
Abstract
Many adolescent female cancer patients will survive into their reproductive years. Pediatric oncologists are advised to discuss oncofertility during treatment planning. In this pilot study, 19 adolescent females completed a retrospective survey assessing recall of a fertility discussion, satisfaction with fertility knowledge, and multiple factors that may influence recall, including parental involvement in decision-making. Eleven respondents (58%) remembered a discussion about infertility risk and 9 (47%) about fertility preservation. Most who recalled a discussion were satisfied with their fertility knowledge (10/11, 90.9%). In this study, we validated the feasibility of survey administration and identified trends in oncofertility counseling at our center.
Introduction
M
Adolescent female cancer patients are interested in information about fertility and fertility preservation options (FP)6,7 and place value on the ability to have biological children in the future.8,9 Multiple clinical guidelines advise oncologists to discuss treatment-related infertility risk and FP before the start of therapy.10–13 Despite this, many childhood and adolescent female cancer survivors report being unaware of their fertility status after treatment.6,14,15 Furthermore, adolescent and young adult (AYA) female cancer survivors admit to fertility-related distress, made worse by incomplete information about fertility.16,17
There are several potential barriers to adequate oncofertility counseling for adolescent females. Infertility risks are not definite or generalizable, and preservation options are limited. In addition, the adolescent patient is unique in her developmental status and decision-making capacity with a potential discrepancy between biological and emotional maturity, adding a complicated ethical component to these discussions. In this pilot study, our aim was to validate a survey to determine whether adolescent females remembered a fertility discussion during treatment planning, were satisfied with their knowledge of fertility information during diagnosis and treatment, and to identify factors that may influence recall. Based on studies of AYA patients, we hypothesized that recall of a fertility discussion would be low,6,9,14,18,19 leading to dissatisfaction with oncofertility awareness. 20
Our survey includes multiple domains to assess whether or not various factors influence recall. One domain specifically addresses adolescent involvement with decision-making. Treatment planning discussions typically involve the adolescent patient and her parent(s). With regard to fertility, adolescents desire information about potential infertility and FP and prefer to participate in decision-making. 21 In another domain, we assessed psychological status at the time of survey administration. While many childhood cancer survivors have normal psychological status and are well functioning, 22 some experience symptoms of anxiety, depression, and posttraumatic stress disorder (PTSD).23,24 We hypothesized that psychological symptoms could influence recall and satisfaction and thus included a modified symptom checklist. Given the retrospective nature of our study, we also compared patient recall with provider documentation of a discussion in the electronic medical record (EMR).
Methods
This single-institution study was approved by the Institutional Review Board of the Lurie Comprehensive Cancer Center and the Ann and Robert H. Lurie Children's Hospital of Chicago. Female patients seen in the Pediatric Oncology Clinic at Lurie Children's Hospital from October 2013 to April 2014 were asked to participate if they were between the ages of 13–18 years at cancer diagnosis and between 6 months and 3 years postdiagnosis at the time of the survey. Parents and 18-year-old participants provided informed consent, and participants 13–17 years of age provided assent before study enrollment. During the 6-month study period, 21 patients were assessed for eligibility. Two patients were found ineligible: relapsed disease (1) and declined participation (1). Nineteen patients completed the 45-item survey using the SurveyMonkey online survey tool (Supplementary Data S1; Supplementary Data are available online at www.liebertpub.com/jayao).
Three authors of the study (S.Z., K.H.A., R.C.) wrote this survey. Survey domains included questions about discussions of infertility risk, FP, and other side effects at treatment planning, parental involvement in decision-making, and satisfaction with fertility knowledge during diagnosis and treatment. Demographic and clinical information was obtained through participant report and review of the EMR. Current psychological status was assessed using a modified six-symptom checklist for anxiety and depression (and PTSD). Symptoms were reported on a 4-point Likert scale (1 = not at all, 2 = sometimes, 3 = often, 4 = very often).
This pilot study was an observational study and outcomes are reported as simple percentages.
Results
Demographics and patient characteristics
Table 1 summarizes patient-reported demographics and characteristics. The mean age at cancer diagnosis was 15.6 with a range from 13 to 18 years of age. Cancer types included sarcoma, lymphoma, leukemia, brain tumor, ovarian tumor, and other. All patients received chemotherapy and a minority also received abdominal/pelvic or cranial radiation and/or gynecologic surgery. At the time of diagnosis, 10 of the 19 young women had not thought about future pregnancy, whereas seven were looking forward to it and two reported that they did not want to become pregnant in the future. Multiple ethnicities and religions were represented.
Recall and satisfaction
Of the 19 respondents, 11 (58%) remembered a discussion about treatment-related infertility risk (Table 2). Another person (doctor, nurse, psychologist, social worker, or family member) initiated this discussion in 8 of 11 cases (73%). Regarding FP, nine respondents (47%) recalled a discussion, initiated by another person in eight of nine instances. Importantly, these results show that 8 (42%) and 10 (52%) respondents did not recall any discussion about treatment-related infertility risk or FP, respectively, during their initial treatment planning. Of the respondents who recalled a fertility discussion, 90.9% were satisfied with the information they knew during diagnosis and treatment (10/11; 1 respondent who recalled a discussion did not answer whether or not she was satisfied). However, only 63% (5/8) of those who did not recall a discussion were satisfied with the amount of information they knew at that time.
The respondents who remembered a discussion about FP were asked a series of questions about specific options and whether they used any of these options. Of the nine respondents who answered these questions, seven (77.8%) reported that oocyte, embryo, or ovarian tissue cryopreservation were described and/or offered, and four (44.4%) reported that they were told about a hormone used to protect their oocytes/ovaries. One respondent (11.1%) participated in ovarian cryopreservation and two (22.2%) took hormone pills. The six respondents (66.7%) who did not use any FP technique were asked to indicate any/all of several suggested reasons they declined. The marked reasons and corresponding number of respondents included: I thought my risk of having difficulty becoming pregnant in the future was low (3), I was too young at the time (3), I did not want to delay my cancer treatment (2), I did not want to be on an experimental protocol/clinical trial (2), and I thought it was too expensive (1).
There was no distinct correlation between recall of fertility discussion and recall of potential side effects on the heart, liver, or kidneys. About half of the patients remembered hearing about other side effects—6/11 of those who did recall a fertility discussion (54.5%) and 4/8 of those who did not recall a fertility discussion (50%).
Parental involvement
All respondents were asked about medical decision-making at the time of initial treatment planning. Twelve of 19 (63%) patients reported that their parents made all (5) or most (7) of the medical decisions, whereas seven (36.8%) of the adolescent females reported making decisions together with their parents. A greater percentage of adolescents who reported making joint medical decisions with their parents recalled a discussion of fertility (5/7 = 71%) than did those respondents who reported that their parents made most or all of the medical decisions (6/12 = 50%).
Psychological status
Each respondent ranked on a Likert scale how frequently she experienced psychological symptoms, including those that interfered with normal functioning (Fig. 1). The scores from each of the 19 patients were compiled to calculate the mean and median for each psychological symptom across all patients (Fig. 1). On average, respondents reported symptoms occurring not at all or sometimes. Notably, two respondents endorsed symptoms of both depression and anxiety occurring very often and one reported depression symptoms occurring often. Of the PTSD symptoms, four respondents reported “avoiding things that might remind them of their cancer diagnosis” either often (n = 2) or very often (n = 2).
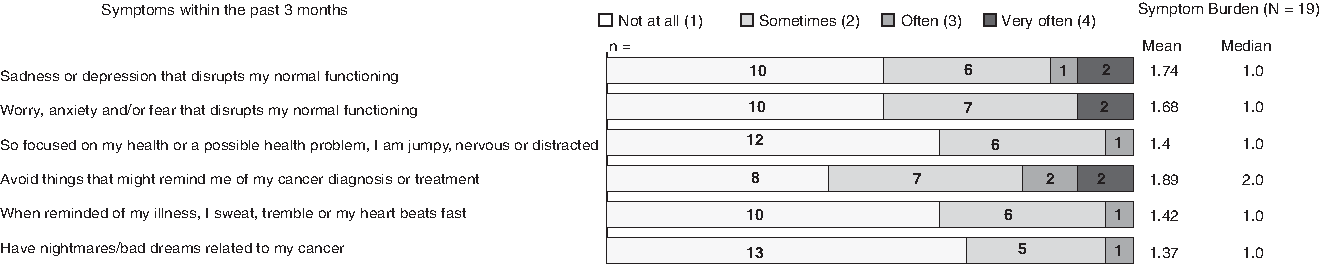
Psychological status at the time of survey administration and psychological symptom burden among all respondents. Survey respondents were asked to respond to the frequency of symptom occurrence in the past 3 months, based on a Likert scale (1 = not at all, 2 = sometimes, 3 = often, 4 = very often). Symptoms queried were sadness or depression that disrupts my normal functioning (depression), worry, anxiety, and/or fear that disrupts my normal functioning (anxiety), so focused on my health or a possible health problem, I am jumpy, nervous, or distracted (PTSD), avoid things that might remind me of my cancer diagnosis or treatment (PTSD), when reminded of my illness, I sweat, tremble, or my heart beats fast (PTSD), and have nightmares/bad dreams related to my cancer (PTSD). The number inside each colored bar represents the number of respondents for each number on the Likert scale. Psychological symptom burden across all respondents is represented as the mean and median of symptom frequency in all 19 respondents. PTSD, posttraumatic stress disorder.
Provider documentation
A review of the EMR demonstrated documentation of a fertility discussion in 10 of 19 charts (52%). For a majority of respondents who recalled a fertility discussion, one was documented (9/11 = 82%). Of the eight subjects who did not recall a fertility discussion, a discussion was documented in only one chart with no discussion documented for the other seven. Understanding that EMR documentation is not guaranteed to be complete and accurate, we calculated the sensitivity of recall to be 90% and the specificity of recall to be 77.8% (Supplementary Table S1).
Discussion
As adolescents diagnosed with cancer are better able to survive into adulthood, future planning and treatment late effects are now of more profound concern. AYA women have identified knowledge about fertility status as an important quality of life factor during cancer survivorship. 22 Their needs are recognized in clinical guidelines that advise oncologists to initiate discussions during treatment planning. This pilot study is the first to ask adolescent females treated at a pediatric oncology center in the United States whether or not they remembered and found satisfactory oncofertility discussions during treatment planning.
Although our study was small and qualitative, thereby limiting its generalizability, several observations may be informative in the design of future studies. In our cohort, we found that although many adolescent females do recall a discussion about infertility risks, a substantial proportion does not and even fewer recalled a specific discussion about FP. A majority of patients acknowledged that these discussions were initiated by another person—most frequently by a clinician and sometimes by a family member. We identified that young women who made medical decisions together with their parents were more likely to recall a fertility discussion. This observation suggests that oncofertility discussions should equally involve the healthcare provider, parent, and adolescent patient. Of those who remembered a discussion of FP, they cited various reasons for not undergoing the options offered. The reasons are consistent with those provided in the literature for AYA patients and included not wanting to delay treatment, being too young at the time, and cost. 25
We were able to capture information about psychological status using our symptom checklist. Overall, this was consistent with previously reported literature that a majority of childhood cancer survivors are well adjusted without a long-term psychological burden. 22 With a larger study population, we hope to detect whether or not there is an effect on patient recall in those who do have frequent psychological symptoms. We did not elicit an obvious negative emotional response to the survey itself. For the two patients who reported symptoms of anxiety and depression that “very often” affected their normal functioning, we referred these patients to their primary oncologist for further management of their symptoms.
A limitation of our study was that it was conducted at a single site with an oncofertility program. Lurie Children's Hospital has had a multidisciplinary Pediatric Fertility Preservation Program since 2008. This program is staffed by pediatric providers, including an oncologist, oncology nurse practitioner, endocrinologist, surgeon, and urologist. A reproductive specialist is accessible at the neighboring Northwestern Memorial Hospital for oocyte cryopreservation. Ovarian tissue cryopreservation is available in-house under an investigational protocol. These resources may have provided a survey study bias and improved the likelihood of oncofertility discussions being had with patients at our hospital.
The retrospective nature of our study contributes to an inherent recall bias. It is reasonable for patients to feel overwhelmed with the amount and extent of information they receive at diagnosis, making them less able to retain and recall this information later. From a research perspective, we could potentially reduce recall bias by administering the survey to those less distant from diagnosis instead of our current range of 6 months to 3 years. In clinical practice, providers should regularly revisit oncofertility discussions throughout treatment and in long-term follow-up. Based on our review of EMR documentation, not all patients had a fertility discussion, highlighting the need for improved communication and/or documentation.
Further surveys of adolescent female cancer survivors at multiple institutions will expand upon our observations to inform pediatric oncology providers of these patients' specific needs. With this information, providers will be better able to direct meaningful discussions about infertility risks and preservation options, while reducing the likelihood of patient dissatisfaction and future regret.
Footnotes
Acknowledgments
The authors thank Jill Woodman at Lurie Children's Hospital for assisting with the Institutional Review Board review and survey administration. S.Z. was supported by the American Pediatric Society/Society for Pediatric Research 2008 Student Research Program.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.