instruments, which reflect both physical and psychosocial AHOs in these individuals.
Introduction
S
Studies on AHOs in childhood cancer survivors have often focused on physical AHOs1–3,8,9 or have dealt with psychological or psychosocial issues such as fatigue, mental health, and quality of life10,11 although less is known about the combination of these AHOs and their association with contemporary general health. Furthermore, severity grading of the physical AHOs has in the largest studies been based on the physician-based common toxicity criteria for adverse effects (CTCAE),5–7 with limited consideration of the survivor's own perception of his/her AHOs. Finally, although childhood cancer survivors more often describe their general health as “poor” or “fair” 12 than their siblings, little is known about the association between the severity of AHOs and the current general health as perceived by childhood cancer survivors.
In 2007–2011, a cross-sectional survey was performed among Norwegian adult CLSs.8–11 The overall aim of this survey was to gain expanded knowledge on type, prevalence, and severity of selected physical and psychosocial post-treatment AHOs among the survivors. Previous reports from the study have dealt with cardiac sequelae, gonadal function, fatigue, and quality of life.8–11 In the present study, we assessed these survivors' contemporary self-reported general health compared with the general health in a control group from the general population and explored the association between different types and levels of AHOs and self-reported general health.
Materials and Methods
Patients and study design
The present report utilizes data from the aforementioned survey among Norwegian CLSs focusing on history and detection of physical and psychosocial AHOs.8–11 All survivors had been identified through the Cancer Registry of Norway. Survivors eligible for the survey were treated for non-Hodgkin lymphoma (NHL) or Hodgkin lymphoma (HL) between 1970 and 2000, aged ≤18 years at diagnosis. The HL survivors had been treated at one of the four University Hospitals in Norway, while included NHL survivors had been treated at Oslo University Hospital serving one of Norway's four health regions and covering about 50% of Norway's inhabitants. The sample is viewed as being representative for Norwegian survivors of HL and NHL treated from 1970 to 2000.
The survey consisted of completion of a mailed questionnaire and a 2-day out-patient examination at Oslo University Hospital. Of 220 invited CLSs, 140 returned the questionnaire, and 127 CLSs participated in the 2-day survey. The present study includes those 124 CLSs who completed the questionnaire and underwent a clinical examination supplemented by blood test, cardiological, and ophthalmological tests as well as bone mineral densitometry. However, not all CLSs participated in all supplementary specialized examinations.
Due to different treatment strategies used from 1970 to 2000, treatment data in the current analysis were broadly classified as “chemotherapy only,” “radiotherapy only,” or “chemotherapy & radiotherapy,” with more detailed specification of the therapeutic regimens as reported previously. 9 Ten patients had undergone stem cell transplantation. Five of them had total body irradiation, and five had combination chemotherapy (carmustine, etoposide, cytarabine, and melphalan) as their conditioning regimen. The observation time was defined as the interval between the date of diagnosis and the date of the outpatient examination and was dichotomized by its median of 20 years. Median age at survey was 33 years, this figure also represents the cutoff value for dichotomization of this age variable.
Patient-reported general health, being the principal outcome of the current study, was assessed by the first item of Medical Outcome Study short form-36 (SF-36). 13 Responding CLSs categorized their general health as “Excellent,” “Very good,” “Good,” “Fair,” or “Poor.” These responses were in a first step dichotomized as follows: the combined first three categories represented “Good” general health, whereas the responses “Fair” and “Poor” reflected “reduced” general health. Following published guidelines, each response was in a second step transformed to a scale ranging from 0 (worst) to 100 (best). 13 Use of mean sum score for all CLSs (“SF36GenHealth”) enabled intergroup comparisons within the CLSs and comparison with the mean sum score of 478 individuals from the Norwegian general population, aged 30–39 years (Controls). 14
Grading of the physical AHOs was based on CTCAE (version 4.0) whenever possible, although with slight modifications discussed with a committee consisting of experienced medical oncologists. Asymptomatic patients without any physician-detected AHOs were allocated to Grade 0. Grade 1 physical AHOs (“mild,” intervention not indicated) covered pathological findings based on blood tests and investigations in patients without or with mild symptoms but no need for interventions. AHOs treated by any medications in mildly or moderately symptomatic CLSs were graded as Grade 2 (“moderate”). AHOs compatible to Grade 3 identified medically significant severe physical AHOs, which, however, were not immediately life-threatening. No Grade 4 physical AHOs (life-threatening, immediate intervention required) were diagnosed during the survey. The CLSs were finally allocated to one of three subgroups separating subjects with physical Grades 1, 2, or 3.
Psychosocial AHOs were assessed by the survivor's completion of validated instruments as the Hospital Anxiety and Depression Scale (HADS) 15 and the Fatigue Questionnaire, 16 the operalization of the responses following published guidelines. Scoring ≥19 point on the HADS questionnaire indicated clinically relevant mental distress, not separating depression from anxiety. 15 Substantial fatigue with duration for at least 6 months reflected chronic fatigue. 16 The CLSs reported their participation in work life and the use of analgesics and psychopharmaca.
Grade 2 psychosocial AHOs included chronic fatigue, 16 regular use of analgesics or psychopharmaca for more than 3 months during the preceding year, receiving disability pension, being on sick leave for more than 1 year (“work inability”), or scoring ≥19 on HADS. 15 Grade 1 psychosocial AHOs covered minor psychosocial problems, short-lasting sick leave, or irregular use of analgesics or psychopharmaca. Grade 0 indicated the absence of any report on psychosocial problems.
Statistics
Dependent on the distribution of the variables, descriptive statistics included calculation of means ± standard deviations, medians (range), or calculations of proportions. Intergroup differences of SF36GenHealth were evaluated by t-tests. A difference of 5 points of SF36GenHealth was considered as “Clinically significant.” 13 Four patients, all presenting with Grade 3 physical AHOs and Grade 2 psychosocial AHOs did not respond to the question about general health. Their missing values were substituted by the mean SF36GenHealth sum score obtained from 23 survivors who reported Grade 3 physical and Grade 2 psychosocial AHOs.
Chi-square tests evaluated the differences between proportions. A logistic multivariate regression analysis evaluated the associations between the dichotomized general health variables (good vs. reduced) and variables significant in the bivariate analysis. The level of statistical significance was set at p < 0.01. Analyses were performed by the SPSS software for PC, version 20 (SPSS, Inc., Chicago, IL).
The study was approved by the Regional Ethical Committee of the southeast health region in Norway (no. 2009/926).
Results
Childhood lymphoma survivors
Of our 124 CLSs, 81 had been treated for HL and 43 for NHL. They participated in the survey after a median of 20 years and with a median age of 33 years. Thirty-eight CLSs (31%) had chemotherapy only (Table 1). In 72 patients (58%), the treatment had consisted of both chemotherapy and radiotherapy, and 14 patients had had radiotherapy as their only therapy (12%).
NHL, non-Hodgkin lymphoma; HL, Hodgkin lymphoma.
Only four patients had no physical AHOs, and 46 (37%) did not report any psychosocial AHOs (Table 2). Based on our definitions, most patients presented with multiple AHOs. In 43 patients (35%), the physical AHOs were restricted to Grade 1, including seven patients with at least four different AHOs in each of them. Another 43 CLSs presented with at least one Grade 2 physical AHO combined with or without Grade 1 AHOs, including three patients with more than three physical Grade 2 AHOs. Grade 3 physical AHOs were described in 34 CLSs (27%), being multiple in only three of them. Multiple Grade 2 psychosocial AHOs emerged among 27 of 62 CLSs, whereas for 15 of 16 CLSs, only one Grade 1 psychosocial AHO was documented.
Without Grades 2 or 3.
With or without Grade 1, but without Grade 3.
With or without Grades 1/2.
AHOs, adverse health outcomes.
Adverse health outcomes
Altogether, 244 Grade 1, 89 Grade 2, and 37 Grade 3 physical AHOs were observed (Tables 3 and 4). The most frequent physical AHO was hypertension (n:91), scored as Grade 1 in 70 CLS. In 45 of 100 evaluable patients, reduced lung function was diagnosed by spirometry only, 32 of them being Grade 1 in asymptomatic patients. In 41 survivors, asymptomatic cardiovascular disease Grade 1 was diagnosed, and 12 and 6 CLSs were allocated to Grades 2 and 3 cardiac AHOs, respectively.
CTCAE-4 criteria.
CTCAE-4 criteria with slight modification based on consensus among experienced clinicians.
Males: <25% of expected, females: <27% of expected.
BCC, basal cell carcinoma; BMI, body mass index; BNP, brain natriuretic peptide; BP, blood pressure; DLCO, diffusion capacity of the lung for carbon monoxide (CO); EF, ejection fraction; FSH, follicle-stimulating hormone; FT4, free thyroxine; LH, luteinizing hormone; SF, shortening fraction; TLC, total lung capacity; TSH, thyroid-stimulating hormone.
HADS, Hospital Anxiety and Depression Scale.
Fourteen of 37 Grade 3 AHOs represented gonadal toxicities (undesired childlessness [n:11] and premature menopause [n:3]). Fifty-four CLSs had Grade 1 hypothyroidism (n:22), and 32 survivors used thyroid medication (Grade 2). The seven events solid cancers included, classified as Grade 3 physical AHOs, were breast cancer (n:2), thyroid cancer (n:2), anal cancer (n:1), osteosarcoma (n:1), and prostate cancer (n:1) in three patients combined with baso-cellular skin cancer. Additional four patients were diagnosed with baso-cellular skin cancer without any other malignancy. Chronic fatigue (n:38) and mental distress (n:41) were the most frequent Grade 2 psychosocial AHOs.
General health
Sixty-nine percent and 31% of the CLSs reported good or reduced general health, respectively. In bivariate analyses, prior radiotherapy with or without chemotherapy significantly worsened CLSs' self-reported general health (p < 0.01; Table 5). Increasing grading of physical AHOs or the presence of at least one Grade 2 psychosocial AHO resulted in increased numbers of CLSs with Fair or Poor general health. Having been treated for HL or being older than 33 years at the survey correlated nonsignificantly with reduced general health.
Chi-square test.
Six patients had radiotherapy only.
In the logistic multivariate analysis, including physical AHOs, treatment and psychosocial AHOs, only the latter factor remained significantly associated with reduced general health (p < 0.001). A nonsignificant association emerged between the presence of Grades 2 and 3 physical AHOs and reduced general health (p: 0.05).
Among all 124 CLSs, the mean sum score SF36GenHealth was 59 ± 21.3 compared with 81 ± 19.5 in the controls (Fig. 1). Among CLSs with physical AHOs but without Grade 2 psychosocial AHOs (n:20 + 23 + 11), the mean SF36GenHealth sum score was 70 ± 17.6, decreasing to 47 ± 19.6 in survivors with physical and Grade 2 psychosocial AHOs (n:19 + 20 + 23; data not shown). The differences between the mean sum scores of SF36GenHealth in CLSs with mild, moderate, or severe physical AHOs did not reach the level of clinical significance (>5 points) as long as the survivors did not report additional Grade 2 psychosocial AHOs. CLSs who had Grade 3 physical and Grade 2 psychosocial AHOs had the lowest mean sum score of SF36GenHealth (42 ± 19.0).
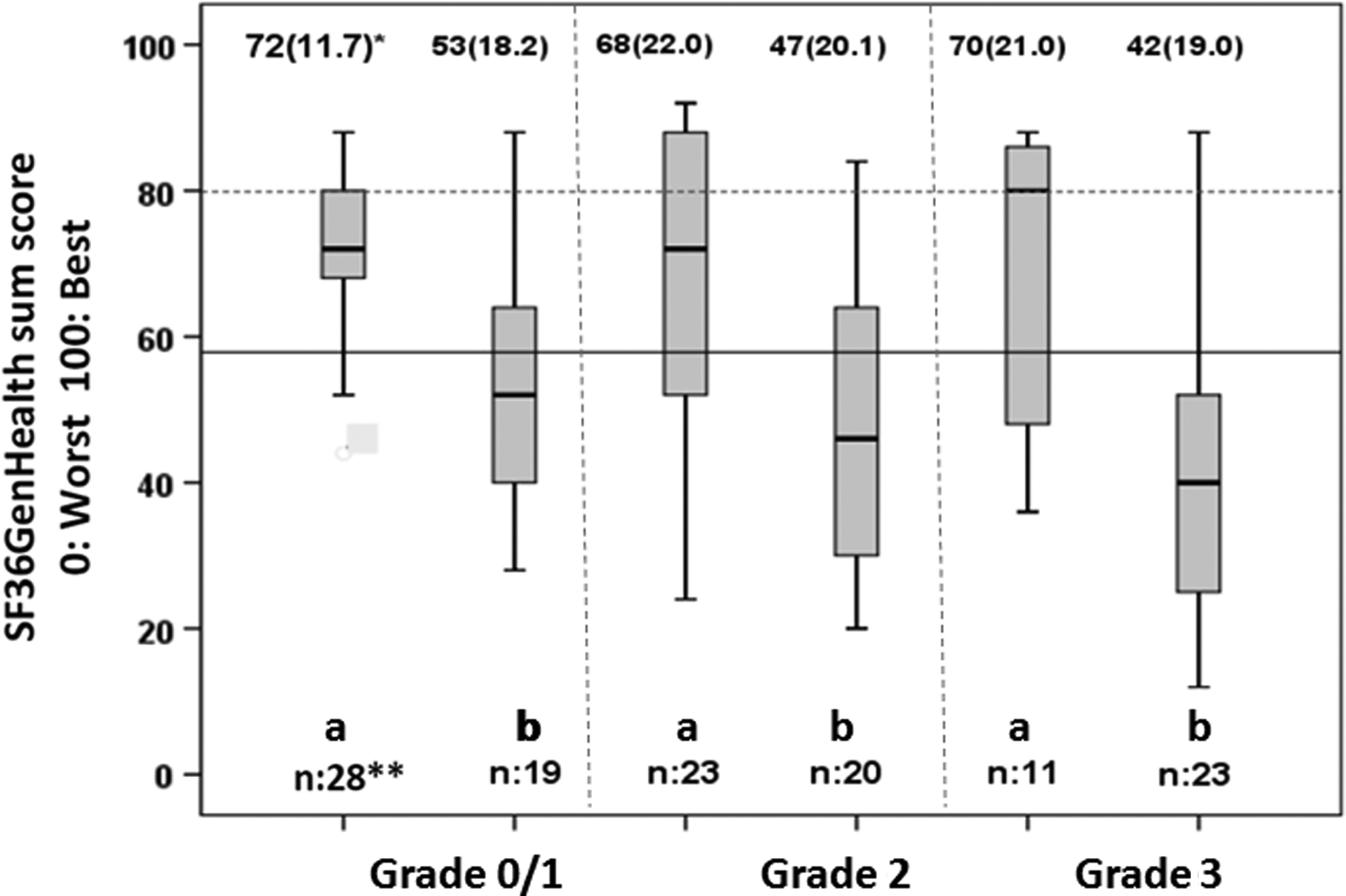
General health (SF36GenHealth) in 124 CLSs and grading of physical AHOs without (a) or with (b) Grade 2 psychosocial AHOs. aGrades 0/1, 2 or 3 physical AHOs without Grade 2 psychosocial AHOs. bGrades 0/1, 2 or 3 physical AHOs combined with Grade 2 psychosocial AHOs. *SF36GenHealth sum score (standard deviation). **Number of CLSs within each group. SF36GenHealth in Controls from the general population (mean sum score: 81). SF36GenHealth in all Childhood Cancer Survivors (mean sum score: 59). AHOs, adverse health outcomes; CLSs, childhood lymphoma survivors.
Discussion
After a median observation time of 20 years 120 of 124 adult CLSs had at least one physical AHO, one third being severe if graded according to slightly modified CTCAE-4 guidelines. Most survivors had multiple physical AHOs. Sixty-two CLSs (50%) reported Grade 2 psychosocial AHOs. One third of the survivors described reduced general health, the reduction confirmed by comparison with controls from the general population. Psychosocial AHOs contributed stronger to reduced self-reported general health than physical AHOs.
The CTCAE-4 criteria were designed to document and to compare the frequency and severity of side effects during and immediately after different cancer treatments, mainly covering physical AHOs. Important psychosocial AHOs as fatigue, reduced work ability or chronic pain are not or only limitedly covered by the CTCAE-4 categories. With this background, our study emphasizes the importance of psychosocial AHOs' negative impact on CLSs' general health, which may be overlooked if the assessment of post-treatment AHOs in long-term cancer survivors is restricted to the CTCAE-4 grading system.
Using the CTCAE-4 system, all recording and grading of AHOs are based on healthcare professionals' observations. On the contrary, severity grading of physical AHOs seemed to differ between CLSs and healthcare professionals, as nonsignificant differences of SF36GenHealth emerged when AHOs of Grades 1, 2, and 3 observed in our study were compared with each other. Recently, Hudson et al. discussed similar shortcomings of the CTCAE-4 system, if applied in long-term cancer survivors, and proposed modifications to be used in clinical research among long-term cancer survivors. 17 Indeed, there is increasing recognition that CTCAE-4 criteria do not or only insufficiently take into account the cancer survivors' own perception of their current general health.18,19 The ongoing attempts to design patient-reported CTCAE criteria meet this insufficiency by letting the patients themselves score the presence and severity of AHOs.20,21
Our admittedly small-sized study supports the above attempts as it documents the limitations of CTCAE-4 grading when investigators aim to describe the patient-perceived comprehensive burden of post-treatment AHOs in long-term cancer survivors. However, researchers should be aware that both under- and over-reporting may represent problems when physician-based records on late effects are compared with patient-reported experience.22,23 We support Hudson et al.'s findings of decreased general health in childhood cancer survivors, siblings representing their control group. 12 The 22 points difference of SF36GenHealth between CLSs and our controls reflects considerable clinical significance. Our further interest is of the observation that the difference observed for all survivors and CLSs with physical AHOs only is 11 points, in contrast to 22 points, comparing all CLS with those whose physical AHOs are combined with Grade 2 psychosocial AHOs. Clinicians should thus be aware that self-reported general health is strongly threatened by major psychosocial AHOs (fatigue, mental distress, and reduced work ability). Our findings also indicate that future long-term surveys in childhood cancer survivors, which aim to document the overall burden of AHOs on general health, should report on the frequency and impact of both physical AHOs and the individuals' experience of psychosocial adverse outcomes, the latter being assessed by validated questionnaires.
As also shown by other investigators,5–7 the great majority of our CLSs reported multiple physical AHOs. The high proportion of Grade 1 hypertension should, however, be viewed with caution as “office hypertension” during the 2 days of survey cannot be excluded.
The high percentage of hypertensive CLSs must also be seen on the background that Grade 1 hypertension according to the CTCAE-4 criteria implies a systolic or diastolic blood pressure of ≥80 or ≥120 mmHg, respectively. The prevalence of cardiac dysfunction, second cancer, gonadal toxicity, and thyroid hypofunction in our CLSs compares well with published observations.1–3,24 Long-term symptomatic pulmonary dysfunction requiring treatment was observed in only 13% of the evaluated CLSs, despite mediastinal radiotherapy and/or use of Bleomycin in the majority of the HL survivors. Decreased bone mineral density was a minor problem in this young cohort, but may become a problem with increasing age, not at least on the background of possible premature gonadal hypofunction. 24
Due to the magnitude of AHOs in childhood cancer survivors, guidelines for regular medical follow-up examinations have been established. 25 However, only half of the survivors comply with the recommended examinations. 26 One reason may be that many childhood cancer survivors, as long as they are asymptomatic, are not sufficiently aware of risk factors, comparable to Grade 1 AHOs. They perceive their health as good and relatively unaffected by their previous treatment, not necessitating contact with the healthcare service. Such survivors will probably need particularly designed information by healthcare professionals to increase their motivation to attend recommended health examinations, which should address both physical and psychosocial AHOs.
The relatively small number of CLSs is an obvious limitation of our study. Only 50% of the invited CLS participated in the original survey,9,10 and the Ethical Committee did not allow us to explore the reasons for nonparticipation. Furthermore, the grading of the psychosocial AHOs was based on ad hoc definitions of a consensus group although many of the survivors' responses were obtained by validated questionnaires. The availability of both patient-reported outcomes and results from clinical examinations is viewed as a strength as is the use of validated measures (CTCAE-4, HADS, and Fatigue questionnaire).
Conclusion
Adult long-term survivors after childhood malignant lymphoma experience their general health significantly reduced compared with that of comparable individuals from the general population. Psychosocial more than physical AHOs are associated with contemporary reduced general health, the reduction being greatest in survivors reporting both types of AHOs. The current Common Toxicity Criteria grading system insufficiently reflects the survivors' experience of their general health, thus indicating a need for development of instruments, which better reflect the cancer survivors' entire health situation.
Footnotes
Acknowledgment
The financial support by the Research Foundation of the Norwegian Radium Hospital is acknowledged.
Disclaimer
This study was presented on a poster discussion held during ECCO 17, Amsterdam, The Netherlands, January 28–30, 2017.
Author Disclosure Statement
No competing financial interests exist.