
Abstract
Purpose:
Resuming normal activities, such as work and school, is an important dimension of psychosocial recovery in cancer survivorship. Minimal data exist regarding adolescents or young adults' experiences of returning to school or work after cancer. The purpose of this study was to explore the processes of resuming work and school among adolescents and young adults after hematopoietic cell transplantation (HCT).
Methods:
In-depth interviews were conducted with 18 adolescents and young adults, who were 15–29 years when they underwent HCT and 6–60 months post-transplant at study enrollment. Interview transcripts were systematically analyzed using Grounded Theory methodology.
Results:
Participants described the context in which they attempted to return to work or school, specific challenges they faced, and strategies they developed in these environments. Feeling left behind from their peers and their pre-diagnosis selves, participants described “rushing” back to school and work impulsively, taking on too much too quickly while facing overwhelming physical and cognitive demands. Factors motivating this sense of urgency as well as barriers to successful and sustainable reentry in these settings are also addressed.
Conclusion:
Findings are discussed in the context of important opportunities for clinical management, age-appropriate interventions, and implications for future research. A better understanding of psychosocial late effects, specifically related to school and work trajectories after cancer, is critical to survivorship care for adolescent and young adult cancer survivors.
Background
L
In broader samples of adult and pediatric cancer survivors, more intense treatment regimens have been associated with significant challenges during reentry and poorer social functioning during the post-treatment period.6–10 HCT survivors face substantial risk for treatment-related morbidity that can contribute to non-relapse mortality and impaired functioning, such as chronic graft-versus-host disease, endocrinopathies, cardiopulmonary effects, musculoskeletal disorders, and subsequent malignancies.1,4,5,11–14 In addition, psychosocial challenges among HCT survivors include neurocognitive impairments,13,15 diminished quality of life, 16 difficulty resuming social roles, 17 fatigue, 18 infertility and sexual dysfunction,19–22 distress, 23 post-traumatic stress disorder, 24 and depression. 25 Although many survivors are able to work after HCT,26–28 they often report long-term challenges in this area, such as job insecurity, financial losses, physical and mental barriers to working, career derailment, and poorer quality of life.29–31
The impact of treatment intensity on psychosocial outcomes among AYAs remains largely unexplored.32,33 In one of the few studies available, AYAs who endured more intensive treatments were less likely to resume full-time work or school and four times more likely to report that cancer had negatively impacted their school and work plans compared with those who received less intense treatments. 34 These findings suggest that survivors of HCT are a particularly vulnerable group of AYAs in terms of work and school outcomes. Despite the prevalence of hematological malignancies in early adulthood 2 and the intensity of HCT, 35 little is known about AYA cancer survivors who have undergone HCT. Therefore, we selected a qualitative approach to highlight the experiences of this subgroup of AYAs. In this article, we describe the process of resuming activities related to work and school among AYAs after HCT, including factors that influenced their decisions if and when to resume, specific challenges related to functioning and sustaining engagement (initially and over the long term), and strategies they developed to adapt to work- or school-specific demands.
Methods
Setting and recruitment
After institutional review board approval at both the University of California, Los Angeles and City of Hope National Medical Center, we identified potentially eligible patients by using a medical chart review, and then obtained permission from treating hematologists (Fig. 1). Study eligibility included individuals who were 15–29 years old at the time of a single bone marrow or stem cell transplant for a primary diagnosis of hematologic cancer and who were currently 6–60 months post-HCT. Exclusion criteria included: history of previous HCT, disease relapse after HCT, non-English speaking, or younger than 18 years old at study enrollment. Of the 106 eligible patients identified, medically complex patients, defined by suspected relapse or recent hospitalization for HCT complications (n = 13), were not approached. Patients receiving follow-up care elsewhere (n = 34) or without physician permission (n = 1) were also not approached. Invitations to participate were mailed to the remaining 59 potential participants. We followed up by telephone or at scheduled appointments in the outpatient clinic to discuss possible study participation.
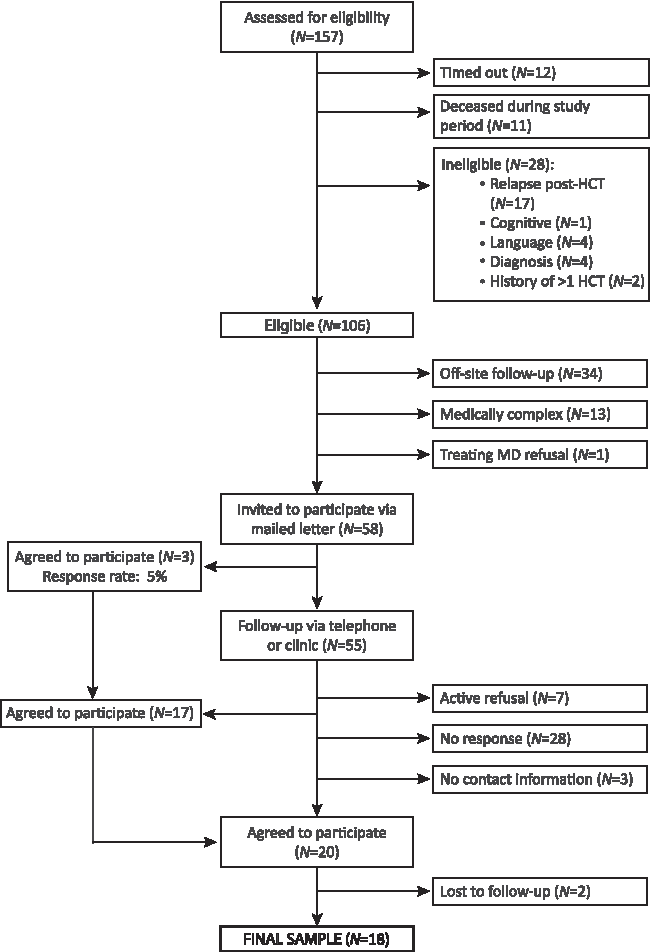
Summary of recruitment.
Data collection and analysis
Grounded theory methodology, influenced by Constructivism, guided all aspects of the study.36,37 Using this inductive, qualitative approach, data collection and analysis occurred concurrently to allow for constant comparison. 37 After obtaining informed consent, participants completed a sociodemographic questionnaire followed by an in-depth interview conducted by the first author in a convenient, private location or via telephone. A semi-structured interview guide was developed from a previous pilot study with AYAs by the first and last authors (Table 1). Interviews were digitally audio-recorded, transcribed verbatim, and de-identified. The duration of interviews was, on average, 102.4 minutes (range: 56.4–164.2 minutes). Participants received a $50 gift card for their time.
HCT, hematopoietic cell transplantation.
Through a systematic yet flexible coding process, we attached analytic meaning to segments of data. We began with the initial coding of each transcript to study the data while remaining open. Then, we used focused coding to develop salient codes and identify tentative categories. In later interviews, theoretical sampling allowed us to gain needed insights, fill out properties of emergent categories, and elaborate relationships between categories. We refined our theoretical interpretation of the data through memos and diagrams.36,37 This analytic process continued until major theoretical categories were deemed saturated and robust and no new properties emerged. 36 To enhance rigor, we ensured sufficient breadth and depth of observations, engaged in reflexive memo-writing, recorded field notes and process memos, and involved at least two researchers in independent analysis and collaboration at each stage.36,37 The Atlas.ti software program supported overall data management. 38
Results
Sample characteristics
A total of 18 individuals were interviewed. Participants were, on average, 23.3 years of age at HCT and 26.0 years at study enrollment. The average time since HCT was 32.8 months (range: 8–60). Medical and sociodemographic characteristics are listed in Table 2. In the following sections, we describe theoretical categories of “rushing” to resume school and work after HCT, fears contributing to this urgency, and barriers to successful, sustainable reentry (Table 3).
“Rushing” to resume
As participants emerged from the isolation of treatment and recovery, they aimed at moving beyond the cancer and HCT experience “as if it hadn't happened.” Rather than accommodate persistent health issues, participants described a fierce determination to “catch up” by “rushing” to make up for “lost” or “wasted” time. After being “obsolete for a while” due to illness, participants admitted that they were “chomping at the bit,” “begging,” or even “harassing” their medical teams for permission to resume school or work as soon as possible. One participant compared this rush with the slow pace of treatment, “I went from snail mode to rocket ship mode. Those are just two very big extremes.” Rushing was characterized by an overriding urgency to resume school and work, often resulting in overextension, lack of preparation, and unrealistic expectations.
Fears of falling further behind and never catching up superseded concerns about lingering health issues. Participants acknowledged that rushing was entirely self-generated; neither their family nor medical team pressured them to do so. As one participant explained, “I had to do what helped me get through the post-cancer part.” On reflection, participants regretted rushing back to work or school and admitted feeling unprepared physically or emotionally. They commented that a longer period of physical and psychological rehabilitation would have been beneficial.
Motivating factors
“Rushing” to resume pre-illness activities of work and school was motivated by three major fears: being left behind, never moving on, and losing the life they had known before diagnosis.
Feeling “left behind”
The prospect of school and work activities outside of the home required participants to survey the aftermath of their cancer and HCT experiences in a broader context. Participants described navigating a changed reality and felt alienated from their pre-diagnosis lives. Many struggled to relate to peers, who had accumulated life experiences without them. Participants also felt behind compared with what they understood to be the normal milestones of young adulthood, or “the regular flow of things,” such as education, career, home ownership, intimate partnerships, or family building. Feeling left behind in these areas triggered jealousy, anger, depression, and deeper fears of failure.
Danger in “dwelling”
Despite feeling uncertain about their health, participants worried that “dwelling,” or overanalyzing their situation, would prevent them from moving on. They described hustling to “get on with my life already” because they feared that if too much time elapsed, the window to catch up and reclaim their pre-illness potential would close entirely. One participant shared, “If I don't push myself enough, I just won't go back to the point where I was before,” while another explained, “I was worried that if I waited too long, I would lose that ambition and just get to a point where I'm like, ‘forget it,’ and I didn't want that for myself.” In this vein, participants also avoided connecting with other cancer survivors. One participant quit her volunteer work with a community-based cancer support network, explaining, “I felt like, if I continue, I'm just going to constantly stay in that mindset that cancer's always going to be around me. And I didn't want that.”
Salvaging “my old life”
Participants also rushed back to work and school in the hope of salvaging what they remembered of their pre-diagnosis lives. Many wanted to hold on to their “old lives,” seeing them as superior to any future they could now imagine for themselves. Participants strongly preferred returning to their pre-illness work and school settings, although this was often impossible. For many, physical limitations prevented them from work-related tasks such as sitting on the floor as a preschool teacher or lifting large boxes at a warehouse store, whereas others could not return to jobs without adequate health insurance. Participants who did return to pre-illness jobs described a smoother transition due to flexible accommodations compared with those who returned to school or started in new settings. One participant explained that his boss allowed him to return full-time for salary and health benefits, even though he “knew that I wasn't going to be at full capacity.”
Barriers to successful, sustainable reentry
Attempts to “catch up” by rushing “into the deep end” of work and school revealed new health issues not previously faced at home. As physical and mental demands increased, many participants felt painfully aware of treatment-related limitations, particularly fatigue, cognitive difficulties, and susceptibility to illness. Participants also tried to curtail the impact of breaks in their schooling due to treatment.
Fatigue
Simply attempting to participate in school or work necessitated substantial increases in activity levels and subsequently higher levels of fatigue. Attending a single class involved a long list of mental and physical tasks, including getting ready, commuting, parking, walking to class, possibly climbing stairs, concentrating, socializing, and commuting home. Many participants described coming home after school or work and collapsing from utter exhaustion.
Participants developed strategies to manage overwhelming fatigue. One participant used a wheelchair to increase independence and conserve energy on a college campus, explaining, “I could walk, but I would take a few steps and I felt like I ran a marathon.” Several participants also learned the value of incorporating recovery time into their schedules, such as avoiding classes 2 days in a row because “back-to-back was too much.” However, many participants ultimately sacrificed healthy behaviors, such as adequate exercise, nutrition, and sleep, and resorted to skipping classes to compensate for fatigue.
Cognitive difficulties
Post-HCT cognitive changes, particularly in memory, attention, and concentration, became more apparent to participants as their mental workload increased at school or work. Particularly at school, struggles with slower thinking, memorization, and working under the pressure of exams or deadlines added a significant layer of difficulty. “Chemobrain” was more elusive than other symptoms because it was difficult to understand, predict, and self-manage. Input from healthcare providers about managing cognitive difficulties was also vague. Although some participants utilized school services for students with disabilities, they often found the offerings unhelpful. For example, extended time on exams did not make it easier to recall information when their mind went blank.
Cognitive changes were also emotionally disturbing and “frightened” participants. Although adaptive strategies, such as daily lists and calendar reminders, were useful in managing these issues in daily life, participants reported dismay that their symptoms seemed to be worsening rather than improving. They agonized about the long-term impact of treatment on their brain and how this might affect their futures.
Susceptibility to illness
Participants' weakened immune system and susceptibility to infection further complicated the return to school and work. Outside of the home, participants experienced frequent illnesses, which exacerbated their worry about relapses and readmissions to the hospital. For one participant, sickness dominated his first year of college; he reported, “every single person that I encountered who was sick, I caught the sickness.” This susceptibility also heightened anxiety about exposure to “germs” and the school or work environment itself as a health threat.
Impact of breaks in school
Overcoming disruptions in school trajectories due to treatment was another significant challenge at reentry. Participants were not able to stay in school during HCT, and many were forced to withdraw mid-year. Unfortunately, these abrupt departures resulted in distressing losses in academic credits and financial investments due to rigid school policies. Many participants lacked support in coordinating formal medical leaves from school. Therefore, when they attempted to return, many were surprised to face administrative hurdles. One participant, who stopped attending college “without telling them anything,” became depressed when he was told, “You didn't take a leave of absence. So, you're no longer a student here.”
As participants attempted to resume work and school, they felt determined to overcome challenges initially. However, the experience of repeated disappointments and failures in these settings left most participants dejected, as one explained, “I just couldn't rebound.”
Discussion
Our findings are among the first to articulate AYA cancer survivors' experiences of returning to work and school after HCT, an intense treatment with significant long-term sequelae. At diagnosis, all participants were in school, employed, or both. At the time of their interviews, participants were, on average, in their third year of recovery and although most had attempted to resume pre-illness activities, six were neither employed nor in school and 11 were managing only one role (school or work), often at part-time status. We found that when AYAs rushed back to school and work after HCT, they experienced immense challenges, a lack of preparation, and a need for specific guidance from healthcare and education professionals to facilitate this important step of survivorship.
The ability to resume work-related activities after HCT is an important indicator of psychosocial recovery and can affect quality of life.29,39 Current research suggests that adult HCT survivors face long-term challenges at work.29–31 Adults who are unemployed 1 year after HCT report higher rates of fatigue and pain, poorer perceived health, and lower quality of life than those who return to work. 39 In our study, several participants did not return to work and many worried about their future employability. Those who returned to previous jobs relied on the empathy of supervisors rather than knowledge of specific policies intended to protect cancer survivors in the workforce. Thus, AYAs may need additional support in navigating return to work and connecting to resources on work protections.
Consistent with other studies on adult cancer survivors returning to work, participants overestimated their functional ability.40,41 Particularly at school, the tendency to take on too much too quickly resulted in demoralizing struggles and even failures. Our findings suggest that AYAs may be particularly at risk for these overestimations because of their developmental determination to catch up with peers and deep fear of losing their ambition. Pediatric care models commonly include school reintegration programs to minimize the effects of cancer-related breaks in education because of federal mandates to protect children with cancer.42–45 Unfortunately, these programs do not typically extend beyond the K-12 setting, leaving AYAs who are in post-secondary programs without much needed resources.
AYAs in our study received a “green light” from their medical teams to resume pre-illness activities, but little guidance about how to implement this decision in light of lingering health issues. Participants expressed frustration that healthcare providers did not understand the rigidity of school requirements, whereas school-based disability services seemed ill-equipped to deal with the complexity of cancer survivorship. Unsurprisingly, this disjointed approach results in distress and difficulty for AYAs who are trying to resume activities. Expertise related to cancer survivorship, particularly late effects of high toxicity treatments, is needed to develop realistic, meaningful education plans that leave room for adjustments and enhance chances for success.
Future research should focus on more formal school and work reintegration interventions for AYAs that are tailored to the specific demands of higher education, early workforce status, and young adult developmental needs. A rehabilitation-focused approach that begins well in advance of actual resumption could provide substantial assistance to this patient population. Interventions, such as occupational or physical therapy, that target persistent post-treatment issues including fatigue and cognitive difficulties may better prepare AYAs for work and school demands.46–49 Another promising but relatively untapped area is the use of internet-based health interventions, 50 mobile apps and m-health,51,52 or video game technology 53 to ease the transition back to school or work for AYAs.
There are several limitations from this small qualitative sample. Participants were recruited from a single specialized institution with an established survivorship program for HCT patients. It is possible that AYAs receiving care elsewhere may be connected to fewer resources. The 5-year post-HCT span provides insight into various experiences along the HCT trajectory, whereas the cross-sectional design does not reflect longitudinal trends. Many participants underwent extensive treatment before HCT, and therefore, disruption in work and school trajectories is not necessarily a direct result of HCT. Because of the younger age of our sample (15–29 years at HCT) with respect to the National Cancer Institute definition of AYA (15–39 years), 54 our findings may be disproportionately focused on school rather than work issues.
Nevertheless, we have documented major challenges in return to work and school for AYAs after high-intensity treatment with HCT. Longitudinal studies are needed that track educational and work outcomes in relation to medical and developmental changes. In the future, differences across important AYA subgroups should be further investigated to develop risk profiles and identify preferences, concerns, and areas of greatest need for support.
Footnotes
Acknowledgments
The authors would like to acknowledge the Oncology Nursing Society (ONS)/ONS Foundation (Dissertation Research Grant), the NIH/NINR Ruth L. Kirschstein National Research Service Award (NRSA) Institutional Research Training Grant T32 NR 07077 for financial support for this project. They would also like to extend their appreciation to Dr. Julie Wolfson, Dr. Saro Armenian, Dr. Stephen Forman, Lindsey Hageman, Alysia Bosworth, and Laura Gustafson for their administrative support of this project.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review boards and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Author Disclosure Statement
No competing financial interests exist.