
Abstract
Aims:
The consequences of cancer and treatment on fertility can be a continuing source of distress for adolescents and young adults. The study aims were to assess the effects of bundled interventions on clinical practice concerning fertility in young people aged 14–25 years with cancer.
Methods:
Bundled interventions, including development of quality indicators, resources, and targeted education, were introduced during 2015 across five cancer centers. Data before interventions (2012–2014) were compared with data prospectively collected during 2015–2016. Relative risks (RR) with 95% confidence intervals (CI) were calculated to assess effects of interventions.
Results:
Compared with the pre-intervention cohort (n = 260), the post-intervention cohort (n = 216) was 1.47 times more likely to have documented discussion of risk of infertility (95% CI 1.12–1.63, p = <0.001). Similarly, documented referral to fertility specialists was more likely in the post-intervention cohort (RR 1.53, 95% CI 1.26–1.87, p = <0.001) as was documented fertility preservation outcomes (RR 2.56, 95% CI 1.91–3.44, p = <0.001). These differences were significant across age, gender, and diseases. Females had greater improvement in documented risk of infertility discussion between cohorts (RR 1.70, 95% CI 1.19–2.08, p = <0.001). Among diseases, the greatest improvements were seen in those with brain cancers (RR 2.15, 95% CI 1.28–3.62, p = 0.004) and soft tissue sarcoma (RR 2.60, 95% CI 1.17–5.78, p = 0.02).
Conclusions:
We have demonstrated the effects of bundled interventions to improve clinical practice associated with fertility preservation in young people with cancer. Interventions were successful for reducing disparities identified in the pre-intervention cohort associated with gender and certain diseases. Assessment of the quality of patient care is not possible without accurate, consistent documentation.
Introduction
W
During adolescence and young adulthood, clinicians may be uncertain about how involved young people should be in treatment decisions, and clinicians report discomfort with discussing the potential effects of treatment on fertility. 12 Moreover, research demonstrates disparities with gender and age, and male and older patients are reported to receive more information compared to female and younger patients. 12 As a result, young people may not receive appropriate information and they describe feeling distressed and confused about the potential consequences of cancer treatment on their fertility.10,14,15 While disparities between gender and age are well described, little is understood regarding differences due to diagnosis and whether this is an important factor. 12
From the clinician's perspective, there can be medico-legal consequences if patients feel they have received inadequate information. In 2014, there was successful action against a health service for failing to provide information regarding options for fertility preservation to a 14-year-old male before treatment. 16 In this case, some 6 years after treatment completion, the patient's action against the health service was successful, and the health service was found to have “breached consumer rights for failing to have adequate mechanisms in place to ensure the provision of fertility information and treatment options to consumers prior to undertaking chemotherapy treatment.” 16
For these reasons, the risk of infertility discussions should be clearly documented in the patient medical notes as a record of discussion between patient and clinician. The discussion and subsequent documentation provide important information about adolescent and young adult (AYA) understanding of the process, support received by health professionals, and other sources of information provided. 17 Including correspondence from the patient's general practitioner can facilitate appropriate follow-up of anticipated reproductive or sexual dysfunction concerns following treatment. This information is particularly useful to inform future family planning discussions between patients and clinicians.
The aim of this study was to investigate the effects of a bundle of interventions (described below) on the clinical practice of documenting risk of infertility discussion, referral for fertility preservation, and outcomes of fertility preservation in young people aged 14–25 years undergoing cancer treatment. Secondary aims were to explore the variables associated with variation in practice regarding fertility preservation.
Methods
Setting
The Youth Cancer Service (YCS) in Queensland, Australia, is a state-wide partnership model based across five tertiary cancer centers in the state. The Queensland YCS advocates all young people with a cancer diagnosis have access to verbal and written information regarding risks of infertility, and that fertility preservation options should be available to patients where clinically possible. Bundled interventions were introduced during 2015 across these five cancer centers. Data before interventions (2012–2014) were compared with data prospectively collected during 2015–2016.
Pre-intervention cohort
To collect data before interventions, we undertook a retrospective medical record audit of AYA patients aged 14–25 years at the time of a cancer diagnosis during the years 2012–2014. A list of patients from each of the five cancer centers was obtained using ICD-10 codes for a cancer diagnosis associated with a hospital admission during the study period (2012–2014). All patients identified in the list were reviewed for eligibility for inclusion in the audit. Patients were included if they presented with a secondary cancer following a childhood cancer diagnosis, but excluded if they had relapsed disease that had been treated in the previous 5 years. Patients with a diagnosis of localized melanoma or in situ carcinoma, such (e.g., thyroid cancer) where systemic treatment was not required, were also excluded from the study because there was no risk to fertility; these patients were also less likely to have been referred to YCSs.
The audits were undertaken at the five cancer centers associated with the YCS in Queensland, Australia. One hospital is a tertiary pediatric cancer center in metropolitan Brisbane, two hospitals are tertiary adult cancer centers also located in Brisbane, and the remaining two hospitals are adult cancer centers located in large regional centers. During the year 2013, three facilities moved to electronic medical records and patient paper medical records were archived. Because of costs and time constraints, where patient medical records were not readily available for auditing, they were excluded from the study.
Instruments
An audit tool was developed by the research team to extract data from the paper based or electronic medical record. Items included the following: patient demographics; age at diagnosis; diagnosis; treatment received; documented evidence of risk of infertility discussion; referral to fertility specialists; documented evidence of fertility preservation; and details of fertility preservation efforts. Study coordinators at each site were trained to use the tool. The first 3 months of clinical notes following diagnosis, correspondence between service providers, and chemotherapy administration sections of medical records were reviewed by study coordinators. Data were extracted and entered into a research database at each site by the study coordinators and then collated for analysis.
Interventions
Interventions to improve clinical practice of documented risk of infertility discussion and subsequent referral for fertility preservation consisted of multiple processes that were introduced during 2015 (Box 1).
Interventions
• Establishment of quality indicators for youth cancer fertility, prospectively collected and entered into web-based data system (QOOL) for all patients referred to YCS
• Delivery of targeted education sessions for medical and senior nursing clinicians
• Provision of gender-specific patient resource packs to newly diagnosed patients
• Development of fertility referral pathways, procedure, and work instruction forms
Quality indicators
At the commencement of 2015, performance metrics regarding fertility, as well as other indicators were included as part of YCS reporting. Collaboration with Queensland Cancer Control Analysis Team facilitated web-based data management of these indicators in a state-wide clinical database (Queensland Oncology OnLine [QOOL]) for all patients. Cancer care coordinators in each of the five partner sites were responsible for prospectively entering patient information in the QOOL database following presentation of patients at multidisciplinary meetings. Dated metrics concerning the following fertility indicators were collected for each patient referred to the YCS:
• Was the patient provided with written and verbal information regarding fertility preservation options? (Yes/No) • Was the patient referred to a fertility specialist? (Yes/No) • Did the patient undergo fertility preservation (Yes/No) • If Yes—what preservation method.
Targeted education
Interprofessional education sessions were based on a learning needs survey undertaken in 2013 with 107 health professionals across all sites. Topics included fertility and genetics, communicating with AYAs; sexuality, intimacy, and relationships; and fertility preservation methods for males and females. Education sessions consisted of a 30-minute presentation, provision of a fact sheet, resources including journal articles, websites, and a print out of the presentation, and discussion of referral pathways. Education sessions were repeated regularly and delivered across all sites in small targeted groups to over 80 health professionals during 2015–2016.
Patient resources
One of the barriers identified in the learning needs survey was a lack of accessible resources regarding fertility for patients in the inpatient areas of the hospitals. While clinicians were aware that there were resources produced by various fertility and cancer support groups, not having these readily available prevented some clinicians from initiating discussions with a patient. Resource packs were therefore established for patients with gender-specific information and brochures for fertility specialist groups. These packs were distributed to patients by the cancer care coordinators.
Referral processes
Finally, referral pathways, procedures, and work instruction forms were developed. Previously, referral pathways had been rather informal; physicians may simply have telephoned a fertility specialist to make a referral or write a referral letter. It was observed, at times, that patients would not have all the required information when attending a specialist appointment. For example, a patient may not know the type and intensity or duration of planned treatment; unless this is included in the referral, the fertility specialist may need to seek further information. In addition, the referral form prompts clinicians to forward serology results regarding HIV, Hepatitis C and B, and Syphilis status. Anecdotally, there were instances of avoidable delays due to incomplete information being provided to the fertility specialists. Having processes for referral agreed upon and documented, formalized the process and raised awareness to ensure all relevant information was collected and passed onto fertility specialists.
Post-intervention cohort
Prospectively collected data post-intervention were retrieved on all patients entered into the QOOL database from the five cancer centers throughout 2015–2016. Dated quality indicators for fertility, as previously described, were collected.
These indicators were extracted from the QOOL database along with patient details regarding demographics, age at diagnosis, diagnosis, and treatment received. These data were used to evaluate the effects of the bundled interventions in the post-intervention cohort.
Data analysis
Diseases were classified according to the AYA Cancer Classification System. 18 Descriptive statistics were used to compare pre- and post-intervention patient cohorts for the following: age group (14–19 and 20–25 years); gender; cancer diagnosis; type of treatment; toxicity of treatment on gonads; documented risk of infertility discussion; and documented fertility preservation outcomes. To establish the toxicity of treatment on gonads, we reviewed the chemotherapy type and dose, as well as any systemic radiotherapy treatment received by each patient. These data were reviewed against Levine and Stern classification of effects of chemotherapy on sperm production or amenorrhea. 19 Accordingly, treatment was considered gonadotoxic if it was classified as a high or intermediate degree risk. Chi-square tests were used to calculate statistical significance of characteristic differences between pre- and post-intervention cohorts. Relative risks (RR) with 95% confidence intervals (CI) were then calculated between pre- and post-intervention cohorts to determine the difference between cohorts with (1) documented risk of infertility discussions, (2) referral to fertility specialists, and (3) outcomes of fertility preservation. Finally, overall influence of gender, age, and diagnosis on documented clinical practice regarding fertility was assessed in the post-intervention cohort.
Compliance with ethical standards
Human Research Ethics Committee approval was obtained before commencement of the study (HREC/14/QRCH/364). Wavier of consent was approved for this low- and negligible risk research. All procedures performed in this study were in accordance with the ethical standards of the National Health and Medical Research Council. 20
Results
Of the 352 patients identified in the pre-intervention phase, 260 records were eligible for inclusion; records were not available to be retrieved for 23 patients, and 69 records were excluded based on diseases not requiring systemic treatment affecting fertility (thyroid carcinoma n = 46, other in situ carcinoma n = 20, and melanoma n = 3). For the post-intervention cohort, data were reviewed for all 216 patients' records. Characteristics of both patient cohorts are presented in Table 1. Characteristics of both cohorts for proportions of age group, sex, and cancer diagnoses were comparable. Despite exclusion of diseases likely to require only localized treatment, there were significant differences between cohorts; patients in the pre-intervention cohort were more likely to be treated with surgery or localized radiotherapy and patients in the post-intervention cohort were more likely to be treated with chemotherapy or multimodal therapy (p = 0.006). However, the toxicity of treatment on gonads was comparable between pre- and post-intervention cohorts with 75% and 78%, respectively, receiving intermediate to high risk treatment potentially effecting fertility.
Outcomes
Compared to patients in the pre-intervention cohort, patients in the post-intervention cohort were significantly more likely to have: (a) evidence of risk of infertility discussion (RR 1.47, 95% CI 1.12–1.63 p = <0.001); (b) documented referral to fertility specialist (RR 1.53, 95% CI 1.26–1.87, p = <0.001); and (c) documented fertility preservation outcomes (RR 2.56, 95% CI 1.19–3.44, p = <0.001; Tables 2–4).
RR, relative risk; CI, confidence intervals.
Documented risk of infertility discussion
In the pre-intervention cohort, we noted patients with lymphoma were the most likely (80%) to have documented risk of infertility discussion and patients diagnosed with soft tissue sarcoma were the least likely (28%). These findings were not associated with individual clinicians, teams, or facilities; patients with both lymphoma and soft tissue sarcoma were represented across the five study facilities. In post-intervention, a significant improvement in documented risk of fertility discussion was observed across all patient variables in both age groups, both males and females, and in all diseases except lymphoma (Table 2). Because patients with lymphoma in the pre-intervention cohort already had high documented risk of infertility discussion, the increase to 94% post-intervention was not statistically significant.
The greatest improvement for documented risk of infertility discussion occurred in females (RR 1.7, 95% CI 1.39–2.08, p = <0.001) and in patients with brain cancer (RR 2.15, 95% CI 1.28–3.62, p = 0.004) and soft tissue sarcoma (RR 2.60, 95% CI 1.17–5.78, p = 0.02).
Documented referral to fertility specialist
The number of documented referrals to fertility specialist also improved significantly post-intervention across both age groups and for both males (RR 1.44, 95% CI 1.17–1.77, p = 0.004) and females (RR 1.82, 95% CI 1.15–2.89, p = 0.01). Significant differences for this outcome were associated only with patients diagnosed with bone sarcoma (RR 1.84, 95% CI 1.12–3.01, p = 0.015) and carcinoma (RR 2.37, 95% CI 1.15–4.88, p = 0.019) (Table 3).
Documented fertility preservation outcomes
Similarly, there were significant differences pre- and post-intervention in patients who underwent fertility preservation; both age groups and both males (RR 2.89, 95% CI 2.05–4.09, p = <0.001) and females (RR 1.9, 95% CI 1.08–3.33, p = 0.025) were significantly more likely to undergo fertility preservation in the post-intervention cohort. Significant differences between diseases post-intervention were noted for documented fertility preservation outcomes in patients with bone sarcoma (RR 3.08, 95% CI 1.32–7.18, p = 0.009) and germ cell tumor (RR 2.71, 95% CI 1.37–5.38, p = 0.004) (Table 4).
Influence of age, gender, and disease on fertility preservation practices in post-intervention cohort
Data for the post-intervention cohort were analyzed to assess the influence of variables associated with the three outcomes of: documented risk of infertility discussion; referral to fertility specialist; and fertility preservation (Table 5).
Fourteen to 19 compared to 20–25 years, males compared to females, each disease compared to sum of all other diseases.
Age
As observed in the pre-intervention cohort, there were no significant differences associated with age categories for documented risk of infertility discussion or referral to fertility specialists; patients aged 14–19 years were comparable to patients aged 20–25 years. However, those aged 14–19 were 0.50 (95% CI 0.35–0.72, p = 0.002) times as likely compared to those aged 20–25 years to have documented outcomes of fertility preservation.
Gender
There were significant differences associated with gender. Compared to females, in the pre-intervention cohort, males were more likely to have documented risk of infertility discussion (RR 1.37, 95% CI 1.11–1.68, p = 0.003). This disparity closed in the post-intervention cohort with no significant differences identified between males and females post-intervention (RR 1.04, 95% CI 0.95–1.15, p = 0.37) for documented risk of infertility discussion. However, compared to females, males were still significantly more likely to be referred to fertility specialists (RR 1.83, 95% CI 1.37–2.46, p = 0.001), and to have documented fertility preservation outcomes (RR 2.06, 95% CI 1.44–2.96, p = 0.001).
Disease
In the post-intervention cohort, the only disease with significantly different likelihood of documented discussion was germ cell tumors (RR 1.10, 95% CI 1.01–1.20, p = 0.03). Documented risk of infertility discussion was otherwise comparable across other disease groups. Differences were noted in regard to referral to fertility specialists; patients diagnosed with acute leukemia were less likely to be referred (RR 0.59, 95% CI 0.38–0.92, p = 0.02) and those diagnosed with lymphoma and bone sarcomas were significantly more likely to be referred (RR 1.29, 95% CI 1.02–1.63, p = 0.03 and RR 1.47, 95% CI 1.15–1.87, p = 0.002, respectively). No differences were found with documented fertility preservation outcomes associated with disease.
The documented types of fertility preservation undertaken are presented in Figure 1. There were noticeable differences between years pre-intervention 2012–2014 and post-intervention 2015–2016, particularly in regard to oocyte or embryo preservation and documentation of patients declining preservation. Sperm cryopreservation was the most common preservation method for males. A number of patients underwent multiple methods, for example, combinations of oocyte/embryo cryopreservation and ovarian suppression.
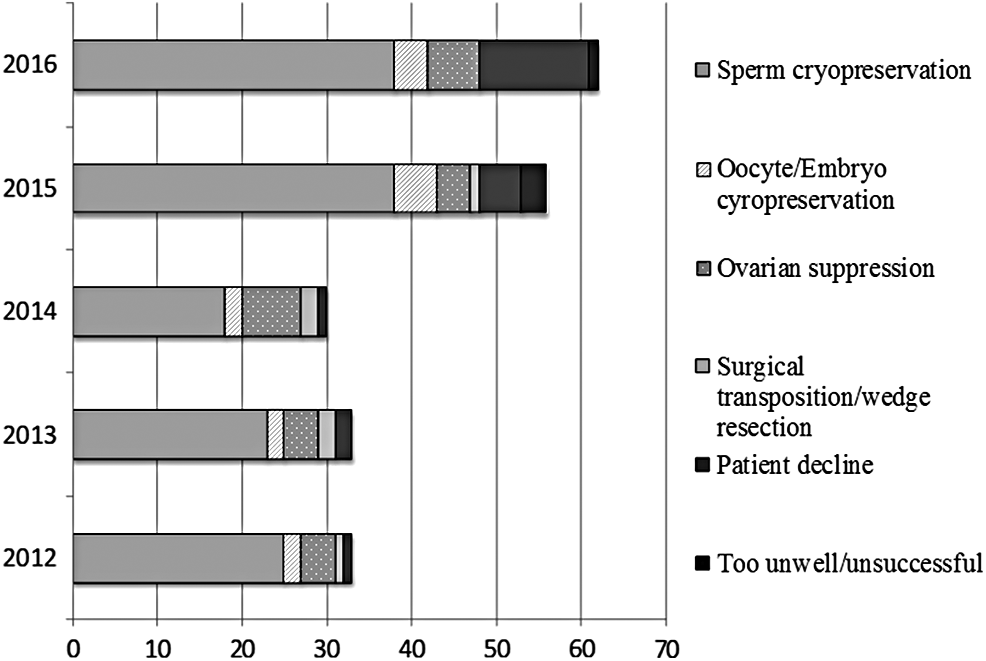
Documented outcomes of fertility preservation.
Discussion
To the best of our knowledge, this is the first multicenter study examining the effects of bundled interventions on documentation for risk of infertility discussion, fertility referral, and fertility preservation outcomes in AYA patients with cancer. The study-identified existing disparities between gender and disease were closed with the introduction of interventions that included the following: streamlined referral pathways, education focus on fertility, distribution of patient resources, and the recording of quality indicators for clinical practice with fertility. This study contributes new information regarding differences associated with gender, age, and disease, and adds to the small body of evidence regarding the clinical practice of risk of infertility discussion and interventions for fertility preservation in AYA cancer. 12
Unlike previous studies reporting clear disparities associated with age,21,22 we found no significant differences with documentation of risk of infertility discussion, or referral to fertility specialist associated with age in both the pre and the post-intervention cohort. Other studies have suggested that younger patients may not consider their fertility to the same extent as older patients, as it can be difficult to comprehend how fertility may impact upon their future lives.23,24 Current practice at the YCS affiliated pediatric hospital is to aim to discuss fertility issues openly with both the patients and parents in all cases. This is likely to have contributed to the documentation of such discussions in this facility, such that we found no differences between patients aged 14–19 years and those who were aged 20–25 years, who received treatment in adult cancer centers.
Similar to other reports in the literature,2,12 we found differences in both documentation of discussions, referral to fertility specialist and fertility preservation associated with gender, most noticeably in the pre-intervention cohort. While males were still more likely than females to have evidence of efforts made to preserve fertility, we were able to significantly reduce this disparity in the post-intervention cohort. These findings provide possible solutions to eliminate gender disparities with clinical practice, facilitating more equitable care to all young people, and may also assist with the development of clinical guidelines.
Gender differences in fertility preservation are likely a consequence of the technicalities of fertility preservation. In males, sperm banking is a relatively simple, noninvasive procedure, and the success rate of achieving a live pregnancy with cryopreserved sperm is high. In females, however, cryopreservation of oocytes is invasive, requires delay of treatment for at least 2 weeks, and a smaller proportion of oocytes survive the process of cryopreservation and thaw. 25 It is also worth noting that spermatogenesis takes ∼74 days, whereas females are born with their full complement of oocytes at birth. 26 These differences have made fertility preservation difficult in females. While there is increasing evidence of the potential for ovarian suppression and oocyte cryopreservation to be used in female fertility preservation, particularly in the pre-intervention cohort, these techniques were still considered experimental and not routinely advocated for.7,27 However, while these technicalities may account for gender differences in rates of fertility preservation, they should not affect rates of risk of infertility discussion.
We were able to improve documentation of risk of infertility discussions across all disease types. Patients with lymphoma were the only disease type where significant differences were not found; this may be explained by the already high rate of risk of infertility discussion in the pre-intervention cohort. The high proportions of patients with lymphomas, bone sarcomas, and germ cell tumors who went on to preserve fertility may be explained, in part, by having time to delay treatment. It is possible that other patients may have been too ill to have undergone preservation or the severity of disease necessitated immediate commencement of treatment. The clinician's objective in most cases is to make a professional judgment regarding urgency of treatment and assess the likelihood of successful preservation in an ill individual. It is well documented that spermatogenesis and the ability to ejaculate viable sperm are impaired when male patients are under stress. 28 It is conceivable that clinicians considered discussions regarding future fertility were not considered appropriate. It should also be noted that documentation does not always reflect actual practice. 29 In our pre-intervention cohort, there were five patients with lymphoma, treated with gonadotoxic treatment, who did not have a documented risk of infertility discussion, but who did have documented fertility preservation outcomes, in most instances confirmation of sperm cryopreservation. These findings were not replicated in other diseases; however, it is likely that rates of discussion were higher than rates of documentation.
The negative consequences of failing to provide patients with information have been documented in case studies. 16 The medico-legal risks justify the importance of this study and highlight the importance of completing and documenting a risk of infertility discussion, even if preservation is not carried out. However, it should also be considered that the outcomes of this study may be explained, in part, by the close juxtaposition between the legal case study in 2014 and our data collection before and after this time point. Clinicians may have had a heightened awareness of the potential for medico-legal consequences and thus have been more vigilant with documentation and clinical practice regarding risk of infertility in the post-intervention cohort.
Nevertheless, the potential for these issues to arise has recently been highlighted in systematic reviews that appraised the quality and recommendations of clinical practice guidelines around the world for fertility preservation in cancer patients. The authors observed variability, poor quality, and lack of uniformity across the guidelines and concluded these are likely to lead to conflicting recommendations and variation in clinical practice.12,30
The importance of the role of the clinician in discussions and decisions regarding fertility preservation cannot be underestimated. These discussions are highly significant for patients and parents. 22 Patients may be concerned about their fertility after cancer, regardless of the types of treatment received. 15 Patients want information regarding risks; referral to fertility specialists has been highlighted as contributing to lower regret and greater quality of life for patients after cancer treatment 3 and those who undergo fertility preservation believe they had made the right decision. 23
Our study identified significant improvement in documentation of clinical practice in relationship to fertility preservation, and anecdotally, we also found evidence of multiple patients achieving pregnancy after cancer treatment. An important aspect of fertility counseling should include the reassessment of fertility after treatment has completed. For males, this can include reassessment of sperm count and motility, and for women, a pre- and a post-treatment blood test of anti-mullerian hormone can provide an indication of ovarian function. 31
The issue of contraception is also important to consider; in this relatively small cohort of patients, two females became pregnant during treatment. Both women, one treated for Hodgkin lymphoma and the other for an osteosarcoma, chose to continue their pregnancies. However, the disease in both women was unable to be controlled and both died in the second trimester of pregnancy. The difficult ethical dilemmas faced by both clinicians and patients in these cases highlight the importance of considering all aspects of fertility during cancer treatment.
Limitations
The authors acknowledge the limitations of our findings due to the retrospective nature of pre-intervention cohort and reliance on medical records. In addition, our post-intervention cohort data were retrieved from QOOL, a state-wide clinical database, rather than the direct patient medical records; information in medical records may be different to that of the database. Nevertheless, our findings highlight the positive effects of relatively simple interventions to improve documentation of clinical practice. Further research is required to understand patient's health literacy of the risks of infertility due to cancer treatment and options for fertility preservation. While providing information is thought to be beneficial, little is known or understood about how this information is used by patients or if it is helpful. It is also not known if patients sought psychological support regarding fertility or if patients received fertility referral and specialist consultation in a timely manner.
Conclusion
With the high survival rates now achievable for many AYAs with cancer, issues such as fertility are increasingly important. We have demonstrated the success of a bundle of interventions aimed at improving documentation of clinical practice related to fertility in young cancer patients. For various reasons, detailed in our study, it is imperative that there is clear documentation of clinical discussions in patients' medical records. This ensures there is evidence that reflects the clinical advice and interventions provided to patients. To reduce variations in practice and improve quality of care, we recommend all cancer centers routinely record discussions regarding risk of infertility as a quality indicator. This study has not only provided a benchmark from which we can measure improvements but also stimulated clinicians across multiple cancer centers to reflect upon clinical practice and consider the importance of fertility for this population.
Footnotes
Acknowledgments
We acknowledge the support of the Queensland Youth Cancer Service (QYCS), which receives federal funding through CanTeen as well as state and territory government funding, provides specialist, age-appropriate treatment, and support for young cancer patients aged 15–25. We thank Glen Kennedy and Kirk Morris for their clinical advice, the QYCS Steering committee, and the clinical staff of the QYCS for their contributions in undertaking this study. We also thank Shoni Philpot and Danica Cossio from the Queensland Cancer Control Analysis Team for their support with data management for the QYCS.
Author Disclosure Statement
The authors state no competing financial interests exist.