
Abstract
Introduction:
Multiple myeloma (MM) is considered as a disease of the old with the reported median age of 60–70 years. The disease occurred a decade earlier in the Indian subcontinent. The literature on MM in adolescents and young adult (AYA) is limited. We studied the disease characteristics and outcomes of the AYA-MM in the real-world setting.
Patients and methods:
It is a retrospective single-center study conducted at a tertiary care center from North India. Records of all consecutive patients with AYA-MM (15–39 years of age) who were managed from January 1, 2010, to December 30, 2015, were reviewed. Survival was assessed from the date of start of treatment to the last follow-up date or death due to any cause.
Results:
A total of 415 patients managed for MM were included in the study. The frequency of the AYA-MM was 9.6% (40/415) of whom 5 patients were younger than 30 years. There was male preponderance with a median age of the patients being 38 years. The main presenting features were bone pain (55%), fatigue (45%), extramedullary plasmacytomas (20%), and infections (12%) and referral from the peripheral hospital as renal dysfunction (58%). On the evaluation of patients, hypercalcemia, renal impairment, anemia, and lytic lesions were seen in 24.32%, 30%, 52.5%, and 59.25% of patients, respectively. The majority had the high-risk disease (International Staging System [ISS]-III: 75%). Only 22.5% patients were transplanted. The 3-year median overall survival of the study population was 80.21%.
Conclusion:
AYA-MM patients have a higher prevalence of extramedullary disease and high-risk disease.
Introduction
P
Multiple myeloma (MM) is a disease of the elderly with peak incidence at 60–70 years.13,14 The disease is rare in the younger age group with the incidence in patients younger than 40 years being 2%.14–17 The number of reported case series on the incidence, clinicopathological characteristics, and survival of MM in this age group is limited in the literature.15–20 Furthermore, there are no data from the real world on myeloma in patients younger than 40 years. The challenges of AYA and cancer are also pertinent for MM patients. The aim of the current study was to identify the disease characteristics and outcomes of the AYA myeloma patients managed in the real-world situation.
Patients and Methods
Patients
In this retrospective observational study, 415 diagnosed patients of MM who were managed at a tertiary care center from northern India, during the period from January 2010 to December 2015, were analyzed. Inclusion criteria included (1) patients 15–39 years of age of either gender and (2) definitive diagnosis of MM based on the prevalent criteria. Exclusion criteria included (1) patients with no continuation of therapy (loss to follow-up) after registration in the clinic, (2) patients visiting only for a second opinion, and (3) patients who refused any therapy for any reason.
Criteria
Diagnosis of MM was based on the International Myeloma Working Group (IMWG) consensus guidelines. 21 International Staging System (ISS) was used to stage the disease. 22 The remission and response were based on the 2008 IMWG criteria. 23
Methods
The demographic details, symptomatology, and other myeloma-related laboratory investigations were analyzed. In addition, type of chemotherapy administered and survival outcomes (progression and overall survival [OS]) were assessed and compared to all ages. We audited the clinical database of these patients, including outpatient records and indoor admission files; all patients alive were clinically examined and interviewed for cross checking the details of the retrospective records. The study was conducted in accordance with the institutional guidelines after Institutional Ethical Clearance of the Post-Graduate Institute of Medical Education and Research.
Statistical analysis
SPSS ver. 16.0 was used for the analysis. The results were mentioned as median and mean range for all continuous variables. Response rates to treatment regimens were assessed using χ2 test. Kaplan–Meier analysis was used for survival analysis. OS was estimated from the time of starting therapy to the last follow-up or event date. Events were defined as death due to any cause while on follow-up for MM management.
Results
A total of 415 patients managed for MM in the last 5 years were included in the study. The frequency of the AYA-MM was 9.6% (40/415) of whom 5 patients were younger than 30 years. There was male preponderance with males 65.0% (n = 26) and females 35% (n = 14). The mean age of the patients was 36.025 ± 4.67 (median 38, 95% confidence interval [CI] 34.53–37.51, range 18–39). All patients except one were married. The median income for the group was INR 6000 (range: INR 600–50,000; mean INR 13,535 ± 15,316). The main presenting features were bone pain (55.17%, 22/40), fatigue (45.45%, 15/33), peripheral edema (21%, 8/38), extramedullary plasmacytomas (20%, 8/40), neurological complaints (20.5%, 8/39), infections (12%, 5/40), or renal dysfunction (58.06%, 22/38). The baseline characteristics of the patients are described in Table 1. The median duration between onset and diagnosis was 122 days (range 15–1503, mean 269.93 ± 382.92 days, 95% CI 131.87–407.99). Organomegaly was seen in 28% [hepatomegaly was present in 27% (11/40), splenomegaly in 12.5% (5/40), and lymphadenopathy in 3.03% (1/33)]. The performance status of the patients was good, evident by only 25% having Eastern Cooperative Oncology Group (ECOG) ≥2. On evaluation of patients at the time of diagnosis, hypercalcemia (corrected calcium >11 mg/dL), renal impairment (estimated glomerular filtration rate [eGFR] <60 mL/min/1.73 m2), anemia (Hb <10 g/dL), and lytic lesions were seen in 24.32% (9/37), 30% (12/40), 52.5% (21/40), and 59.25% (16/37) of AYA-MM patients, respectively.
BM, bone marrow; ESR, erythrocyte sedimentation rate; LDH, lactate dehydrogenase; PO, serum phosphate level.
Of the 37 evaluable patients, on the skeletal survey, 44.44% (12) of patients had multiple lytic lesions, 14.81% (4) of patients had a single lytic lesion, and 40.74% (11) of patients had no lytic lesions. On serum-free light chain assay, 76.9% (30/39) of patients had an abnormal ratio. On urine analysis, Bence Jones proteinuria was present in 46.15% (6) and urinary M protein was present in 31.82% (7) of the evaluable patients (n = 13). Amyloid was detected on fat pad biopsy in two of the nine evaluable patients (22.22%). On risk stratification, 12.5% (5), 17.5% (7), and 70% (28) of patients were in ISS-I, -II, and -III, respectively. The extramedullary disease was found at diagnosis in 15% (6/40) and during the disease course in 28.2% (11/39). Of the 39 evaluable cases, the different types of myeloma have been depicted in Figure 1. Of all AYA patients, autologous stem cell transplant was done in only 22.5% (9). Other patients were managed with chemotherapy even after remission induction due to financial limitations (77.5%, n = 31). The 3-year OS of the study population was 80.21% (Fig. 2), whereas among the transplant patients 3-year survival was 85.71%. The 1-, 2-, and 3-year survivals of the stage III disease are 92.96%, 82.74%, and 73.71%, respectively, the same could not be calculated for the stage I and stage II disease due to the small sample size (Fig. 3).
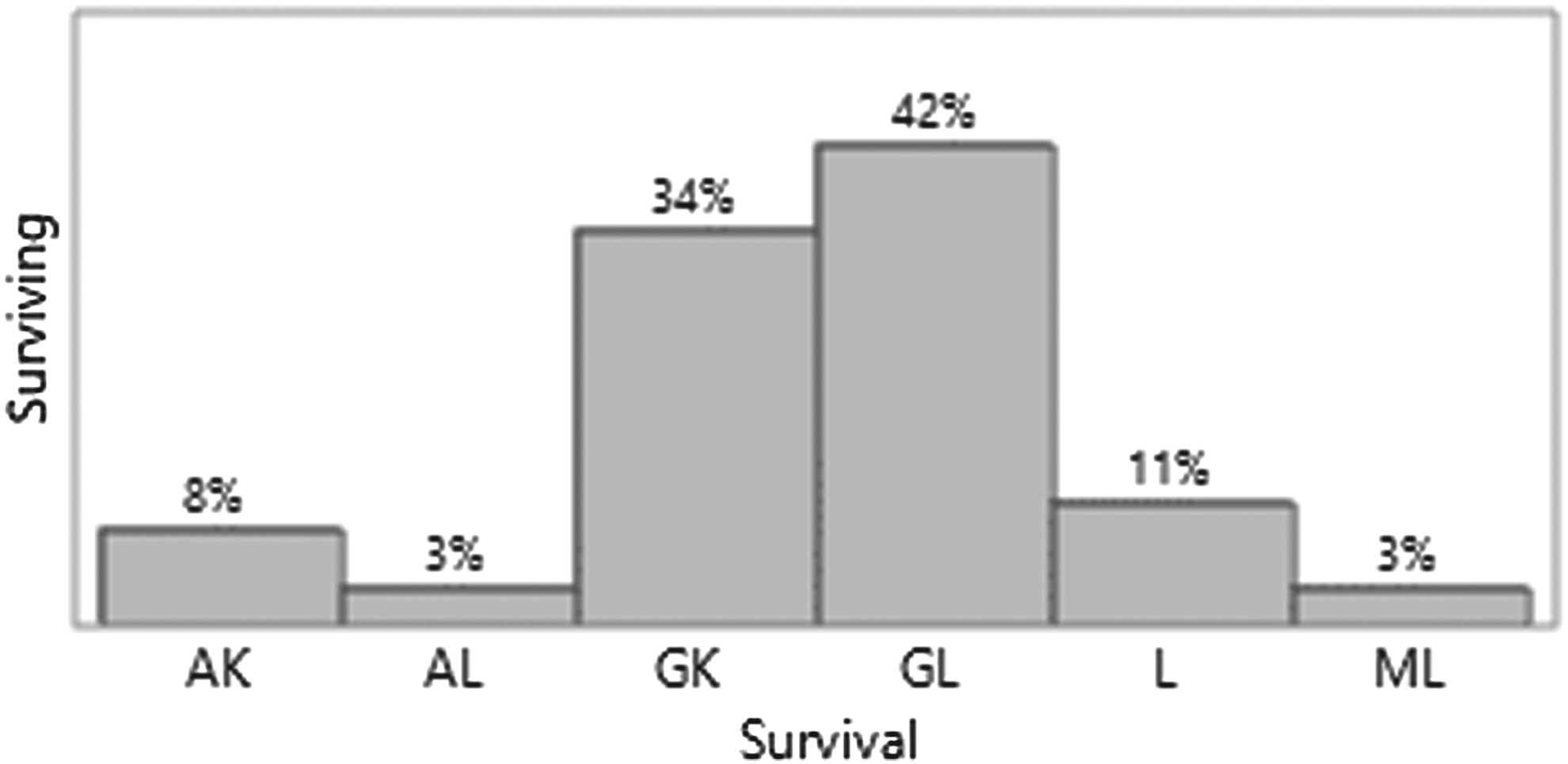
Histogram showing the proportion of different myeloma types (AL, IgA Lambda; AK, IgA Kappa; GL, IgG Lambda; GK, IgG Kappa; L, Lambda; ML, IgM Lambda).
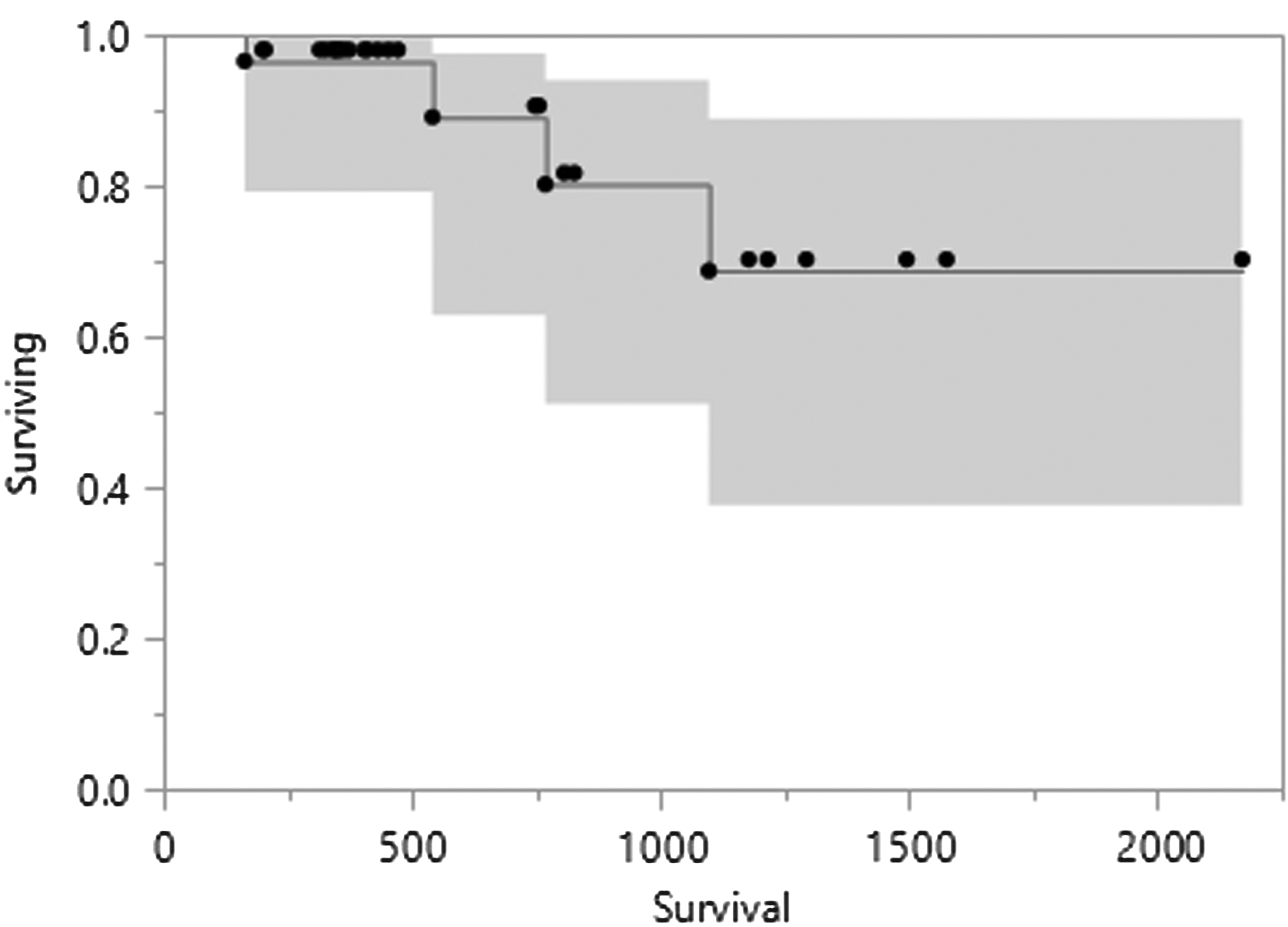
Kaplan–Meier curve showing the survival of the AYA-MM patients with the shaded area showing the 95% CI. AYA, adolescents and young adult; CI, confidence interval; MM, multiple myeloma.

Kaplan–Meier curve showing the survival of different ISS stages (stage I, stage II, and stage III) of the AYA-MM patients with the dotted line depicting the survival of the complete cohort. ISS, International Staging System; OS, overall survival.
Discussion
Studies on clinical differences, therapeutic response, and outcomes of MM in the younger age group are considerably limited. Being primarily a disease of the elderly, only 2% cases of MM occur under the age of 40 years and only 0.3% under the age of 30 years.14–17 Age is inversely correlated with survival and therefore has been recognized as an important prognostic factor. Age also critically influences treatment options, such as high-dose therapy and/or bone marrow transplantation.24,25 Also, it is an unresolved question whether or not MM in young patients is an independent biological entity or just one end of the disease spectrum. In our study, the incidence is close to 10%. This higher incidence can be partially attributed to a decade earlier age of onset of MM compared to the west, 26 but the same may not be a true reflection of the real-world incidence as this hospital-based study is subject to referral bias.
AYA may have an atypical presentation with a more indolent course and a longer survival. Sagaster et al. studied 250 MM patients in three age groups classifying them as group A (<45 years), group B (45–70 years), and group C (>70 years). 17 The three groups showed no statistically significant difference in the laboratory and clinical findings. Equal distribution of immunoglobulin subtypes and light chain paraprotein was also noted in three groups. There is not much statistical difference in the three groups in relation to 14q translocation plus del13q14 pattern. In our setting, evaluation for chromosomal abnormalities is not routinely done due to financial constraints and lack of standardized testing by laboratories. Median OS in group A patients in ISS-I and -II was not reached, whereas in ISS-III, it was 23.4 months, 24.6 months in group B/stage III, and 32 months in group C/stage III. The stages and their prognosis were also studied. There was a greater disparity in survival between ISS stage I/II and stage III in the first group (<45 years) with median survival not reached in stage I/II and 23.4 months in stage III. This difference was not present in the elderly group (group C) with a median survival of 39.6 months in stage I/II and 32 months in stage III. Shorter survival of group A (younger age) stage III patients was independent of abnormal cytogenetic/molecular patterns. In our study cohort, there was a preponderance of stage III patients probably due to the late presentation of our clientele. Our results are akin to those by Sagaster et al., in which the survival of the stage III patients was inferior to the stage I/II patients and the 3-year OS in stage III disease was 73.71%.
Blade et al. studied patients with MM in the younger than 30-year age group. 16 They evaluated 10 patients (6 males, 4 females) in the period from 1956 to 1992. Six patients had no extramedullary involvement, three had serum creatinine >2 mg/dL, and increased serum calcium of >12 mg/dL was seen in three patients. Most of the patients in this study had the high-risk disease, six patients with stage II, and the rest with stage III disease, as in our cohort. Five patients with Bence Jones myeloma had median light chain protein in the urine, 3.8 g/dL (0.3–12.2). The median survival of these patients was 87 months. In another study, Blade and Kyle included 4081 patients of whom 3% were younger than 40 years. 18 They studied that the initial clinical signs and symptoms were similar to the other age groups in the series. One-third of the AYA patients had light chain myeloma, whereas 6% had IgD disease, which was not found in our cohort (light chain myeloma constituting only 11%). Conventional treatment at younger age leads to 54% objective response. The median survival was 4.5 years in young patients. Young patients with low β2 microglobulin and normal renal function had a median survival of 8 years.
The literature on the demographic and survival details of AYA-MM from India is limited. 27 Table 2 summarizes the other important studies on MM in AYA. Guidelines on the management of AYA-MM are scarce.18,28 These guidelines suggest autologous stem cell transplant (ASCT) as the preferred treatment choice with both OS and progression free survival (PFS) benefit in this age group. This benefit was also noted in our study, in which was the 3-year OS in patients who underwent transplant versus the complete cohort (85.71% vs. 80.71%), but only 22.5% of the patients could be taken up for transplant due to financial constraints.
NR, not reported; OS, overall survival; PFS, progression free survival.
This is a retrospective study and all the limitations of a retrospective study also apply to our study. The major limitations include recall bias and nonavailability of clinicopathological details of all the patients. Despite all the limitations, this is the first effort from the real-world settings to identify the clinicopathological profile and outcomes of the AYA-MM patients.
Footnotes
Acknowledgments
We acknowledge Dr. Kamal Kant Sahu (previously Resident PGIMER), the hematopathology department, and all our patients.
Author Disclosure Statement
No competing financial interests exist.