
Abstract
Purpose:
High incidence rates for cervical cancer in adolescents and young adults (AYAs: 15–29 years) make this the most common carcinoma in Brazil. Our aim was to analyze the incidence trends for cervical cancer (CC) and in situ neoplasia (IsN) among this age group.
Methods:
Incidence data were extracted from 21 Brazilian population-based cancer registries (PBCRs). Tumors with behavior code/3 (malignant) were classified as CC. Tumors with behavior code/2 were classified as IsN. Age-adjusted and age-specific incidence rates were calculated for individuals aged 15–19 years, 20–24 years, and 25–29 years. Incidence trends were evaluated by joinpoint regression analyses.
Results:
The median incidence rate of CC for AYA in Brazil was 3.63 per 100,000, with the highest rate observed in Recife (27.50 per 100,000). Significant increase in incidence for CC was identified in two PBCRs, with decreased rates for three PBCRs. The median incidence rate of IsN was 16.78 per 100,000 and was highest in Roraima (93.37 per 100,000). Increased incidence rates for IsN were identified in six PBCRs, with significant decreases in two PBCRs.
Conclusion:
The incidence rate for CC among AYA in Brazil is high and warrants intervention in terms of both prevention and control.
Introduction
C
High incidence rates for cervical cancer (CC) in AYA make this the most common carcinoma in four of the five Brazilian regions (North, Northeast, Midwest, and South). 3
Prevention against CC is well established for children and adolescents aged 9–13 years (Human papillomavirus—HPV vaccination) and for adults aged 25–64 years (Papanicolaou test screening) in Brazil. 4 However, AYAs aged 14–24 years fall between these groups and are therefore especially vulnerable to CC. HPV infections are common in this age group and appear shortly after the onset of sexual activity, although lesions typically regress in 3 years, with progression to cancer negligable. 5 Accurate data on incidence rates for CC in AYA are essential if we are to instigate changes to our current prevention and control programs. Relevant data are also critical for the establishment of educational strategies, improved prevention, detection, and survival rates. Our current aim was to analyze the incidence trends of CC and in situ neoplasia (IsN) in the Brazilian AYA group.
Methods
Data were retrieved from 21 Brazilian population-based cancer registries (PBCRs) located in the 5 Brazilian regions (North, Northeast, Midwest, South, and Southeast), 19 capital cities, 1 state (Roraima), and the Federal District according to the different time periods available. The last two editions of the International Classification of Diseases for Oncology (ICD-O2/ICD-O3) were used for coding of tumor morphology and behavior.6,7 Tumors with behavior code/3 (malignant), and morphological subtypes 800 (neoplasia not specified—NOS), 801–808 (squamous cell neoplasia), 814–838 (adenocarcinoma), and others (excepting NOS, squamous cell neoplasia, and adenocarcinoma), were classified as CC. Tumors with behavior code/2 (noninvasive/in situ), and morphological subtypes 805 and 807 (squamous cell neoplasia) or 814–838 (adenocarcinoma), were classified as IsN.
Age-adjusted incidence rates (AAIRs) and age-specific incidence rates (ASIRs) per 100,000 women were calculated for all 21 PBCRs according to age group (i.e., those aged 15–19 years, 20–24 years, and 25–29 years). Median incidence rates, used to measure central tendency, allowed us to derive an overall assessment of the incidence rate for the five regions. AAIR was estimated by a direct method using estimates of the world population for groups aged <30 years. Interquartile range was used to describe the distribution of incidence rates. 8
Information about quality indices was available in official home page of Brazilian PBCRs and can be seen in Table 1 (www2.inca.gov.br/wps/wcm/connect/estatisticas/site/home/rcbp).
Less than 10 cases.
AAIR, age-adjusted incidence rate; ASIR, age-specific incidence rate; CI, confidence interval; DCO, death certification only; IQR, interquartile range; MV, microscopically verified; NA, not available; PBCR, population-based cancer registry.
Incidence trends were evaluated for those PBCRs with 8–10 years of reporting (14 PBCRs). Among these (14) PBCRs, three (Palmas, Roraima, and Teresina) were excluded as they had values of zero. Joinpoint regression analysis was performed to identify significant changes in incidence trends, with estimates generated for the annual average percentage change (AAPC). The optimal cut-point period for measuring trends is described elsewhere; significance was determined using the Monte Carlo Permutation method.9,10 The protocol was approved by the Research Ethics Committee of Instituto Nacional de Câncer.
Results
Incidence rates of CC and IsN
The median AAIR for CC was 3.63 per 100,000, with comparable values for the Midwest (5.55 per 100,000), North (5.54 per 100,000), and South (5.53 per 100,000) and lower values in the Northeast (2.89 per 100,000) and Southeast (2.26 per 100,000) (Fig. 1). The greatest values for AAIR were those reported for Recife (27.5 per 100,000), João Pessoa (11.27 per 100,000), and Belém (7.28 per 100,000). The peak ASIR of CC, among all age groups (15–19 years, 20–24 years, and 25–29 years), was observed in Recife (Table 1).
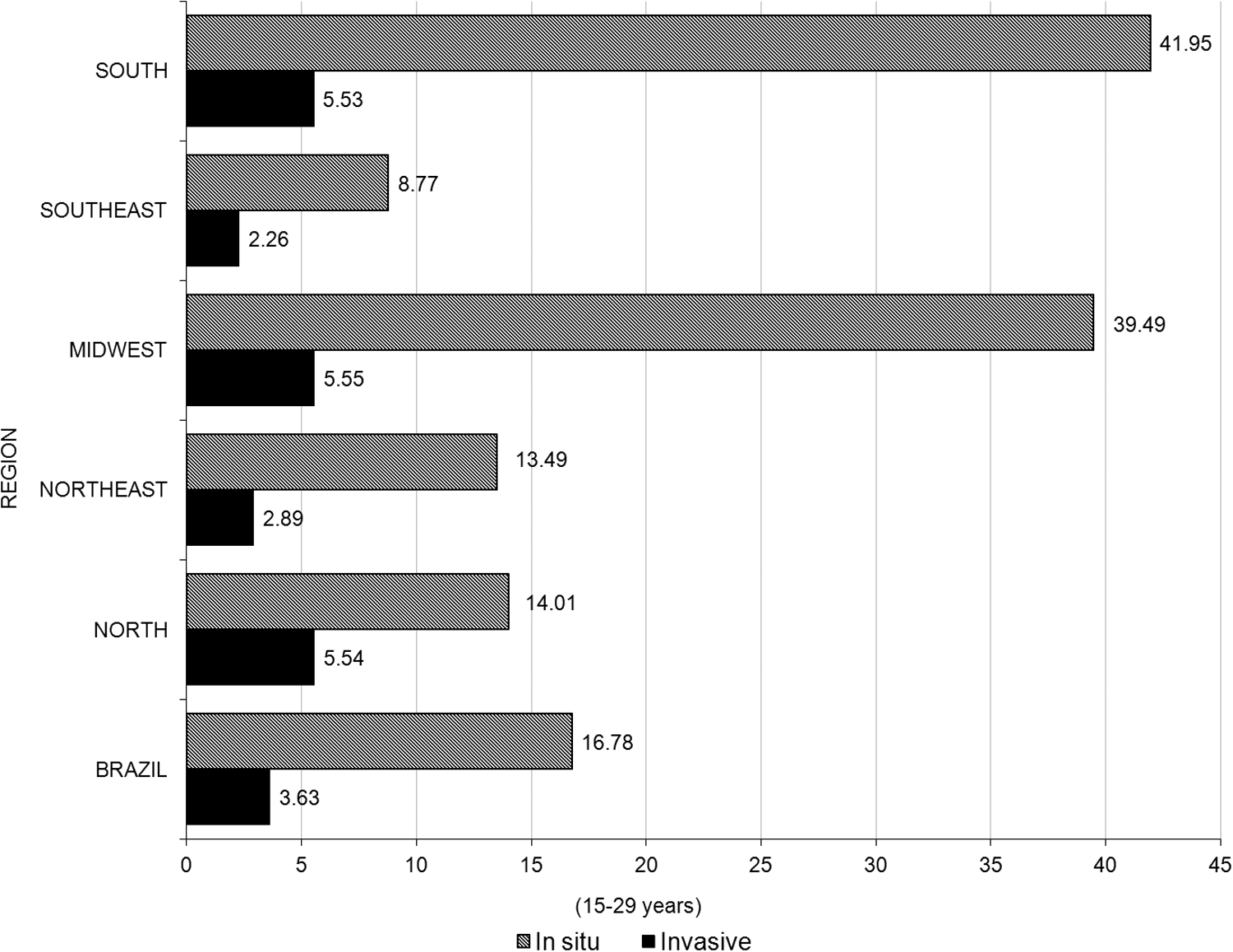
Incidence rates of cervical cancer/in situ neoplasia in adolescents and young adults.
Concerning IsN, the median AAIR was 16.78 per 100,000 with the greatest values seen in Roraima (93.37 per 100,000), Curitiba (59.00 per 100,000), and Goiânia (58.97 per 100,000). For the Belém and Teresina PBCRs, rates of in situ/CC were <1 (0.47/0.94), while in the João Pessoa and Recife PBCRs, values were just over one (1.19/1.08). The ASIRs of both CC and IsN increase with age, and a large variation in incidence rate was seen across the PBCRs. For those aged 15–19 years, the highest ASIRs were seen in Curitiba, Aracaju, and Roraima; the highest rates for those aged 20–24 years and 25–29 years were seen in Roraima (Table 2).
Less than 10 cases.
CC, cervical cancer; IsN, in situ neoplasia.
Incidence trends of CC and IsN
Figure 2 shows the incidence trends for all PBCRs, with significant increases in Belo Horizonte (AAPC +4.6) and João Pessoa (AAPC +12.6). In Aracaju (AAPC −13.8), Fortaleza (AAPC −7.7), and Goiânia (AAPC −14.0), important declines were reported.
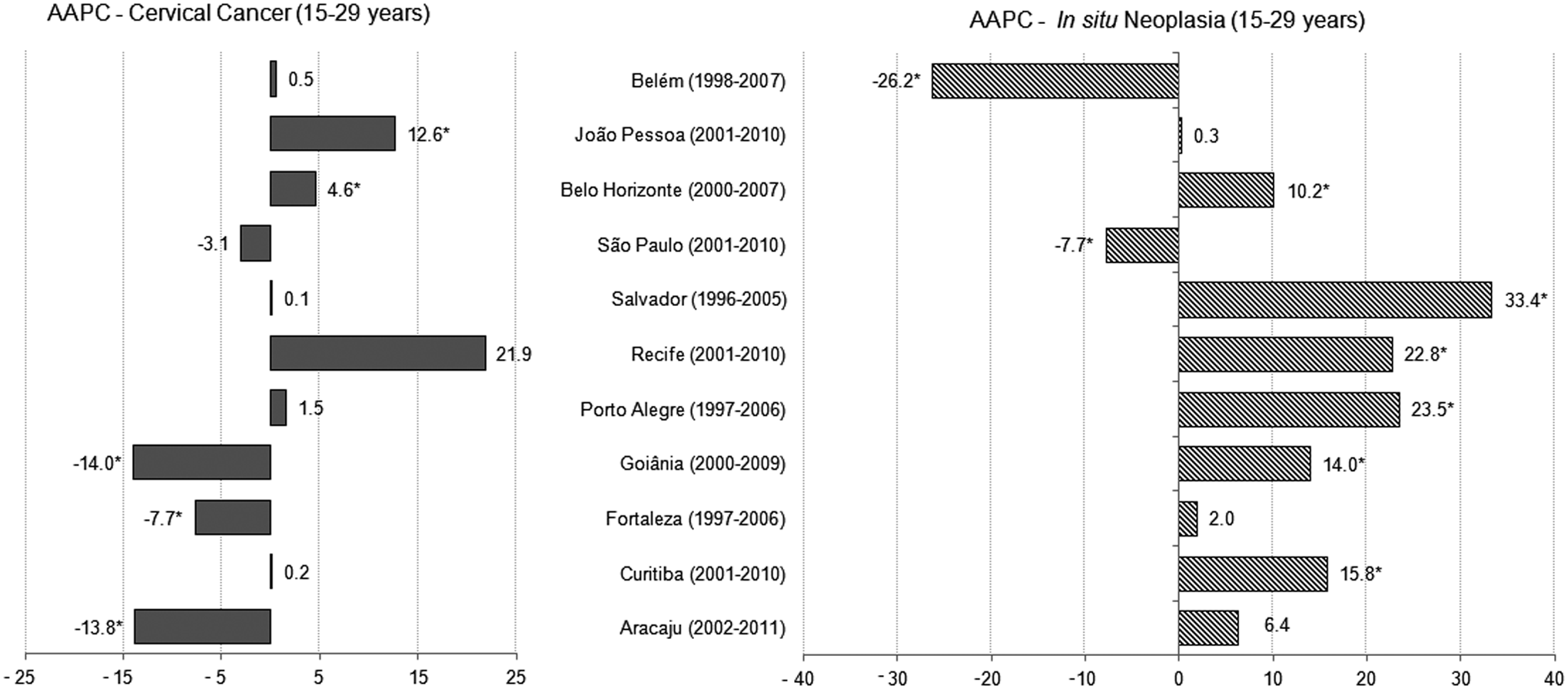
Joinpoint of analysis incidence trends of cervical cancer/in situ neoplasia in adolescents and young adults. *Statistically significant. AAPC, average annual percent change.
IsN manifested a significantly increased incidence rate in Curitiba (AAPC +15.8), Goiânia (AAPC +14.0), Porto Alegre (AAPC +23.5), Recife (AAPC +22.8), Salvador (AAPC +33.4), and Belo Horizonte (AAPC +10.2). The cities of Belém (AAPC −26.2) and São Paulo (AAPC −7.7) showed a significant decline.
Discussion
CC and its precursor lesions can be easily diagnosed with screening programs and their methodologies are well documented. Screening supports diagnosis and helps to improve survival rates. In Brazil, CC is the most frequent tumor in the North region, the second in the Midwest and Northeast regions, the third in the Southeast, and the fourth tumor in the South, for all ages. 11 The 21 PBCRs cover ∼20% of Brazilian population. In Brazil, 1.5% of this case load arises in those aged 15–24 years. 12 From 2011 to 2015, cytopathological examinations were completed for 19% and 14% of those aged 15–24 years and 25–29 years, respectively. 13 In our recent data, we observed a very high incidence rate of CC in Brazilian AYA. Among the group “carcinomas,” this cancer was the most frequent, with an incidence rate of 3.5 per 100,000. 3
In comparison, for the period 2005 to 2007, population-based data from Canada demonstrated an incidence rate for invasive CC of <0.3 per 100,000 for those aged 15–19 years, 1.2 per 100,000 for those aged 20–24 years, and 6.3 per 100,000 for those aged 25–29 years. 14 The National Cancer Registry of England described an incidence rate of 0.08 per 100,000 for adolescents (15–19) and 2.1 per 100,000 for those aged 20–24 years. 15 An Australian database described a significantly decreased AAPC (−2.7%) among those aged 15–39 years. 16 In a recent report from Korea, incidence rates of 0.04, 1.0, and 5.8 per 100,000 were reported for those aged 15–19 years, 20–24 years, and 25–29 years, respectively, with an increasing incidence rate observed for AYA. 17 In a recent analysis of the SEER database (2007–2011), incidence rates for invasive CC were reported to be 0.1 per 100,000 (15–19 years), 1.5 per 100,000 (20–24 years), and 6.6 per 100,000 (25–29 years) among AYAs. 18
The Brazilian median incidence rate is higher than those of developed countries. Recife, in the Northeast region, has one of the highest incidence rates of CC (27.5 per 100,000), which has increased from the rate of 19.3 per 100,000 recorded for 2005–2009. 3
Incidence trends of IsN also increased significantly suggesting the influence of screening programs. In the South region (Curitiba, Florianópolis, and Porto Alegre), we observed a high incidence rate of CC, with Curitiba registering the highest incidence of IsN. Smoking is associated with an elevated risk for high-grade cervical intraepithelial neoplasia (CIN) in young women. 19 The South region of Brazil is a worldwide leader in tobacco production and, despite a reduction in female Brazilian smokers, this region still has the highest rate of female smokers.20,21 Smoking can contribute to pathogenesis by reactivating or prolonging HPV infection. Among those aged 15–19 years, a high incidence rate of IsN was seen in this (South) region. While it is well known that low grade lesions regress spontaneously in this age group, around 2%–15% can progress to CIN3 (IsN).5,22–24
In addition, Soares et al. report correlates for risk factors such as the initiation of sexual activity and tobacco use in adolescents in the South region of Brazil. 24 Data from the Brazilian National Adolescents School-based Health Survey report that 27% of adolescents aged 13–15 years had initiated sexual activity. 25 Since 2014, vaccination against HPV has been recommended for girls aged 9–13 years by the Brazilian Health System through the CC program. 26 Recent data demonstrate a vaccine adherence rate of 74.2% nationally, with some variation across regions. The lowest adherence rate was in the North and Northeast regions (around 69%). 25
Pap smear testing in Brazil began in 1996, and, since 2011, has been recommended for all women aged 25–64 years following commencement of sexual activity. While it is well known that screening women aged <25 years increases the incidence rate by only 1%, our incidence rate in AYAs (<25 years) is extremely high. 27 Among four (19%) PBCRs, the ratio between IsN and CC is <1.19, suggesting that screening should be improved. Early diagnosis, sexual education, and access to treatment should all be emphasized. Increase in incidence rates of IsN across mostly all PBCRs draws attention; we believe that this is due to Brazilian CC screening program.
This study helps us to understand the incidence trends of CC in the AYA population and suggests possible causes. Furthermore, it also provides a framework with which to analyze future trends and assess the impact of prevention programs such as HPV vaccination. The main limitation of this study concerns the provision of data. PBCRs are only available for some Brazilian capitals and cities, making it impossible to derive accurate average statistics for the whole country. Another important limitation is discrepancies in describing this age group in several publications. In some studies, the AYA designation is reserved for those aged 15–24 years, 15–39 years, and even 15–49 years, making comparable analyses extremely difficult.15,16,28
The data generated in this study point to a high incidence rate for CC in Brazil, particularly for the 15–29 years old age group. Therefore, improved prevention and control are necessary, with the success of future measures assessed by robust epidemiological data.
Footnotes
Acknowledgments
L.S.V. and N.V.B. have a scholarship from Instituto Nacional de Câncer. B.D.C. has a scholar grant from the National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico, CNPq) (Brasília) (No. 306291/2014-2) and the Foundation for Support of Research in the State of Rio de Janeiro (Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro, FAPERJ) (Rio de Janeiro) (No. 212989-2016).
The authors are responsible for the content and writing of the article. L.S.V. and N.V.B. collected and analyzed the data. M.O.S., R.S.R., N.P.S., L.C.T., and B.D.C. discussed and interpreted the data. L.S.V., N.V.B., R.S.R., and B.D.C. wrote the article. All authors participated in the interpretation, read, and approved the final article.
Author Disclosure Statement
The authors report no conflicts of interest.