
Abstract
Ovarian tumors presented with ovarian mass in childhood and adolescence are uncommon but an important part of gynecological cases. Struma ovarii is one of the rare cystic benign ovarian tumors that is observed predominantly in women who are between the ages of 40 and 60 years old. It is extremely rare in adolescents. Herein, we present a 14-year-old adolescent girl with struma ovarii who presented to the emergency room with abdominal pain.
Introduction
O
We present a 14-year-old adolescent girl with struma ovarii who presented to the emergency room with abdominal pain.
Case
A 14-year-old adolescent girl presented to the emergency room with complaints of abdominal pain and increasing abdominal girth. There was no significant medical history. An ultrasonography of the abdomen showed a 13 cm solid lesion that had arterial and venous blood supply originating from the right ovary. An abdominal contrast-enhanced computed tomography scan revealed a 10 × 7 × 5 cm necrotic pelvic mass with contrast enhancement without any extraovarian lesion (Fig. 1A). No evidence of metastasis was noted with computed tomography. Blood lactate dehydrogenase (LDH), alpha fetoprotein (AFP), carcinoembryonic antigen (CEA), CA125, CA19.9, and CA15.3 levels were normal and thyroid function tests of the patient were also in the normal range. Beta-HCG level was negative. We had a preoperative diagnosis of malign germ cell tumor and laparotomy was performed. A solid 10 × 5 cm white cyst that originated from the right ovary was observed (Fig. 1B). Right ovarian cystectomy was performed. Intraoperative frozen section was performed and it was consistent with struma ovarii. The patient was discharged from the hospital on postoperative day 4 with good pain control and without incidents.
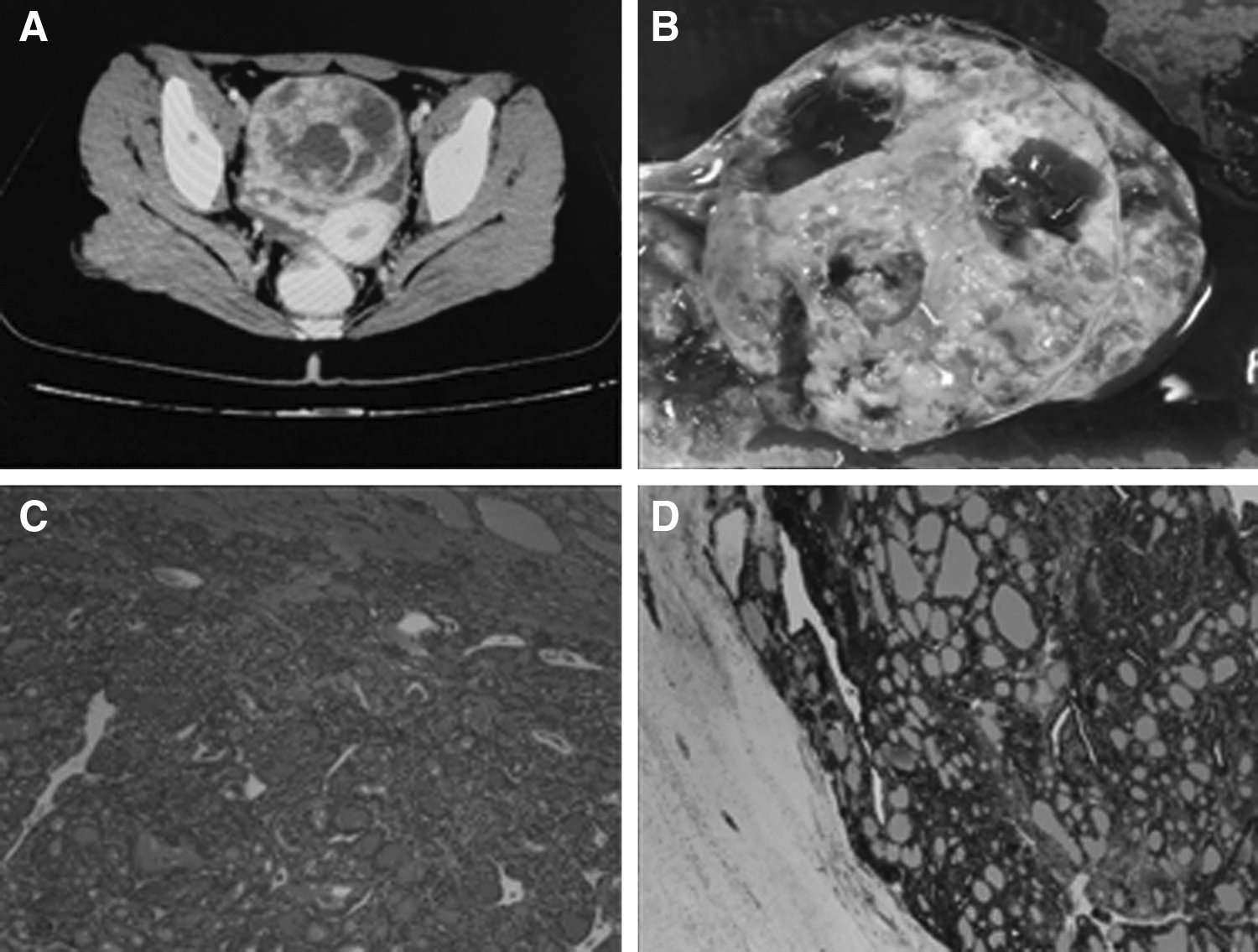
Pelvic mass seen in abdominal computed tomography
Final paraffin block evaluation revealed normal thyroid tissue with markedly crowded follicles that showed diffuse expression of thyroglobulin and CK19 in immunohistochemistry, resulting in a diagnosis of proliferative struma ovarii (Fig. 1C, D).
She was followed up every 6 months for 1 year. Her ultrasonographic scans did not show any abnormality. She continues to menstruate regularly after surgery. We will continue to see her every year.
Discussion
Struma ovarii was first described in 1895 by Von Klden and in 1899 by Gottschalk. In 1889, Boettlin noted thyroid tissue in an ovarian dermoid.8,9 Struma ovarii is histologically characterized by the presence of at least 50% of thyroid tissue. 2 Functional thyroid tissue in the ovary may cause classical symptoms of hyperthyroidy, and Ezon et al. reported that hyperthyroidy can be observed in up to 12% of all cases of struma ovarii.2,6 In our case, no hyperthyroidy symptom was observed by the patient. Moreover, blood tests for thyroid function were normal. Struma ovarii is mostly seen between the ages of 40 and 60 years, but there are some case reports at younger ages. 2 In our case, we presented a 14-year-old adolescent girl with struma ovarii. To the best of our knowledge, the youngest patient described in the literature to have struma ovarii was also at the age of 14 years. 10
Patients usually present with abdominal pain and pelvic mass. In our case, the patient presented to the emergency room with abdominal pain. We performed ultrasonographic examination and found that the pelvic mass originated from the right ovary. Struma ovarii is usually observed <10 cm in diameter in the literature. However, Ezon et al. described a case with 30 cm struma ovarii. 2 Our patient's pelvic mass was 10 × 5 cm macroscopically. In the literature, no correlation could be described between the malignant potential of the tumor and the size of the tumor.
Struma ovarii can be malignant or benign histologically. The management is surgery through laparotomy or laparoscopy. 11 Although cystectomy or oophorectomy is sufficient for benign struma ovarii, complete surgical staging including pelvic and para-aortic lymphadenectomy is suggested for malignant struma ovary. We performed cystectomy by laparotomy and we performed frozen section because the ovarian tumor was mostly solid in preoperative imaging, resulting in a malignant appearance. Struma ovarii has a nonspecific nature of presentation that often mimics ovarian malignancy. Many times it is not in the differential diagnosis because of its rarity. 8 This is important because when there is an ovarian solid mass in an adolescent girl, germ cell malignant neoplasms are considered in the differential diagnosis. This may lead to direct oophorectomy instead of cystectomy during surgery of these young girls compromising future fertility for a benign lesion of the ovary.
In the literature, some authors argued that the term “proliferative struma ovarii” should be used to describe a proliferative follicular lesion of the ovary without evident malignant features. 12 Park et al. could not completely exclude malignant potential, and they diagnosed the lesion as a “follicular proliferative lesion, requiring long-term follow-up”. 12 There is no data in the literature suggesting follow-up for benign struma ovarii. However, patients with proliferative struma ovarii may be better followed up, because there are very few patients to make a conclusion.
In conclusion, this case report demonstrates a rare benign ovarian tumor in adolescents that may mimic ovarian malignancies. Although struma ovarii is extremely rare in adolescents, it must be kept in mind when diagnosing young patients presenting with solid pelvic mass during planning for surgical management.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.