
Abstract
Purpose:
Adult survivors of childhood cancers (ASCCs) are a unique and growing population. Because these individuals were diagnosed in childhood, their developmental stage at diagnosis may influence medical sequelae and perception of their cancer diagnosis and potentially result in long-term complications and challenges. Our aim was to determine how developmental stage, time since diagnosis, and cognitive impairment relate to Canadian ASCC distress and unmet needs.
Methods:
Canadian ASCCs aged 19–77 years (N = 115) diagnosed between ages 0 and 5 (n = 25), 6 and 12 (n = 22), or 13 and 18 (n = 68) completed demographic, neurocognitive self-report, depression, and anxiety and unmet needs questionnaires.
Results:
The developmental stage predicted distress, β = −0.29, p = 0.01. Survivors diagnosed in middle childhood reported significantly more distress than those diagnosed in adolescence. Shorter time since diagnosis predicted greater psychosocial needs, β = −0.24, p = 0.05, and greater distress, β = −0.22, p = 0.05. Greater memory impairment predicted higher need across outcomes, β = −0.36–0.61, p < 0.05. In adjusted analyses for unmet needs, endorsement of cancer affecting education and/or work importantly altered outcomes.
Conclusion:
Our results indicate that greater self-reported memory impairment increases childhood cancer survivors' care needs. We additionally suggest that supportive care interventions might best target those reporting work or education interruption due to cancer. Identification of ASCCs who report work/school interruptions may provide a quick screen for health providers to assess possible need for intervention. ASCCs still experience unmet needs long into survivorship.
Introduction
W
Many ASCCs will experience disruptions to relationships, identity, and/or independence due to their diagnosis. 12 Research and theory in developmental psychology suggest themes specific to each developmental stage that may interact with a cancer diagnosis, resulting in increased future needs. 13 The challenges ASCCs face may be contingent on the developmental context of their cancer diagnosis and treatment through mechanisms such as how they experience these disruptions and cope with treatment neurotoxicities that impact developing brains. A cancer diagnosis during adolescence is related to greater relationship difficulties, 14 lower school completion, 15 delayed psychosexual development, and lower psychosocial and health-related QOL.4,5 These are understandable given adolescents' developmental focus on autonomy, relationships, self-esteem, and sexuality.14,16 By comparison, younger age at diagnosis may lead to lower educational attainment, 15 higher unemployment, 17 greater disability, 18 lower marriage rates, 11 and more care-related health needs.1,19 Young children may have difficulty comprehending the immediate and long-term gravity of their diagnosis 20 and may lag behind in educational and social development due to absenteeism. Particularly for children aged 0–5 years, cancer treatment may impede normal parent–child attachment14,16 and interfere with neurological development, causing lifelong deficits.9,21 Our study adopts this developmental perspective to better understand the unmet needs of ASCCs.
Time since diagnosis and cognitive impairment may also affect distress and unmet needs. In cancer survivors diagnosed as adults, many aspects of distress decrease with time. 22 The same cannot be said for ASCCs as symptoms can relate to either increasing or decreasing time since diagnosis. 9 Cognitive impairments are also common in ASCCs, especially in children treated for brain tumors, acute lymphoblastic leukemia, and head/neck tumors. 23 Cognitive impairments, such as learning and memory problems, often increase emotional distress. 24 We therefore incorporated time since diagnosis and cognitive impairment as possible predictors of unmet needs and distress.
A recent study from the Childhood Cancer Survivor Study (CCSS) found that ASCCs experience a range of unmet needs 25 and identified risk factors accompanying greater unmet needs: female sex, lower socioeconomic status (SES), and children diagnosed between 5 and 14 years of age. In a Swiss study, ASCCs reported that they either did not receive information on treatment, follow-up, or late effects or they only received this information orally, despite desiring written and personalized details. 26 This lack of information led to greater psychological distress and lower QOL. It is clear therefore that ASCCs experience unique unmet needs that need to be addressed.
Although recent studies on ASCCs' unmet needs exist, most focus on healthcare systems quite different from Canada's systems. Of these studies, small sample sizes limit generalizability, except for the American and Canadian CCSS cohort. 27 The current study aims to identify ASCCs' unmet needs and distress in a larger Canadian sample at a later follow-up than previous studies 27 and to examine risk factors, including developmental stage at diagnosis, time since diagnosis, and cognitive impairment, to better understand needs.
Objectives
Our primary objective was identifying the unmet needs that ASCCs face in Canada and to explore the number, level, and types of unmet needs ASCCs experienced by developmental stage at diagnosis. Our second aim was examining how the developmental stage at diagnosis, time since diagnosis, and cognitive functioning interacted to impact distress and unmet needs. Based on prior studies,4,17 we hypothesized that ASCCs diagnosed at younger ages would experience greater practical unmet needs, while those diagnosed at older ages would experience greater psychosocial unmet needs. Because time since diagnosis may increase or mitigate unmet needs 28 and cognitive impairment may increase difficulties,24,29 we included these and all two-way interactions when testing hypotheses.
Methods
Participants
The study received approval from our university's Research Ethics Board. Our cancer registry mailed invitations to all ASCCs in Alberta, Canada, who were 19 years or older with histologically confirmed childhood diagnoses. We excluded those with in situ, nonmelanoma skin cancers, opting out of research contact, or deceased.
Among 1562 eligible ASCCs, the registry had the wrong address or the patient was deceased for 563 and 3 others refused (unknown reasons), reducing the overall eligible population to 996. Of 159 responding ASCCs, 117 ASCCs completed surveys (73.6%), although 2 were excluded (age of diagnosis >18). We examined generalizability using aggregated registry data to find that our sample did not differ from nonresponders by cancer type, χ2(3,1041) = 3.24, p = 0.36, or age, t(1039) = 1.18, p = 0.24, but significantly more women than men completed surveys, χ2(1,1041) = 7.55, p = 0.01. The 115 ASCCs included in these analyses were, on average, aged 35 years and were 23 years postdiagnosis (Table 1). The most common cancer types were lymphoma and reticuloendothelial systems (29.6%) and leukemia (13.0%). Participants reported aggressive cumulative treatments over their lifetimes (72.2% surgery, 65.2% chemotherapy, and 63.5% radiation). Recurrences occurred in 9% and new cancers in 21%.
p < 0.05.
DASS, Depression Anxiety Stress Scale-Short Form; SUNS, Survivor Unmet Needs Survey; CCSS-NCQ, Childhood Cancer Survivor Study Neurocognitive Questionnaire.
Procedure
ASCCs contacted through mail-outs and up to four phone calls consented and participated online (82.6%, n = 95) or through hard copy.
Measures
Independent variables
Demographics and medical history
Participants reported demographics and medical history (Table 1). We created three age-at-diagnosis groups: early childhood (0–5), middle childhood (6–12), and adolescence (13–18).
CCSS Neurocognitive Questionnaire
The CCSS Neurocognitive Questionnaire (CCSS-NCQ), 30 a 25-item Likert-type scale, assesses neurocognitive function (higher scores, higher difficulty) over four dimensions: Task Efficiency, α = 0.91; Emotional Regulation, α = 0.84; Organization, α = 0.80; and Memory, α = 0.89. Subscales were highly correlated, Spearman r = 0.31–0.71, so we only used the Memory subscale.
Dependent variables
Depression Anxiety Stress Scale-Short Form
The Depression Anxiety Stress Scale-Short Form (DASS-21), a short form of DASS, 31 contains three 7-item Likert-type scales (higher scores, higher distress): depression, α = 0.89, anxiety, α = 0.61, and stress, α = 0.85. High correlations between subscales, Spearman r = 0.47–0.60, led to our using a total score (α = 0.90) that is a reliable and valid measure of general distress. 32
The Survivor Unmet Needs Survey
The Survivor Unmet Needs Survey (SUNS) measures cancer survivors' unmet needs. 33 It has 89 Likert-type items (higher scores, higher need; 0 = No unmet need–4 = Very high unmet need) and five subscales: Emotional Impact (α = 0.99), Access/Continuity of Care (α = 0.94), Coping and Sharing (α = 0.97), Finances (α = 0.94), and Information (α = 0.92). We created the Practical Unmet Needs Scale (α = 0.97) from Information, Financial, and Access subscales, Spearman r = 0.52–0.57, and a Psychosocial Unmet Needs Scale (α = 0.99) from the Coping and Emotional subscales, Spearman r = 0.77.
Statistical analysis
Primary analysis
We first examined which items ASCCs endorsed most frequently to better understand their psychosocial and practical unmet needs in Canada.
We examined the normality of distributions and collinearity among variables. Parametric tests were appropriate for both dependent variables (DVs) and independent variables (IVs; developmental stage, time since diagnosis, and CCSS-NCQ memory score). To test hypotheses, we used multiple regressions for each of the DVs with IVs (and all two-way interactions) centered and entered simultaneously.
Sensitivity analyses
For significant IVs, we conducted sensitivity analyses to test whether demographic or medical variables could explain results. If inclusion of these variables resulted in a reduction of significance of IVs, then it is possible that our IVs were proxy to these other variables. Only demographic or medical variables that demonstrated significant correlations with both the IV and the DV were investigated. 34 For continuous or binary variables, we tested associations using Spearman correlations, and for categorical variables, we used one-way ANOVAs. We included any variables that met these criteria in adjusted multiple regressions.
Results
Description of scores
No cutoffs exist for the DASS-21 total score, although depression (M = 4.78, SD = 7.64), anxiety (M = 3.15, SD = 4.50), and stress (M = 6.05, SD = 7.32) were within normal clinical cutoffs 31 ; 4.3% of our participants scored moderate or above clinical cutoffs on depression, 11.3% on anxiety, and 15.7% on stress.
On the CCSS-NCQ Memory subscale, our sample demonstrated significantly more memory problems (M = 6.56, SD = 2.45) compared with a healthy group of ASCCs (M = 5.80, SD = 1.85; t(801) = 3.89, p < 0.001), but less than a group of survivors treated with high-dose cranial radiation to the frontal areas of their brains (M = 7.60, SD = 2.47; t(360) = 3.74, p < 0.001). 30
Unfortunately, no norms exist for the SUNS with ASCCs. On average, our participants reported a relatively low number of practical unmet needs (M = 0.39, SD = 0.71, range = 0.00–3.00) and psychosocial unmet needs (M = 0.67, SD = 0.97, range = 0.00–4.00). On all of these measures, we found no differences in scores among developmental age at diagnosis groups (Table 1).
Primary analyses
Unmet needs
Overall, 45.3% of participants reported at least one High or Very High unmet need in the last month, with 15.4% not reporting any. The most frequently endorsed High to Very High unmet needs were, “Finding someone to talk to who understands” (15.6%), “Worry about earning money” (14.8%), and “Coping with having a bad memory or lack of focus” (13.9%).
We explored unmet needs endorsed for each developmental stage (Table 2). For early childhood, middle childhood, and adolescent participants, respectively, 56.0%, 86.4%, and 82.4% endorsed at least one practical unmet need and 52.0%, 77.3%, and 82.4% at least one psychosocial unmet need.
DASS total score R2 = 0.38, F(9,104) = 7.16, p < 0.001.
Practical unmet needs R2 = 0.19, F(9,105) = 2.76, p = 0.006.
Psychosocial unmet needs R2 = 0.25, F(9,105) = 3.86, p < 0.001.
ASCCs, adult survivors of childhood cancer.
Regressions
Depression Anxiety Stress Scale-Short Form
Shorter time since diagnosis (β = −0.22, p = 0.05), greater memory problems (β = 0.61, p < 0.001), and developmental stage (i.e., a diagnosis in middle childhood predicted increased DASS-21 scores compared with adolescence) significantly predicted greater DASS-21 total score. No significant differences emerged between middle childhood and early childhood groups (Table 3 and Fig. 1).
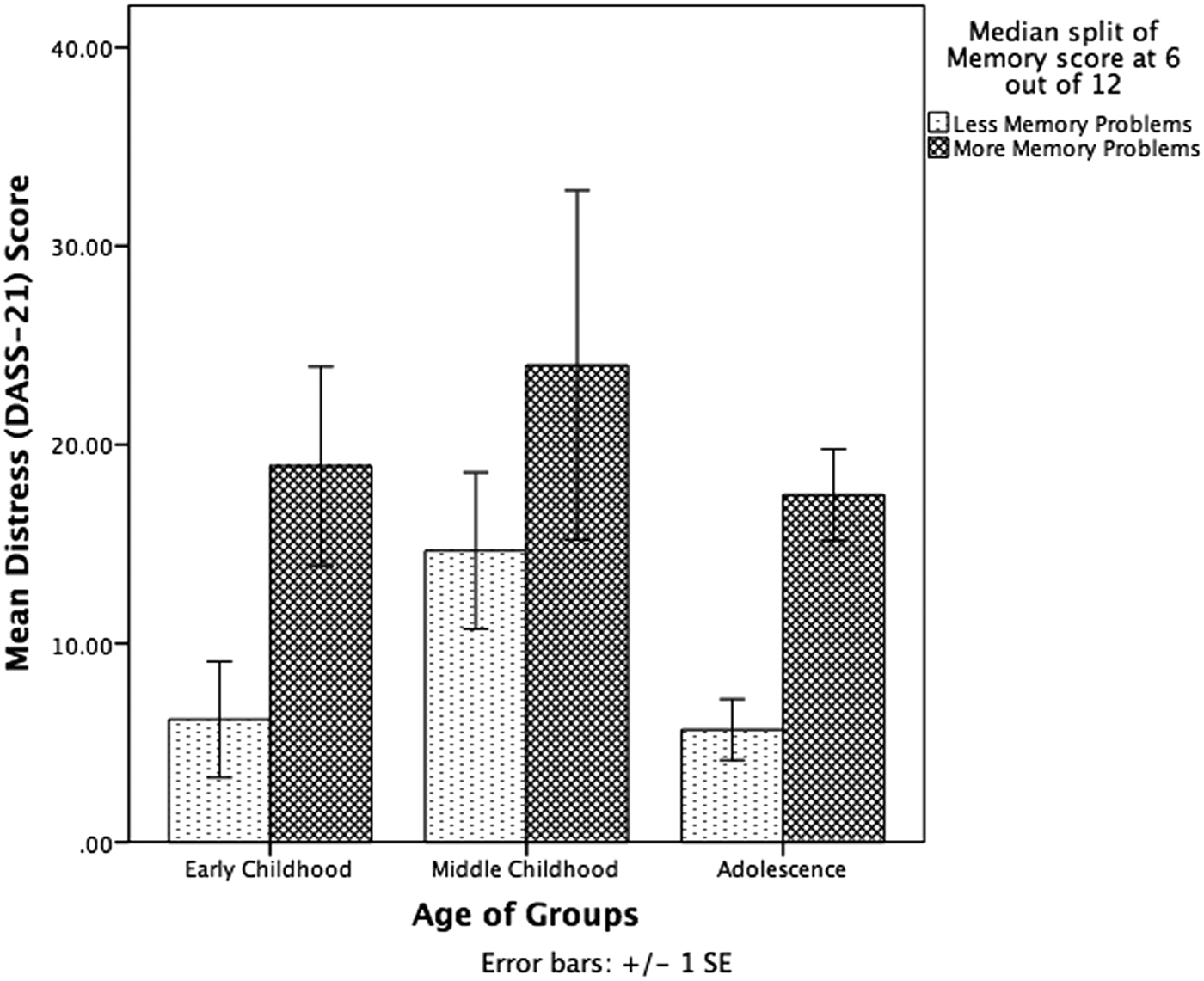
Significant predictors of distress (DASS-21), developmental stage by memory score. DASS, Depression Anxiety Stress Scale-Short Form.
Practical unmet needs
Greater memory problems (β = 0.36, p = 0.001) significantly predicted greater SUNS practical unmet needs. No significant developmental-stage or time-since-diagnosis effects emerged (Table 3).
Psychosocial unmet needs
Greater memory problems (β = 0.45, p < 0.001) and shorter time since diagnosis (β = −0.24, p = 0.05) significantly predicted greater psychosocial unmet needs. No significant developmental-stage effects emerged (Table 3 and Fig. 2).

Significant predictors of psychosocial unmet needs (SUNS), time since diagnosis by memory score. SUNS, the Survivor Unmet Needs Survey.
Sensitivity analysis
Age, gender, ethnicity, cancer type (CNS cancer vs. non-CNS cancer), recurrence, radiation treatment, and second cancers did not correlate with either IVs or DVs and therefore were not considered proxy variables. However, the binary variable “did your cancer experience directly affect your education and/or work?” significantly correlated both with IVs (memory score, time since diagnosis, and developmental stage) and DVs (practical and psychosocial unmet needs, but not DASS total score). Therefore, we adjusted unmet needs' equations to test whether results were proxy to this variable.
Adjusted regressions
Endorsing education/work disruptions significantly predicted greater practical unmet needs, β = 0.26, p = 0.04, but greater memory problems, β = 0.21, p = 0.11, and was no longer significant, adjusted R2 = 0.14, F(14,100) = 2.27, p = 0.01. Memory was proxy to the underlying report of cancer affecting education/work.
With education/work in the equation, greater memory problems, β = 0.26, p = 0.03, and shorter time since diagnosis, β = −0.24, p = 0.05, still significantly predicted greater psychosocial unmet needs, adjusted R2 = 0.24, F(14,100) = 3.57, p < 0.001. Endorsing education/work significantly predicted greater psychosocial unmet needs, β = 0.28, p = 0.02, with a significant education/work by memory interaction, β = 0.26, p = 0.03 (Fig. 3). In this study, results were not proxy; the interaction of education/work and memory score was an additional predictor.

After adjustment, significant predictors of psychosocial unmet needs (SUNS), interaction of memory score and cancer affecting education/work.
Discussion
We found that many ASCCs in Canada report High and Very High unmet needs, especially about finding someone who understands their experiences, worrying about money, and memory problems. The middle childhood group experienced the most unmet needs. We examined whether developmental stage at diagnosis, time since diagnosis, memory impairment, and their interactions predicted levels of distress and practical and psychosocial unmet needs and found that greater self-reported memory impairment predicted higher need across all outcomes. Developmental stage significantly affected distress, with those diagnosed in middle childhood reporting greater distress than those in adolescence. Shorter time since diagnosis significantly predicted greater psychosocial unmet needs and greater distress. In adjusted analyses for practical and psychosocial unmet needs, we found that cancer disrupting education and/or work importantly altered outcomes. Memory impairment was not as important in predicting unmet practical needs as cancer impacting education and/or work. For psychosocial unmet needs, education/work and memory significantly interacted to predict higher needs, while the significance of shorter time from diagnosis remained unchanged. Those who endorsed disruption of their education/work had a linear increase in psychosocial unmet needs for each increment in memory impairment (Fig. 3) that was absent for those not endorsing this fact. These results suggest that meeting survivors' supportive care needs may require personalizing interventions.
Our participants rated Coping and Sharing, Financial, and Emotional unmet needs highly. These differed from those reported in studies with adult cancer survivors, 33 where the top unmet needs were, “Fears about cancer spreading,” “Being told I had cancer,” and “Not feeling sure that the cancer has gone.” Sample dissimilarities in years post-treatment may explain these differences as Campbell et al.'s rates were 1–5 and ours were 3.68–62.68. It is also possible that a diagnosis in childhood versus adulthood may account for differences. Adolescent and young adult survivors of cancer in Canada report a need to talk to peers with similar experiences and a need for psychological and emotional support, 35 similar to our results, suggesting that ASCCs have unique needs. 36
In examining predictors of needs and distress, our analysis suggested that memory problems were particularly important. Previous studies indicate that treatment-related cognitive impairment can negatively impact health-related QOL,37–39 emotional distress, 24 educational/work attainment, 40 and relationship success.41,42 Our study supports these results by showing that greater self-reported memory impairment increases survivors' care needs. Supportive care interventions for ASCCs might best target those reporting cancer-related education or career interruptions. This single factor may provide a quick screen for clinicians to assess the need for intervention.
We found minimal support for associations between developmental stage at diagnosis and unmet needs; however, those diagnosed in middle childhood compared with adolescence experienced greater distress. Previous research documents mixed results; some studies have found an association between greater distress and younger age at diagnosis,1,11 while others found the opposite.4,5,14 However, these studies typically examined age at diagnosis as a continuous variable, which may mask the distress associated with a middle childhood diagnosis. In addition, treatment toxicities may be worse for younger children's brain and social development,9,21 leading to more serious late effects.
Complicating this picture, patients treated in older eras likely received more toxic treatments. In the 1960s, fewer than 50% of children lived 5 years post-treatment, 43 although now the 5-year survival rate is >80% 44 due to changes such as reduced dose radiation and lower dose chemotherapy.45,46 Despite temporal changes in therapeutic exposures in childhood cancer treatments, self-reported health status is not significantly improved by treatment era. 47 Similarly, we found that a shorter time since diagnosis was associated with more distress, suggesting that more support is required especially in the years immediately post-treatment. While past studies typically focus on a specific time since diagnosis, 48 our mean follow-up time of 23 years postdiagnosis represents a noteworthy time period and offers implications for clinicians seeking to provide relevant support to all ASCCs regardless of time from diagnosis.
In our study, 24.0% of those diagnosed in early childhood reported that cancer affected education/work, compared with higher levels in middle childhood and adolescence (68.2% and 77.9%, respectively). The middle childhood group received significantly more radiation (86.4%) compared with adolescence and early childhood (61.8% and 48.0%), and a higher percentage did not finish high school (18.2% vs. 7.4% and 4.0%). These findings may partially explain the greater distress in our middle childhood group, as research documents dose–response radiation effects on brain development and education. 37 However, sensitivity analyses found it unnecessary to adjust for radiation, nor was radiation significantly correlated with outcomes (Spearman r = 0.05–0.14), so this alone cannot fully explain our results. Future research is needed to replicate findings with regard to distress in different developmental stages at diagnosis.
Qualitative exploration of the commonly endorsed unmet needs at each stage shows some possible developmental differences (Table 2). Those diagnosed in early childhood endorsed financial, trust, and psychosocial unmet needs; those in middle childhood endorsed information, financial, specialist access, and psychosocial unmet needs; and those in adolescence endorsed psychosocial unmet needs. These can be construed to reflect developmental themes. In early childhood, given children's dependency on caregivers, they may not comprehend their disease or anticipate long-term complications,20,49 and thus dependencies for financial and information needs may extend into adulthood. In middle childhood, treatment may threaten normative social and academic achievement due to absenteeism, 20 leading to greater sensitivity and isolation compared with their peers continuing into survivorship. In adolescence, peer relationships are particularly important, 14 and disruptions to the development of social skills and relationships may manifest as psychosocial distress and needs into adulthood.
Limitations, Implications, and Future Directions
Our sample size, while larger than other Canadian samples, limited our generalizability. It is possible that we were unable to detect more complex interaction effects due to sample size. In addition, given the nature of our sampling procedure, it is possible that self-selection to participate in this study may bias results. Response rates were lower than anticipated due to the transient nature of young adults and ethical limitations restricting our use of the most up-to-date patient address databases. We included survivors regardless of cancer type and time from diagnosis, giving a broad picture of survivor needs, but limiting understanding of specific cancers, treatments, and post-treatment periods. Additionally, given the significant time since diagnosis in our sample, it is possible that unmeasured more recent life events may relate to their distress and unmet needs.
The findings from this study provide several suggestions for clinical interventions. First, asking current ASCCs whether their education/work was affected by cancer may be a quick screen to identify those who may need additional support. Second, possible interventions could consider what normative developmental tasks are for the child's age at treatment and, as much as possible, integrate support to maintain the child's ability to progress through those stages. For school-age children, maintaining schoolwork and active and meaningful peer contact is a developmental priority, and recent interventions, including social media and online interactions with peers, may be helpful.50,51 Third, after treatment is complete, there is often little attention to survivorship needs. And of support that is available, most does not focus on vocational training that may importantly decrease distress and unmet needs.
In summary, this was one of the first studies to relate developmental stage at diagnosis to unmet needs in Canada, finding limited evidence of these relationships. Surprisingly, longer time since diagnosis meant lower needs. Participants endorsed more psychosocial unmet needs related to emotions and social identity than practical unmet needs relating to healthcare experiences. Future studies could qualitatively examine the experiences of ASCCs and would benefit from more effective tracking of long-term survivors. Asking if cancer affected ASCCs' education/work may allow clinicians to quickly assess needs. In addition, this study provides insight into enhancing preventive psychosocial interventions during childhood and coping interventions into survivorship.
Footnotes
Acknowledgments
This research was supported by a grant from the Enbridge Research Chair in Psychosocial Oncology and Alberta Cancer Foundation to the last author. The authors thank Dr. Linda E. Carlson for her feedback and input on the manuscript. The authors thank the ASCCs who participated in this study.
Author Disclosure Statement
No competing financial interests exist.