
Abstract
Purpose:
Impairment of fertility is a common sequela of successful cancer treatment. Therefore, fertility preservation (FP) should be discussed with all young cancer patients. Decisions about FP are challenging. Patients wish more specific support and the first results concerning the helpfulness of decision aids (DA) were promising. Aside from describing the process of development and the content of an online DA in German, the objective of this study was to pilot test users' satisfaction with the DA and its effect on knowledge about FP and decisional conflict (DC).
Methods:
In this prospective consecutive study, a control group (n = 20, fertility counseling) was followed by and compared with an intervention group (n = 20, counseling and additional use of the DA, developed by an interdisciplinary team) of recently diagnosed female cancer patients between 18 and 40 years.
Results:
Nearly all participants who applied the DA considered it helpful for decision-making and recommendable. Knowledge about FP was high with regard to FP techniques women went for. DC was moderate according to the mean score (M = 27.92, standard deviation = 13.27) and only in 20%, the score was above the threshold for high DC. There was no difference between the control and intervention group for knowledge and DC.
Conclusion:
The DA seems to serve as additional and well-accepted support tool in decision-making for patients and professionals. Referral to a reproductive specialist is crucial to warrant comprehensive information. These results need to be confirmed with the current ongoing randomized controlled study.
Introduction
I
Previous studies have shown that fertility is an important issue for young female cancer patients.7–10 However, studies showed that only 34%–72% of patients were addressed with regard to fertility issues by their physicians11–15 and discussion about fertility often had to be initiated by patients themselves.16,17
The decision whether to opt for FP or not needs to be made in the short time frame right after cancer diagnosis and before the start of treatment. The situation, with which patients are confronted, is challenging, might evoke ethical dilemmas, and have a considerable psychological impact. 3 Several studies have shown that patients experience substantial decisional conflict (DC).8,18,19 Factors that may increase DC are uncertainty concerning the impact of the planned cancer treatment on future fertility, safety concerns, time constraints, and financial considerations, 19 as in Switzerland, Germany, and other countries, FP procedures have to be paid by the patient herself. However, previous studies showed that if patients had sufficient knowledge and their decisions were in accord with their personal values, it was more likely that they could make an informed choice.3,20–22
One way to support young cancer patients in this situation may be by providing decision aids (DAs), which are described as tools designed to support patients in healthcare decisions. They help patients understand potential risks and benefits of different options as well as embrace their personal values in the decision-making process. 23 According to a recent review, DAs are considered helpful instruments, especially when time for decision-making is limited. 24 A Cochrane review including 115 studies on DAs showed high-quality evidence that DAs compared to usual care are able to increase patients' knowledge and decrease their DC. 23 Particularly in the context of cancer, DAs are successful in encouraging patients to involve themselves in decision-making.24,25
To date, only two evaluated DAs about FP for young female patients with breast cancer are available, one in English and one in Dutch.26,27 Another DA in English for female patients with different types of cancer is currently under evaluation. 28
Based on our previous research in this field, our study team developed a web-based DA in German for young female patients affected by different types of cancer and considering the option of FP. The aim of the pilot study presented in this article was to evaluate the acceptability of the DA to make last modifications for the subsequent randomized controlled trial (RCT). Furthermore, we aimed at receiving first data on the current status of knowledge related to FP and DC of young female patients who had FP counseling shortly after having been confronted with their cancer diagnosis.
Materials and Methods
Development of the DA
The online DA was developed according to the International Patient Decision Aid Standards (IPDAS) 29 and by an interdisciplinary medical team consisting of oncologists, reproductive specialists, psychologists, and gynecologists. An online format was chosen because people nowadays frequently use the internet to gain information about health-related topics, including fertility.30–32 Online tools represent an ideal way of addressing young cancer patients to acquire information at any time and in any location.
The two already existing and evaluated DAs inspired the structure and parts of the content of the DA.33,34 During the development process, physicians from collaborating fertility centers and hospitals, as well as a nonclinical sample of female students (n = 17) were invited to use the DA and complete a short usability survey. Their feedback has been worked into the final version of the DA.
DA content
The DA aims at helping newly diagnosed young cancer patients (1) to better orientate themselves with regard to the effect of cancer on fertility and options to preserve fertility, (2) to clarify their priorities with regard to FP, and (3) to identify their specific needs. After using the DA, participants should know their priorities, be aware of the resulting options as well as the consequences, and have formulated the remaining questions they want to discuss with a specialist.
The DA is divided into an informative and an interactive part. The first part consists of background information about cancer and fertility in general, specific information about different cancer types, their treatments, and the possible impact on fertility. Moreover, the nowadays available options to preserve fertility are explained with regard to procedure, risks, costs, legal situation, and current scientific knowledge.
In the interactive part of the DA, value clarification exercises (VCE) are applied, which are key components of DA's to improve the decision-making experience. 35 VCE typically list benefits and harms of options and encourage individuals to value them. In this DA, women rated the listed benefits and disadvantages of each FP option they chose based on their personal factors with a 5-point scale from “not important at all” to “very important.” Patients could also add up to four additional personal arguments. In addition to the VCE, individuals were asked to indicate their gut feeling about each option they rated. The DA generates with all information together, a personalized summary of each FP option they worked on. Furthermore, the DA contains graphics, a notepad and literature, as well as webpage recommendations.
Study design
This study is a prospective consecutive intervention study, where the control group (fertility counseling) was followed and compared with an intervention group (fertility counseling and additional use of the online DA). The first 20 participants were assigned to the control group, while the DA was being developed. As soon as the DA was ready, the next 20 participants were assigned to the intervention group. The study was approved by the local ethics committee.
Recruitment and procedure
Eligible participants were female patients with a recent cancer diagnosis, who had to undergo a cancer treatment that potentially endangered their fertility. Further inclusion criteria were age between 18 and 40 years, German-speaking, and having access to a computer and the internet. Data were collected between July 2014 and June 2016. Five Swiss fertility centers/hospitals recruited participants from the beginning. To guarantee a sufficient sample size in due time, additional three German fertility centers/hospitals were included later and started recruiting only in the second recruitment phase. Patients were approached by a fertility specialist during their first counseling for FP. After signing an informed consent, the reproductive specialist provided the contact details to the study coordinator, from whom participants were contacted within 24 hours by email. Due to the consecutive study design, participants knew to which group they would be assigned. Women assigned to the control group received an online questionnaire at three time points, whereas participants in the intervention group received their individual link to the online DA at the start by email. After having applied the DA, they received identical online questionnaires in the same time setting as the control group. In addition, they were asked to answer three questions about their satisfaction with the DA. During the study, the DA was only accessible for study participants and will continue to be only available for study purposes until completion of the ongoing RCT.
Measures
Measures had to be completed right after counseling (T1) as well as 1 month later (T2), when a decision was expected to have been made, and 12 months after counseling (T3), when we expected women to be able to look back at their decisions. In this study, only data from T1 were used for analysis.
Demographics and cancer-related information
Data included age, marital status, nationality, parity, level of education, monthly income, and satisfaction about their financial situation. Information about cancer (diagnosis and planned therapy) was provided by their reproductive specialist. FP preference as well as their personal reasons for the decision (open-ended question) were assessed.
Knowledge about FP
Participants were asked whether they knew about seven particular FP options (cryopreservation of embryos, oocytes, ovarian tissue, or follicles with immature oocytes, in vitro maturation of oocytes, organ preserving surgery, and hormonal ovarian suppression during cancer treatment). The list of options included techniques that are well established (e.g., cryopreservation of embryos and oocytes), techniques that are still categorized as experimental, but where clinical experience is given (e.g., cryopreservation of ovarian tissue), other techniques that are entirely experimental (e.g., cryopreservation of follicles with immature oocytes), 4 but patients might nevertheless have had heard or read about, and techniques that are discussed controversially with regard to their benefit (e.g., hormonal ovarian suppression). 36
In addition, patients were asked to indicate their source of information (counseling, DA, and individual research) in case they knew about a particular option, and to answer two additional questions about the harmfulness and scientific state of the option. Finally, participants were asked to indicate their level of confidence about their fertility-related knowledge for every option they knew (5-point Likert scale with 1 = not sure at all to 5 = very sure).
Decisional conflict scale
The decisional conflict scale (DCS) was interpreted according to the official guidelines, in which the total score has been standardized and ranges from 0 to 100, with higher scores indicating a higher DC. 37 Scores >37.5 indicate high DC. At T1, participants answered only 12 out of the 16 items, as the last 4 items assume that the decision had already been made.
Satisfaction of the online DA
The intervention group answered three questions about satisfaction, helpfulness, and recommendation of the DA (“I'm overall satisfied with the online DA”/“I found the online DA to be helpful for making my decision”/“I would recommend the online DA to others”), rating them on a 5-point Likert Scale ranging from 1 (totally disagree) to 5 (absolutely agree).
Statistical analysis
Data were analyzed using SPSS 22.0 (Statistical Program for the Social Sciences) for Windows. All outcomes will be described using mean and standard deviation (SD) for continuous data and frequency for categorical data. Descriptive statistics were calculated to describe the sample with their demographic characteristics. Continuous data were analyzed by ANOVA, t-test, or Mann–Whitney U-test as appropriate. Categorical data were analyzed using Fisher's exact tests or chi square test. A two-tailed p value of <0.05 was considered statistically significant.
Results
Response rates and sample
Fifty-three women agreed to participate in this study, of which 24 were assigned for the control and 29 for the intervention group. Four participants in the control group and nine in the intervention group could not be included into further analysis because they never started the questionnaire or did not use the DA. Reasons for their nonparticipation are not known.
The final sample consists of 40 female cancer patients (n = 20 in each group) with a mean age of 29.23 (SD = 5.79). One patient was pregnant at the time of her diagnosis. As in most studies, breast cancer was predominant with 52.5% (21). 77.5% (31) of all participants stated to have already made a decision for or against FP. There were no significant differences between the control and the intervention group except for nationality (p < 0.001). This difference is due to the fact that fertility centers/hospitals from Germany were only involved in the recruitment process in the second study period with the DA. Table 1 shows detailed demographic and cancer-related data.
p < 0.05.
FP, fertility preservation; SD, standard deviation.
Knowledge (T1)
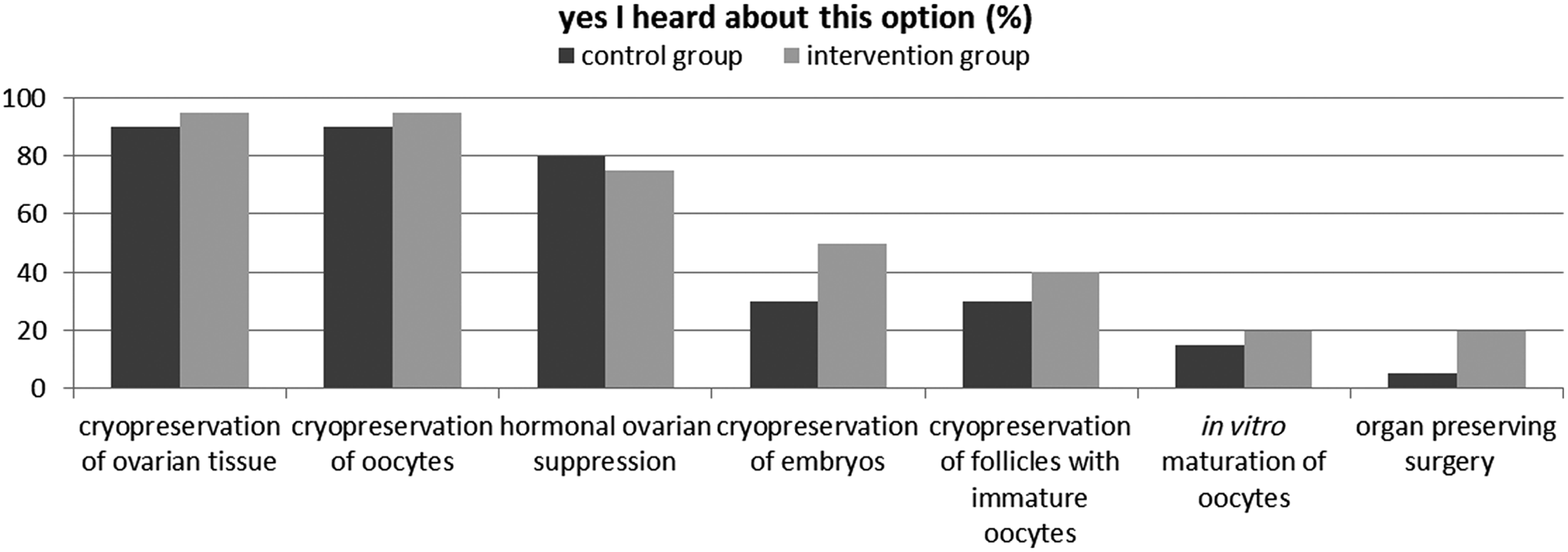
The most frequently known options in the overall sample were “freezing ovarian tissue” (92.5%, n = 37), “freezing egg cells” (92.5%, n = 37) and “hormonal protection of the ovaries” (77.5% n = 31). The same three techniques also represent the most commonly applied FP techniques within this sample (Table 1). Forty percent (n = 16) stated that they had heard about the option “freezing embryos,” 35% (n = 14) about freezing follicles with immature egg cells, 17.5% (n = 7) about in vitro maturation of egg cells, and 12.5% (n = 5) about organ preserving surgery. There are no statistically significant group differences in terms of knowledge (Fig. 1). The confidence of knowledge scores over all participants and options showed an average of 3.58 (with a maximum of 5). In regard of the option “freezing egg cells,” the intervention group showed a statistically significant (p = 0.047) higher confidence of knowledge (M = 4.00, SD = 0.82) compared to the control group (M = 3.39, SD = 0.78) (Table 2).
Knowledge about fertility preservation options in each group (%).
p < 0.05.
Mean (SD), from a 5-point Likert Scale ranging from 1 = not sure at all to 5 = very sure.
Decisional conflict (T1)
The mean overall score was 27.92 (SD = 13.27) out of a maximum score of 100, indicating a moderate DC. 37 20% (8) of the participants showed scores over 37.5, which is defined as high DC. Regarding overall score of the DCS, the intervention group showed a marginally higher mean score (M = 28.64, SD = 10.64) compared to the control group (M = 27.19, SD = 15.71) (Table 3). Regarding the subscales, the intervention group showed lower scores in the subscales “feeling informed” and “value clarity” compared to the control group. However, there were no statistically significant differences between the two groups, neither in the overall score nor the subscales.
Mean (SD), significant level with alpha <0.05, ANOVA.
DCS, decisional conflict scale.
Satisfaction with the DA
Participants reported to be satisfied with the DA. The helpfulness in the decision-making process was considered good and most participants would recommend the DA to other women in their situation (Table 4).
n = 20 (intervention group only); higher mean ratings indicate greater satisfaction.
Scores ranged from 1 = not at all to 5 = absolutely.
DA, decision aids.
Discussion
In this article, the development and evaluation of the first German online DA for young women considering FP after a cancer diagnosis are described. The pilot test revealed that the DA was well received by majority of participants. They considered the DA helpful and would recommend it to others. Furthermore, the study showed that knowledge related to FP was good with regard to the most frequently chosen procedures, and confidence of fertility-related knowledge was high concerning all options. DC was moderate with no statistically significant differences between the control and the intervention group. These results will need to be confirmed by our currently ongoing RCT.
Knowledge
Previous research has identified information and knowledge deficits with regard to FP in young cancer patients, 38 which was not the case in our sample. A fertility specialist had provided all participants with comprehensive basic information, and women assigned to the intervention group could additionally profit from the DA. As a consequence, knowledge as well as confidence about one's knowledge were satisfactorily high. Considering the small sample size of our pilot study, it is not surprising that the application of the DA did not lead to a significant increase in knowledge, as was the case in several other studies. 23 These results are of limited comparability, as they generally represent knowledge before and after the use of the DA, which was not the case in our study. Most participants in our study were remarkably confident about their knowledge on all FP options. This indicates that they felt already well informed throughout the counseling. Considering that some individuals wish as much information as possible, whereas others may be confused by too much information,39,40 a DA represents an ideal complement to counseling. Further research should focus on associations between knowledge and satisfaction with a DA.
Decisional conflict
The score of the overall DC in this sample was much lower than in our previous online survey on young cancer survivors (Mueller et al., submitted) and other studies.8,19 However, a substantial part of those participants had insufficient or no counseling about FP in these prior studies. All women from this study had access to comprehensive information and there seems to be some evidence that with higher knowledge and educational work, DC can be reduced. 23
The intervention group showed a tendency to higher overall DC; this, however, did not reach statistical significance. At first sight, this may be a contradictory result. However, according to Knops et al. 41 and Nelson et al., 42 a higher DC indicates that women are strongly involved in the decision; therefore, a slight increase in DC is not necessarily disadvantageous,41,42 especially when the DC is below the cutoff level, which was the case in our sample.
According to a Cochrane review, DAs may reduce DC related to feeling uninformed and unclear about personal values, 23 and it was precisely these two subscales that showed no tendency to higher scores in our intervention group.
The presented data were obtained immediately after FP counseling, and only analysis of the results at time points T2 and T3 will provide insight in potential changes of the DC over time between the two groups.
Limitations
The number of participants in this pilot study is small and interpretations of the results need to be treated with caution. The study design is consecutive, which may lead to bias, as recruiters and participants knew from the beginning to which group they would be assigned. These aspects will be addressed in the ongoing RCT. Moreover, we only included women who had already been referred to a reproductive specialist, while there are still a lot of women who are never referred or informed about FP before cancer treatment.
Conclusion
Individuals confronted with a recent cancer diagnosis and the necessity of deciding whether or not to opt for FP face a challenging situation in their lives, and adequate, well-thought out support is of utmost importance. Women often express the desire for guidelines or DAs with comprehensive information. 43 Professionals likewise, appreciate being able to offer qualitative and reliable references, 44 especially when considering that valid information about FP is still difficult to acquire and internet sources are often of questionable content. 44
Online DAs should be seen as a supplement support tool to fertility counseling,23,27 retrievable for the patient at any time and place. Currently, the number of available DAs for different patient groups is rapidly growing, but to our knowledge, there is no other German DA for female cancer patients regarding FP. By integrating the DA into clinical practice, more patients may profit from an additional helpful instrument for their decision-making process.
Footnotes
Acknowledgment
This study was financially supported by the Swiss Bridge Foundation and the Swiss Cancer League (KFS-3584-02-2015).
Author Disclosure Statement
No competing financial interests exist.