
Abstract
Purpose:
This study focused on self-perceived mate value of young adult survivors of childhood cancer relative to healthy peers. Qualitative studies indicate potential problems surrounding romantic relationships among survivors, but systematic studies are missing.
Methods:
One-hundred forty-nine childhood cancer survivors and 149 matched controls completed online questionnaires about their mate value, social comparison strategies (i.e., upward/downward identifying/contrasting strategies), and marital status. Survivors and controls were aged 20–40 (M = 27.8), 55% were female, and survivors had been treated for brain tumors (n = 52; 35%), leukemia (n = 42; 28%), lymphoma (n = 31; 21%), or other solid tumors (n = 24; 16%) at 5–33 years before study participation.
Results:
Survivors and controls did not differ on overall mate value, but on individual characteristics: Survivors thought they had a better sense of humor (d = 0.36), were more loyal (d = 0.32), had higher social status (d = 0.26), and were more ambitious (d = 0.19), while also considering themselves less sexually adventurous (d = 0.31), less healthy (d = 0.26), having less desire to have children (d = 0.21), and a less attractive face (d = 0.20). Higher mate value was related to being partnered, more upward-identifying, less upward-contrasting, and less downward-identifying strategies. Moreover, less downward-identifying was associated with higher mate value in survivors, but not controls; whereas greater downward-contrasting was associated with higher mate value among controls only (R2 = 30.8%).
Conclusions:
Survivors do not generally view themselves as less valuable (potential) romantic partners, but they evaluate different characteristics either more positively or more negatively. Social comparison strategies offer targetable points of interventions to intervene on negative self-evaluations, potentially enhancing well-being.
Introduction
B
Qualitative studies illustrated that adult survivors of childhood cancer express beliefs that others might not want to date them, 3 and that late effects such as infertility impede romantic relationships.4–7 Survivors also express concerns about being pitied or perceived as weak,3,4,8 or that potential partners could find the physical reminders of cancer (e.g., scars) unattractive.3,8 Thus, survivors' self-consciousness3,4 and fears of rejection 9 can hinder forming intimate relationships, and even after survivors successfully initiate relationships, they often worry about dissolutions. 10 In contrast, some of these qualitative studies also indicated that survivors feel more mature, stronger, and more resilient than their peers after having overcome cancer,4,7–10 leading them to think of their relationships as deeper/more meaningful. Thus, survivors may evaluate themselves both more negatively and positively than their peers on various aspects of mate value.
Self-perceived mate value is influenced by social norms, and humans have a tendency to compare themselves with others to evaluate themselves and their situation. 11 Such social comparisons are made to targets (i.e., other people) that are either doing better (i.e., upward target) or worse (i.e., downward target) on various characteristics. When people compare themselves with these upward/downward targets, they either identify with or contrast themselves. The combination of target and type of comparison results in four different social comparison strategies11,12 (see the Methods section for a more thorough description) that could lead to either more positive or negative self-evaluations. No study has evaluated social comparison strategies and mate value among cancer survivors, but based on the qualitative findings described earlier, survivors may be more likely to use upward-contrasting (e.g., not feeling good enough, being more sick, or unemployed/financially dependent)4,7,13–18 and, therefore, report lower self-perceived mate value than their healthy peers. Alternatively, they may evaluate themselves more positively (e.g., more mature, stronger, resilient),4,7–10 while using downward-contrasting strategies. Overall, childhood cancer survivors may consider themselves both ahead of and behind their peers in different domains3–5,9,19 and, consequently, adopt an attitude of feeling different, thus using more contrasting strategies (both upward and downward).
Note that studies on social comparison strategies among cancer populations have focused on either belonging (e.g., adolescent cancer patients at a camp felt more similar to other campers than their peers at home) 20 or the use of social comparisons as a form of coping (e.g., adult patients judged their prognosis relative to others with cancer). 12 Only studies among healthy people have linked social comparison strategies and mate value. For example, exposing individuals to others with high physical attractiveness (i.e., upward targets) lowered the estimates of their own physical attractiveness.21,22 This finding also underscores the potential role of social comparisons and mate value in establishing intimate encounters/relationships, but studies among cancer survivors are lacking.
In addition, there are sociodemographic and/or disease-specific factors that should be considered. First, self-perceived mate value and social comparisons are cognitive processes, for which childhood cancer survivors may be less equipped. Numerous childhood cancer survivors receive intense treatment that is directed to the central nervous system and experience deficits in neurocognitive functioning (e.g., lowered processing speed, attention, intelligence).23–29 This may not only make survivors less attractive mates, in general, but could also impair their capacity to self-evaluate, 30 such that they may not realize that they are reacting/behaving differently from their peers. This lack of awareness, however, might be protective for survivors, especially those treated with intense neurotoxic treatments. For example, young brain tumor survivors were found to have poor peer relationships according to their classmates but did not according to self-report. 31 Second, marital status seems to be related to mate value: Unsuccessful dating/rejections were related to lower mate value and to beliefs of never getting married among healthy people, whereas being partnered/married served as a cue for higher mate value.32–35 Thus, marital status and neurotoxic treatment intensity are likely important factors in survivors' appraisals of their own mate value.
In this study, we examined whether young adult survivors of childhood cancer reported different mate value than controls (taking marital status into account). Given diverse qualitative findings, survivors may be likely to rate certain mate value characteristics more positively and others more negatively, which may differ by the extent of neurotoxic treatment. We further examined social comparison strategies, hypothesizing that survivors would be more likely to contrast themselves. Finally, we tested whether such differences in social comparisons were related to mate value.
Methods
Participants and procedure
Adult survivors of childhood cancer who were treated at Nationwide Children's Hospital were eligible if they were young adults (aged 20–40), 36 diagnosed with a malignancy between ages 5 and 18, and were ≥5 years post-diagnosis. Eligible survivors were identified through the hospital's registry or long-term follow-up clinic and were sent an invitation letter with a web link to complete the survey online. Participants provided informed consent online before proceeding to the survey. Survivors who did not participate within 2 weeks were reminded by phone. Completers were compensated for their participation, and this study was approved by the Institutional Review Boards of Nationwide Children's Hospital and the University of Groningen.
Childhood cancer survivors
Invitation letters were mailed to 539 survivors, but 119 had incorrect contact information (i.e., N = 420). Another 186 survivors had incorrect phone numbers (identified during the reminder procedure) and may have had outdated addresses too. Therefore, 243–420 survivors potentially received our invitation, 173 survivors started the survey (response rate = 74%–41%), and 166 completed it (completion rate = 96%). Seventeen participants were subsequently excluded, due to skipped/contradictory answers (n = 7), or errors in the patient registry deeming survivors ineligible after a complete medical chart review (n = 10).
The final sample (N = 149) was 55% female (n = 82) and 91% Caucasian (n = 135). They were aged 20–40 (M = 27.8, SD = 5.3) at study participation, diagnosed at age 5–18 (M = 11.7, SD = 3.8), and 5–34 years post-diagnosis (M = 16.2, SD = 6.4). Diagnoses included brain tumors (n = 52, 35%), leukemia (n = 42, 28%), lymphoma (n = 31, 21%), and other solid tumors (n = 24, 16%). Two thirds (n = 92, 62%) of survivors were partnered (in a relationship/married), whereas 38% (n = 57) were single.
The extent of neurotoxic treatment intensity was coded based on a previously developed rating that takes into account dosages of cranial radiation, intrathecal chemotherapy, and certain intravenous chemotherapy drugs. 37 Medical records were reviewed and survivors were grouped into having received non-neurotoxic treatments (n = 49, 33%), low-dose treatments (n = 36, 24%), or high-dose treatments (n = 62, 42%; n = 2 had missing medical records).
Controls
U.S. residents were invited to participate in an online survey through Survey Sampling International, a company specializing in online survey data collection. Four hundred individuals aged 20–40 without a previous or current cancer diagnosis were recruited. From this pool, we matched one control to each survivor based on gender, age, and race (N = 149). After matching, we compared both groups on other demographic factors (i.e., relationship status, living situation, level of education, occupational status, and annual income) and found both groups to be comparable (all p's>0.14).
Measures
Mate value
Participants completed the Mate Value Inventory, 1 assessing 17 characteristics relevant to a person's mate value (e.g., ambitious, good body, good sense of humor, independent, loyal, responsible, financial resources, stable personality, etc.) on a scale from 0 to 10 (low–high) to indicate to what extent each characteristic applied to them. Items were averaged to create an overall mate value score (0–10), and reliability analyses showed very good results with Cronbach's alpha (α) = 0.88.
Social comparison strategies
Tendencies to use upward/downward identifying/contrasting comparison strategies were measured with the Social Comparison Strategies scale. 12 It assesses four different styles: upward-identifying (i.e., relating to positive characteristics in other people and identifying them in oneself), downward-identifying (i.e., relating to worse aspects in others and concluding to be similar), upward-contrasting (i.e., identifying characteristics in others and concluding that one does not meet these standards), and downward-contrasting (i.e., identifying worse aspects in others and concluding that one is doing better). Twelve generic items measure these four strategies, such as When I see others who are doing better than me, I am happy to think I can improve as well (i.e., upward-identifying), When I see others who are worse off than me, I get quite scared that my situation will deteriorate as well (i.e., downward-identifying), When I think about others who are doing better than me, I feel frustrated about my own situation (i.e., upward-contrasting), or When I meet others who are worse off than me, I realize that I am actually doing quite well (i.e., downward-contrasting). Items are answered on a 5-point scale (not at all–very much), and Cronbach's α ranged between 0.81 (upward-identifying) and 0.87 (upward-contrasting).
Statistical analyses
Descriptive statistics are presented accompanied by Cohen's d effect sizes. To test both differences on average mate value and separate mate value characteristics, we ran an ANOVA (overall mate value) and MANOVA (mate value characteristics). We used cancer status (survivor vs. control) and marital status (single vs. partnered), as well as their interaction as factors. Differences on mate value by neurotoxicity subgroups were tested similarly with an ANOVA and MANOVA among survivors only. We further compared all social comparison strategies between survivors and controls in another MANOVA. Finally, we tested the relative contribution of social comparison strategies to mate value in a stepwise linear regression. Step 1 included cancer (survivors vs. control) and marital status (single vs. partnered), Step 2 included the four social comparison strategies, and Step 3 included interaction terms of all comparison strategies with cancer status. Power analyses indicated ample power (>0.8) to detect at least moderate differences between survivors and controls and to conduct our proposed regression analysis. Power for subgroup comparisons among survivors was limited (>0.6).
Results
Mate value
Childhood cancer survivors reported similar mate value to controls (d = 0.07; Table 1), but groups differed on 8 out of 17 mate value characteristics: Survivors thought of themselves as having a better sense of humor (d = 0.36), being more loyal (d = 0.32), having higher social status (d = 0.26), and being more ambitious (d = 0.19), whereas they also considered themselves less sexually adventurous (d = 0.31), less healthy (d = 0.26), having less desire to have children (d = 0.21), and a less attractive face (d = 0.20; Table 1). However, all of these differences are considered small (d < 0.5).
Hotelling's trace: F = 5.44, p < 0.001; please note that men and women did not differ on overall mate value (F = 0.34, p = 0.559) and all mate value characteristics combined (Hotelling's trace: F = 1.723, p < 0.095), nor was an interaction between gender and cancer status significant. However, post hoc tests indicated that women reported slightly higher faithfulness (d = 0.26, p = 0.026) and lower sexual adventurousness (d = 0.31, p = 0.007).
p < 0.05.
p < 0.01.
Bold values represent significant F-tests.
Partnered individuals (n = 188) differed from singles (n = 110), such that partnered individuals reported higher overall mate value than singles (d = 0.54; Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/jayao) as well as higher scores on 11 out of 17 mate value characteristics: The biggest differences were found for the desire to have children (d = 0.70), being faithful (d = 0.48), or being sexually adventurous (d = 0.46; see Supplementary Table S1). Importantly, no interaction effects were found between cancer and marital status, indicating that partnered survivors (n = 92) and controls (n = 96), as well as single survivors (n = 57) and controls (n = 53) rated their mate value similarly.
Group comparisons among survivors stratified by neurotoxic treatment intensity (i.e., non-neurotoxic, low-dose, or high-dose) showed no group differences regarding overall mate value (F = 1.496, p = 0.227, means ranged between 7.3 and 7.7). However, one difference was found among all 17 mate value characteristics: Survivors in the high-dose neurotoxic group reported a significantly lower desire to have children (M = 5.8, SD = 3.5) than the low-dose (M = 7.7, SD = 2.9) and non-neurotoxic groups (M = 7.8, SD = 2.9; F = 7.15, p = 0.001), with corresponding medium effects of d = 0.58 and 0.63, respectively. It should be noted that comparisons between diagnostic groups indicated that brain tumor survivors reported lower mate value than lymphoma as well as leukemia survivors (M = 6.9 vs. 7.7 and 7.8, p = 0.002), but subgroups were small.
Social comparisons
Childhood cancer survivors and controls differed on one of the four social comparison strategies: Survivors were less likely to use downward-identifying strategies (d = 0.30; Table 2), which is regarded as a strategy typically leading to negative self-evaluations. Among childhood cancer survivors, social comparison strategies did not differ between the non-neurotoxic, low-dose, and high-dose treatment groups.
Hotelling's trace: F = 2.166, p = 0.073.
p < 0.01.
Bold values represent significant F-tests.
Social comparison strategies and mate value
A stepwise linear regression tested the relative contribution of all comparison strategies to mate value. The final model (R2 = 30.8%; Table 3) suggested that being partnered (β = 0.211), more upward-identifying (β = 0.214), less upward-contrasting (β = −0.181), and less-downward identifying strategies (β = −0.287) were associated with higher self-perceived mate value. More importantly, two significant interactions emerged as well: Less downward-identifying was significantly associated with higher mate value in survivors, but not in controls; whereas greater downward-contrasting was associated with higher mate value among controls, but not survivors (Table 3; Figs. 1 and 2).
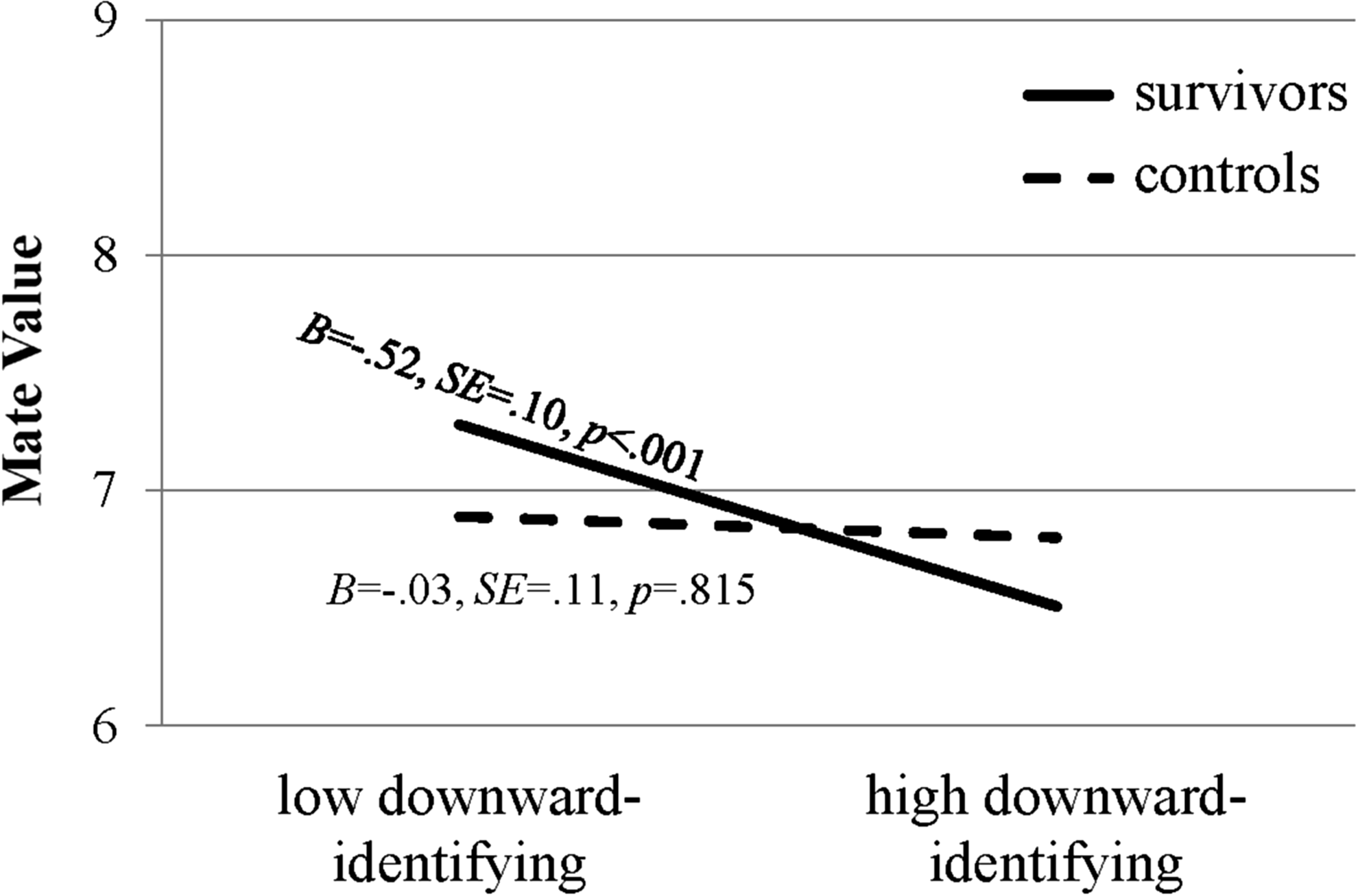
Testing simple slopes of the interaction effect of cancer status and downward-identifying on mate value.

Testing simple slopes of the interaction effect of cancer status by downward-contrasting on mate value.
The same regression analysis without relationship status yields the same results with R2 = 0.264 in the final model; ap < 0.01, bp < 0.05.
Discussion
This is the first study to systematically examine mate value among young adult survivors of childhood cancer. Survivors rated themselves both more positively and negatively on various mate value characteristics compared with their peers, whereas their overall mate value was similar. Differences on social comparison strategies only concerned survivors being less likely to use downward-identifying strategies, which was also associated with higher mate value among survivors, but not controls. In addition, factors such as being in a relationship and several social comparison strategies were related to mate value among both survivors and controls. However, many of the identified effects were rather small, and several aspects should be considered.
Most of the mate value characteristics that survivors rated higher than matched controls (i.e., loyal, social status, ambitious) go hand in hand with feelings of maturity and valuing life as reported in previous qualitative studies.4,7–10 At the same time, other negative self-evaluations reported in qualitative studies (e.g., worse health and physique)4,7,13–16 were also reflected in the mate value ratings (e.g., less healthy, less desire to have children, less attractive face). Interestingly, survivors previously reported feeling self-conscious about their appearance,3,4,7,14 but having a “good body” did not differ between survivors and controls in this study. Although some survivors, indeed, feel self-conscious, having been treated at a young age may also present many survivors with the opportunity to still “grow” into their (altered) bodies or integrate cancer-related alterations into their self-concept while growing up,19,38 and they, consequently, may not feel considerably more negative about their bodies than others. This might be an advantage over patients diagnosed with cancer in adulthood, a population in whom negative body issues are more commonly reported. 39
The survivors in this study also rated themselves as less sexually adventurous. It is possible that survivors interpreted this item as being promiscuous, which may not fit with views of being mature. Alternatively, survivors may, indeed, be less sexually adventurous due to certain health conditions/medical late effects (e.g., cardiovascular or musculoskeletal conditions), but this remains poorly understood. Overall, it was striking that higher scores on some mate value characteristics and lower scores on others leveled out to an overall similar mate value score relative to controls (M = 7.4/7.3). Although this should be regarded as positive, healthcare providers should pay attention to whether certain self-evaluations/characteristics may weigh heavily on survivors. It appeared that more negatively endorsed characteristics clustered around survivors' health/physique, whereas more positively evaluated characteristics were desirable personality characteristics.
Interestingly, subgroups of survivors divided by treatment neurotoxicity did not differ in their self-perceived mate value. However, it remains to be tested as to whether survivors may, indeed, be attractive mates or whether their self-perception is inaccurate. This also refers to a general problem surrounding self-perceived mate value: Self-perception does not necessarily align with “reality” or characteristics that are valued by others. Thus, survivors may not have difficulties in approaching potential partners, as they rate themselves similar to their peers, but it remains to be tested as to whether potential partners, in turn, evaluate survivors as worthy partners. In general, it is important that individuals can at least approximate their own mate value to be successful on the dating market (instead of, for example, overestimating their mate value and continuously being rejected by others). 35 Nevertheless, and regardless of accuracy, survivors judged only certain characteristics differently, which did not affect overall mate value relative to controls.
Contrary to our expectations, survivors were not more likely to use contrasting strategies than healthy controls; instead, survivors used less downward-identifying comparison strategies. This strategy is considered as potentially leading to more negative self-evaluations, and it is, therefore, positive that survivors do not commonly use this strategy. Interestingly, three out of the four social comparison strategies were associated with mate value in the expected directions, and more importantly, two interactions emerged as well: Less downward-identifying was associated with higher mate value in survivors, whereas more downward-contrasting was associated with higher mate value among controls only. Effects were rather small (Figs. 1 and 2), but the overall model explained almost one third of the variance in mate value scores. Even when relationship status was taken out of the regression analyses, the total variance explained was still 26%. This suggests that together, the four social comparison strategies could be highly important for mate value and may be excellent targets for interventions to improve self-perceptions. Previous research, utilizing social comparison strategies in educational materials to enhance coping among adults with cancer, has shown promising results 40 and may be helpful to childhood cancer survivors too.
Although this is the first study addressing mate value among adult survivors of childhood cancer, certain limitations should be considered. Overall, we had a rather large sample and ample power, but analyses among neurotoxicity subgroups had limited power to show differences, if present, and the sample lacked racial diversity. In addition, the actual mechanisms of whether social comparison strategies influence mate value remain to be tested, along with other potentially relevant factors (e.g., relationship history, occupation, additional cancer-specific aspects). Nevertheless, this study offers novel insights into differences in self-perceived mate value among childhood cancer survivors relative to matched controls. In addition, social comparison strategies (and relationship status) explained a substantial amount of variance in mate value, offering valuable points of intervention for survivors who may perceive themselves less favorably.
Future research might consider the importance of mate value and social comparison strategies in relation to other outcomes (e.g., self-esteem, well-being). Larger longitudinal studies are also needed to more comprehensively understand survivors' development. Healthcare providers should be attentive to both positive and negative self-evaluations and social/emotional functioning among survivors to provide comprehensive care and optimize survivors' quality of life.
Footnotes
Acknowledgments
This work was supported by an intramural grant from the Research Institute at Nationwide Children's Hospital (V.L.) and a grant from the Dutch Cancer Society (RUG2009-4442; M.A.T).
Disclaimer
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.