
Abstract
Purpose:
We evaluated the satisfaction of adult survivors of childhood cancers and their general practitioners (GP) after a long-term consultation.
Methods:
The first Long-term Follow-up Study in Oncology (SALTO1) is a prospective cohort study of survivors of childhood cancers (except leukemia) diagnosed between 1987 and 1992 in the Rhône-Alpes and Auvergne regions of France. Of the 481 patients eligible for the study, 150 participated in a long-term consultation with a pediatric oncologist and an internist, after which survivors and their GPs received long-term plans and recommendations based on consultation findings. A year after the consultation, survivors and their GPs assessed their satisfaction with the process.
Results:
Of the 150 survivor participants in the long-term follow-up, 120 (80%) completed the satisfaction form, with 107 (89%) reporting satisfaction. Forty-eight (32%) expressed strengthening their follow-up as a consequence of the consultation. Of the 79 survivors sent recommendations, 76 (96%) reported reading them, most (n = 68; 86%) found them useful, and 56 (71%) followed recommendations. Of the 107 GPs of the survivors, 82 (77%) conceded having been poorly informed about long-term complications for their patients after chemotherapy, and 93 (88%) appreciated having a hospital contact available for these patients.
Conclusion:
The long-term consultations ultimately enhanced medical follow-up of survivor participants, improving knowledge of both patients and family physicians regarding the patients' early disease, its treatments, and possible concerns, and offering consultative resources of medical specialists. The levels of participation of survivors and their physicians and reported satisfaction encourage the adoption of such consultations throughout France.
Introduction
I
Late effects can include physical issues, such as second primary tumors, secondary leukemia, cardiovascular disease, infertility, growth impairment, and other manifestations, as well as educational, behavioral, and social problems. 2 An estimated 60% of survivors of childhood cancer will have one or more treatment- or disease-related late effects, more than 30% of which will be classified as moderate or severe, and as many as 30% will experience significant psychosocial late effects.3–13
Long-term follow-up is recommended to improve detection of late effects, to inform survivors about their early diagnosis, the treatment they received, and the associated risk for comorbidity, and to develop an appropriate long-term care plan in compliance with findings of this follow-up.
Models of long-term follow-up care for adult CCS have been driven by the patient, general practitioner (GP), nurse, or medical specialist and conducted in either a long-term follow-up clinic or the physician offices.14–18 Two general models have involved either the GP conducting follow-up without sustained contact with a primary cancer treatment center or late-effect clinic (GP only) or the GP working in close collaboration with practitioners in such facilities (shared care). Some authors have proposed that the primary care physician should take over follow-up care once the risk of intermediate-term late effects and cancer recurrence are low. In the shared-care model, the GP cares for the individual, but the pediatric oncologist or long-term follow-up center remains available for consultation. 19 Very close collaboration is essential for survivors with high risk to develop late effects and who might need to visit the cancer center regularly.
We evaluated the level of satisfaction of adult CCS and their GPs with a long-term follow-up consultation process that involved joint consultation of the survivor with a pediatric oncologist and an internist.
Materials and Methods
Population
The population-based childhood cancer registries of the Rhône-Alpes (ARCERRA) and Auvergne regions of France record the type of cancer for each child diagnosed since 1987 according to the norms of the third revision of the International Classification of Childhood Cancer (ICCC-3). 20 Eligibility criteria for adult survivors in our study were: diagnosis of their primary cancer between January 1987 and December 1992, their age less than 15 years at diagnosis and residence in the Rhône-Alpes or Auvergne regions, and their age of at least 18 years on December 31, 2010. We did not include survivors of leukemia in our cohort because another French study has analyzed the long-term follow-up of these cases (LEA Cohort). We also excluded 27 registered cases—8 who died from any cause at some time after the end of their cancer treatment, 8 with borderline tumor after anatopathologic review, 5 not living in the Rhône-Alpes region at diagnosis, 3 living outside France and lost to definitive follow-up, 2 with severe neurologic deficit, and 1 who appeared as a duplicate entry in the registry. Patients were considered lost to follow-up whose vital status was unknown after checking with the National Directory of Identification of Individuals (Répertoire National d'Identification des Personnes Physiques [RNIPP]) maintained by the National Institute of Statistics and Economic Studies (INSEE) or whose address was unknown at the time of the study.
Methods and evaluation
We sent each eligible adult CCS a letter requesting their participation in this first Long-term Follow-up Study in Oncology (Suivi A Long Terme en Oncologie [SALTO1]) followed by a letter of reminder 1 month later if they did not respond to the initial correspondence. Those who responded and agreed to participate (respondents) were asked to complete a baseline questionnaire that asked them to describe their general situation, socio-professional status, physical health, and quality of life. After completing the form, respondents consulted with a pediatric oncologist and an internist who explained to the patient the disease that affected him during childhood and the treatment he received, including the main drugs used in the case of chemotherapy, type of surgery performed, and type of radiotherapy (RT) delivered, as applicable, and the risk of potential late effects of the treatment given.
Additional tests were scheduled after their consultation according to their clinical findings and recommendations made after chemotherapy and/or RT.1,21 Based on the findings of these consultations, participants were given cards delineating specific recommendations along with advice for prevention of complications and for scheduling follow-up evaluation/s. Sample cards may be seen on the website of the French Society of Cancers of Children and Adolescents. 22
Survivor respondents and their GPs were sent summaries of the SALTO1 consultation and about one year later, a form to assess their satisfaction with the long-term consultation process by using an analogue scale. Survivors responded to nine questions (Fig. 1), and GPs assessed five areas (Fig. 2). In addition, a medical doctor followed up by telephone with GPs who did not respond to the initial form.

Survey of satisfaction of adult survivors of childhood cancers who participated in the first Long-term Follow-up Study in Oncology (SALTO1).

Survey of satisfaction of general practitioners of adult survivors of childhood cancers who participated in the first SALTO1.
Statistical analysis
Data were computerized by using EpiData software (EpiData, version 3.1, The EpiData Association, Odense, Denmark) and analyzed with SAS software (SAS, version 9.2, SAS Institute, Inc., Cary, North Carolina).
Scores from the 8 questions of the survey regarding the patients'expectations were calculated from 0 (not satisfied) to 100 (very satisfied).
To analyze the characteristics of the populations and results of the self-administered questionnaire and satisfaction survey, we used Chi-square test or Fisher's exact test for qualitative data and Student's t-test for quantitative data.
Results
Characteristics of the sample
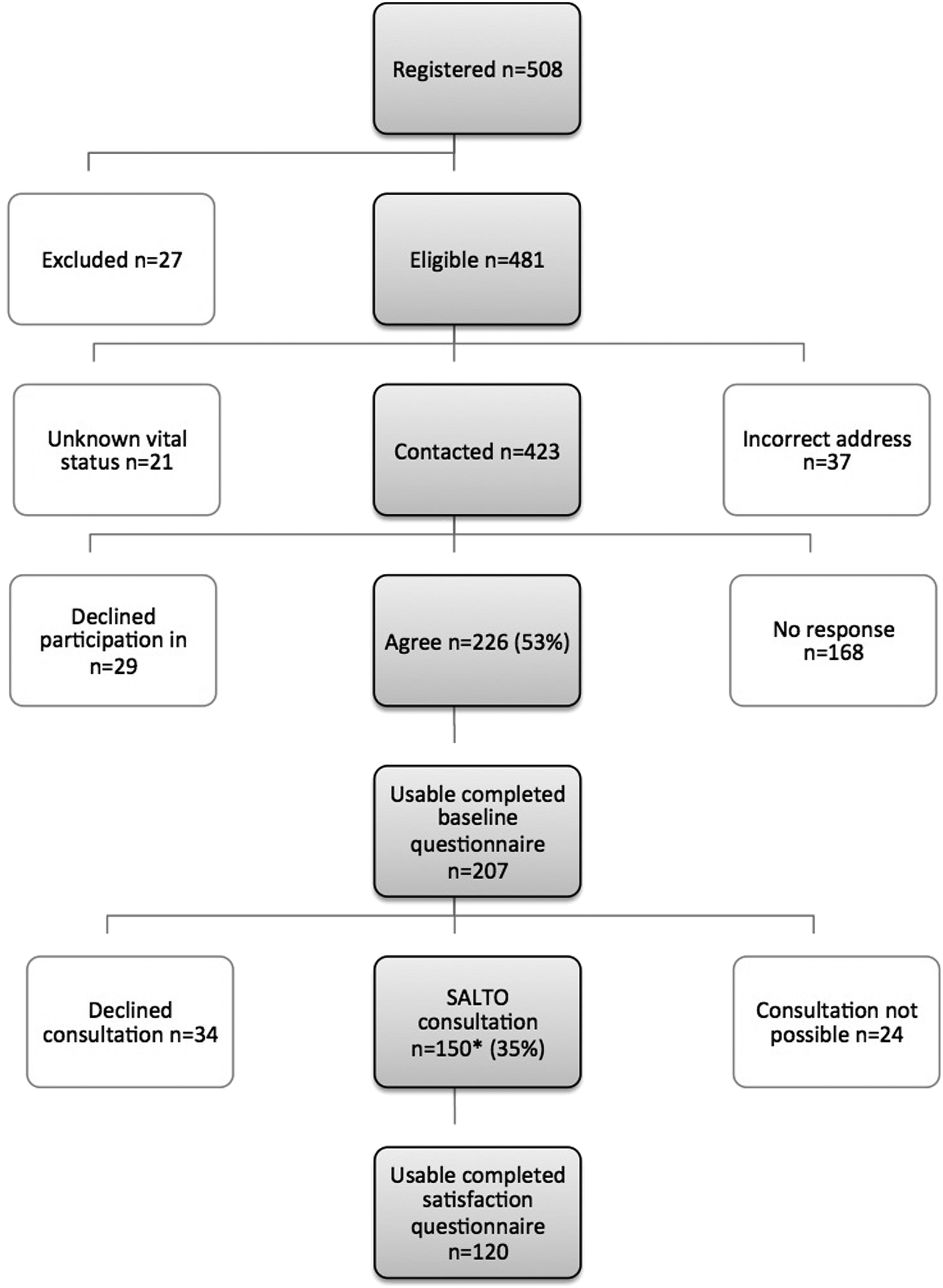
As of June 30, 2013, 58 of the 481 adult CCS eligible for the study (12.3%) were lost to follow-up, including 21 whose vital status was unknown according to the RNIPP and 37 whose correct address was unknown. We were finally able to contact 423 survivors; 168 did not respond to the first letter, and 29 chose not to participate. Two hundred seven of the 226 CCS who agreed to participate responded to the initial questionnaire to ascertain their general status. One hundred twenty of 150 survivors (response rate 80%) who came to the long-term follow-up consultations completed the satisfaction survey (Fig. 3). One survivor of a cerebral tumor with resultant moderate mental difficulties participated in the consultation but did not respond to the satisfaction form.

Flow chart of survivor participation in the first SALTO1.
Age at consultation, age at diagnosis, and type of cancer did not differ between participants and nonparticipants in the SALTO1 study, but gender and treatment received did (Table 1). Most survivors of hepatic tumors (85.7%) came to the consultations, but only 15% of survivors of retinoblastoma came. Twenty-five percent of those treated by surgery alone attended the consultation, and 54% who received at least radiation therapy participated in the survey.
Timepoint: June 30, 2013.
CSRT, Cranial and/or spinal radiotherapy; CT, chemotherapy; NS, not significant; TBI, total body irradiation.
No factor significantly influenced patient participation in completing the satisfaction form (Table 2). GP response varied as a function of their patient's diagnosis (more response for bone and soft tissue sarcoma tumors; p = 0.03) and therapy (more response if survivor received RT; p = 0.01).
GP, general practitioner.
Patient satisfaction
The vast majority (n = 107) (89%) of survivors who participated reported satisfaction with the consultation, and most participants (51%) expressed the desire to participate in a subsequent SALTO consultation (60% after 2 years, 35% after 5 years, and 4% after more than 5 years). However, 28% reported that they would not like to participate again. Regarding the recommendation cards given at the end of the consultation, 96% (n = 76) of the adults who received at least one card reported reading them, most (86%) (n = 68) found them useful, and 71% (n = 56) followed the recommendations. After the SALTO consultation, 32% (n = 48) said that they changed their medical care—half pursuing new regular medical follow-up with a GP, specialist, internist, or psychologist. More than 75% reported changing their lifestyle with respect to physical activity and consumption of food or tobacco. In addition, 76% of the patients recommended that other survivors be given the opportunity to participate in the SALTO consultation.
Gender did not appear to predict satisfaction—the mean satisfaction score for the 116 survivors who responded with a usable form (69 women, 47 men) was 77.7% (±17.9) for each gender (Table 3). However, the type of cancer diagnosis did (p = 0.033)—the mean score was lowest for adults who survived a lymphoma (68.6% ± 21.9%) and highest (87.3% ± 15.3%) for those with soft tissue sarcoma. The type of treatment received also significantly influenced the average score of satisfaction (p = 0.018)—scores were lowest from those who received total body irradiation (TBI) (62.8% ± 43.7%) and highest from those receiving chemotherapy (83.1% ± 14.6%). Multivariate analysis demonstrated a significant individual effect of diagnosis (p = 0.022) and treatment (p = 0.012).
SALTO, Long-term Follow-up Study in Oncology; SD, standard deviation.
No factor affected reported satisfaction regarding questions about the organization or place of conduct of the consultation, but the expression of satisfaction with staff availability differed according to the treatment patients had received—scores were lowest from those treated with craniospinal (76.9% ± 21.0%) or focal (77.0 ± 20.7) RT (p = 0.037).
Satisfaction regarding explanations received about the survivor's cancer and its treatments differed according to the type of cancer diagnosed—scores were lowest for survivors of lymphoma (66.7% ± 22.0%) and highest for survivors of tumors of the central nervous system (86.2% ± 18.9%) (p = 0.025). According to the treatment received, satisfaction was highest for those who had received craniospinal RT (83.3% ± 17.4%) (p = 0.038). Multivariate analysis demonstrated a significant individual effect of the type of cancer diagnosed (p = 0.017) and the type of treatment received (p = 0.026).
The type of treatment received did not influence the level of satisfaction reported by survivors regarding the responses they received during consultation to their own questions about their disease and treatment. Neither did gender, treatment group, or diagnosis affect their reported level of satisfaction with explanations they received regarding secondary prevention via screening programs, which was 69.3% (±26.8) (Table 3).
Survivors who received chemotherapy expressed total satisfaction with the follow-up analyses requested after consultation (83.3% ± 19.8%) (p = 0.03). The rates of satisfaction regarding receipt at home of the patient's medical report were 83.7% ± 20.9% for those who received chemotherapy alone (p = 0.003) and 61.7% ± 30.2% for those who received focal RT.
GP satisfaction
One hundred six of 141 GPs (75%) returned their satisfaction surveys. Most (n = 82) (77%) reported that they were poorly informed about their patients' long-term complications after chemotherapy. More than half (n = 63) (59%) did not know the treatments that their patients had received for their childhood cancers, and 93 (72%) had performed no follow-up evaluations of these patients before the long-term follow-up consultation. Most reported the usefulness of the report of the SALTO consultation (61%), collaborative consultation with a pediatric oncologist/internist (82%), and availability of a hospital contact for this specific population (88%).
Recommendations of the GPs regarding particular follow-up differed significantly according to the diagnosis of the patient—53.9% proposed particular follow-up for those who had had renal tumors, and 95.7% reported making no such recommendation for survivors of lymphomas (p = 0.013).
Discussion
Of the 423 eligible survivors we invited to participate in the SALTO1, 53% (n = 226) accepted and 7% (n = 29) declined the invitation. The others did not respond to our correspondence despite our use of an address known to be correct. The median interval between diagnosis and the time of contact for this study was 21 years, so these subjects had generally not seen their pediatric oncologists for more than 10 years.
Twenty years ago, organized late-effect clinics and transitional care for such patients did not exist as they do today.23–25 When the young patients with cancer reached the age of 18 or were considered cured of their malignancy, the care of most was entrusted to their GPs with or without advice regarding follow-up. At this age when young people are attempting to make important life decisions, such as having children and purchasing a home, these individuals lacked information regarding their previous care and what they might expect in the future to make such decisions with confidence.
Now, survivors are better prepared to plan their future lives and health decisions, equipped with more thorough and accurate information regarding their disease and treatment histories and what they might expect in the future as well as answers to their questions and concerns. Though these follow-up consultations might reveal to them possible unexpected late effects and even cause some anxiety, thus informed, these cancer survivors and their families can better understand and plan for the future and advocate for themselves if and when it might become necessary.
Finally, 150 survivors participated in the long-term follow-up consultations. Participation was low for survivors of retinoblastoma because of the presence of a national center for care and long-term follow-up of such patients at the Institut Curie in Paris, and the rate was highest for survivors of hepatic tumors (mostly hepatoblastomas). In addition, only 54% of subjects who had been treated with extracranial RT took part in the consultation. Given this knowledge, efforts should be made to ensure greater follow-up with this group of survivors.
Long-term follow-up programs exist primarily to provide optimal care for survivors of childhood cancers. The choice of the model of care is important, but each model has advantages and disadvantages. 26 After reviewing various models of follow-up care, Heirs and associates emphasized the usefulness of follow-up in all patients regardless of their perception of its need, 17 recommending further studies to clarify what might be termed an optimal model.
Various studies have revealed discrepancies between survivors' knowledge of their past diseases and the information recorded in their medical records. During our first study, we found an important difference in the number of late effects reported by the survivors themselves and those indicated by physicians in their medical records, 27 and we noted that only one of the eight survivors whose medical records indicated that they had cardiomyopathy reported knowledge that they had this condition. Similarly, Kadan-Lottick et al. indicated that adult survivors of childhood cancers could not necessarily accurately report their disease diagnosis and key treatment exposures compared with findings in medical records: correct diagnosis (72%), any chemotherapy (94%), any radiation therapy (89%), splenectomy (93%), daunorubicine (30%), and doxorubicin (52%). 28 On the other hand, they found that medical records were less likely than patients to report alopecia, a condition that is known to impact the quality of life. Alopecia was reported 13 times by survivors, 3 times by both survivors and pediatric oncologists, and once by medical records alone. The implementation of follow-up consultations such as those we describe can help identify where such inconsistencies do and might arise to improve overall care in the long run.
Primarily because of the organization of transitional care for various chronic pediatric pathologies in our region, we chose to collaborate with medical internists, doctors who are capable of managing patients with a broad range of diseases and of acting as physicans of transitional care between that provided by GPs and organ specialists. Our choice also complied with recommendations of a panel of health policy experts from 2004. 29 Our aim was to organize a global long-term follow-up process shared by a pediatric oncologist, medical internist, and psychologist who would be available to GPs and survivors in the case of unusual symptoms. 26 We also proposed that during these consultations the survivors be instructed regarding their cancers and treatments and provided with cards with recommendations that they could read at home and share with their families or partners to reinforce their understanding of their ongoing care. Some studies have found that both survivors and GPs have valued the shared-care model. A Dutch study showed high survivor (88%) and GP (82%) satisfaction with a shared-care model in which GPs received information from cancer centers regarding patient history, health risks, and necessary follow-up tests. No study has reported the associated involvement of a pediatric oncologist and internist for this transition and long-term follow-up care.
In the past, such communal consultation was useful in responding to weaknesses of long-term follow-up clinics. In the future, giving recommendation cards to the patient with “passports” detailing their chemotherapy, RT, and surgical treatments may be helpful for the survivor and their GP. In most cases, access to this information may be enough for the GP. Nevertheless, long-term follow-up may be inadequate if survivors change their GPs and/or addresses during this transition period. We have also found that some patients between the ages of 18 and 25 are not receptive to explanations of their cancer care and treatment and become interested only later.
Few studies have analyzed the wishes of adults who have been cured of a childhood cancer. Lie's group organized 5 focus groups of adult survivors of childhood lymphoma who had completed routine follow-up care and participated in a preceding follow-up study. 30 Although ambivalent, all survivors wanted information about late effects (symptoms, prevention, and treatment), lifestyle concerns, and their privacy rights. Those authors suggested that information should be tailored, carefully timed, and given in person and in writing. Though many of their patients expressed ambivalence regarding receiving information as adolescents, they perceived this knowledge as essential in case a late effect occurred. A “re-information” consultation about late effects around age 25 was suggested as beneficial. We propose this scheme because the median age of our subjects at the time of consultation was 26. We believe the information made available to these individuals was very useful because 1 year after the consultation, more than 75% reported having changed their lifestyles with respect to physical activity and consumption of food and tobacco.
As well, we consider the completion of the satisfaction survey by 120 of the 150 (80%) participants in the consultation as an indicator of the willingness of these adults cured of a childhood cancer to contribute to the improved follow-up of others like themselves. We observed no significant influence of gender, cancer diagnosed, or type of treatment received on the rate of participation, but a study in the United Kingdom found higher satisfaction with such follow-up among women. 31 However, though not significantly different, participation of our subjects was highest for those who survived tumors of the bone or central nervous system (about 90%), and adults who received TBI during childhood cancer participated fully in this survey. Nevertheless, reported satisfaction was lowest for survivors of lymphoma (68.6%) and highest for survivors of soft tissue sarcoma (87.3%). Satisfaction scores were lowest for those treated with TBI and highest among those who received chemotherapy.
Furthermore, we believe that those survivors who received RT, a treatment known to induce numerous late effects, might have been more likely than those receiving other treatments to want and expect such long-term follow-up consultation from their medical professionals.
The high participation rate of GPs in this study confirms their wish for and appreciation of help with the care of this particular population and corroborates findings of a previous study conducted by Nathan in the United States and Canada. 32
Conclusions
The long-term follow-up consultations we put in place in this study ultimately enhanced the medical follow-up of those survivors who participated. They improved the knowledge of survivors and their family physicians regarding their early disease and treatment and introduced a collaborative link for physicians for consultation with specialist caregivers. The high levels of participation by survivors and their physicians and their reported satisfaction with this follow-up process encourage the adoption of such consultations throughout the country.
We propose in the future to have at least one common consultation of the pediatric oncologist with an adult internist to organize the survivor's transition to adult heathcare and to establish a regular schedule for follow-up by an internist for survivors at high risk for late effects.
Footnotes
Acknowledgment
The authors express their sincere thanks to all the survivors who participated in this study and their families; the French National Cancer Institute (INCA) for financial support; Professor Fernand Freycon, ex-president of ARCERRA, for helpful advice; Rosalyn Uhrig for editorial assistance in the preparation of this article; Audrey Loubier for help in entering data; Professors Dominique Plantaz, Jean-Louis Stephan, and François Demeocq; Drs. Justyna Kanold, Corinne Armari-Alla, Anne Pagnier, Didier Frappaz, Perrine Marec-Berard, Safia Khenifer, Catherine Le Quang, and Sandrine Thouvenin-Doulet; and Françoise Odier, Sandrine Billet, Nathalie Gauthier, Pierre Métral, and Aurélie Chausset for their work in each participating center.
Authors' Contributions
All authors have contributed to this article in significant ways and reviewed and agreed on the content.
Funding
This work was supported by the French National Cancer Institute (INCA-2010-046) and sponsored by CHU Saint-Etienne.
Ethics Committee Approval
Appropriate ethical approval was obtained for the study (Clinical trial number NCT01531478). The authors confirm that this article has not been previously published, is not under consideration for publication elsewhere, and that, if accepted, will not be published elsewhere in the same form, in English or in any other language, without the written consent of the publisher.
Author Disclosure Statement
No competing financial interests exist.