
Abstract
Global recognition of the need to improve outcomes for adolescents and young adults (AYA) with cancer has led to the development of specific oncology programs and services. In Australia, Youth Cancer Services (YCS) are now established across the country. While each service has been shaped by nationally agreed principles, program development has been influenced by local policy and geographic differences. Queensland is a vast state with a widely dispersed population; coordination of cancer services for young people across this landscape presents unique challenges. The Queensland YCS (QYCS) work in a consultative partnership model with primary treating teams, across both pediatric and adult tertiary cancer services. Understanding how cancer services approach challenges and service development can provide guidance for other developing services. In this article, we describe the goals and development of QYCS and review the outcomes achieved in the service to date. We reviewed referral data and retrieved statewide clinical activity from the web-based data system. We compared these data with cancer registry data to identify disparities and areas for service development. While the service has achieved notable outcomes, challenges remain. These include recruitment of appropriately skilled and trained health professionals for this newly developing area of oncology. In addition, there is an ongoing need to advocate for this relatively small patient group, and to promote awareness and understanding of the need for AYA-specific services. With the dispersed population and concentration of services in metropolitan Brisbane, identifying and testing new innovative models, including telehealth, to reach all AYA diagnosed with cancer regardless of location of care are priorities.
Background
W
In Australia, following a senate enquiry in 2005, the federal government formally recognized the need for dedicated and specialized AYA cancer services and provided funding in 2008 to develop a national service model. 5 Key elements of the model are presented in Box 1.
Key Elements of the National Service Delivery Framework. 6
To improve health outcomes for AYAs aged 15 to 25 years with cancer by the following:
(1) Establishing lead AYA cancer sites with linkage to local services and support
(2) Increasing access to clinical trials
(3) Facilitating access to comprehensive medical and psychosocial assessment at diagnosis
(4) Empowering of young people to be involved in decision making
(5) Ongoing management by multidisciplinary team expert in AYA care.
Due to the relatively small population numbers and immense geographical distances in Australia, it was recognized nationally that stand-alone AYA facilities similar to the Teenage Cancer Trust (TCT) 6 model in the United Kingdom would not be sufficient to suit the local landscape. This together with jurisdictional government policy has resulted in different service models across the five Australian Youth Cancer Services (YCS). 7
The national YCS network collaboration includes CanTeen Australia (a consumer support organization for AYAs with cancer) 8 and extensive engagement with individual consumers and specialist pediatric and adult health professionals. Federal government funding supports the national network of YCS, with some states, including Queensland, providing additional funding. This local state government support has ensured institutional buy-in and the development of sustainable services in Queensland.
The Queensland YCS (QYCS) was formally established as a statewide partnership model in 2013 to link the five tertiary cancer services in the state. Building on the extensive cancer networks already existing across public hospital and health services, the concept of centralized care for AYA cancer, with devolved care as appropriate, was formulated. Formal linkages were also made with one private facility in metropolitan Brisbane. Dedicated QYCS personnel are located across these partner sites (Fig. 1 and Table 1).
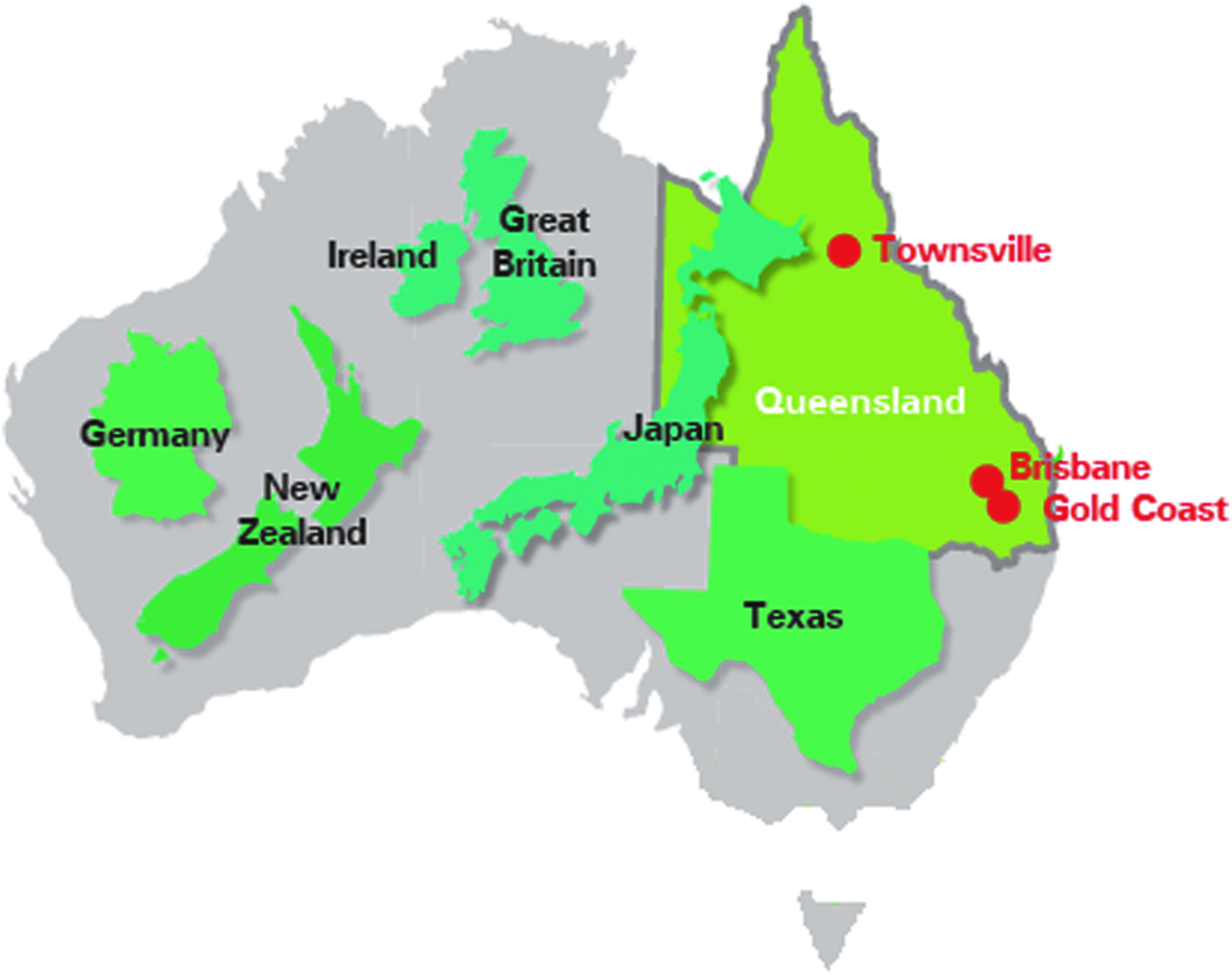
Map of Australia compared with other nations; locations of QYCS facilities in red.
Refers to level of Clinical Service Capability Framework (personal communication; Data manager, Queensland Children's Cancer Centre, 2016).
FTE, full-time equivalent; MDTM, multidisciplinary team meeting; MDT, multidisciplinary team;
More than half of the state's 4.6 million people live outside of the greater metropolitan area of Brisbane; compared with the rest of Australia, this is a large proportion of people living in regional or remote locations. 9 Like all other specialties, cancer services are concentrated in the southeast corner surrounding Brisbane, and access to highly specialized cancer services in the rest of the state is limited. As a result, many young people with rare cancers must travel to access specialist services.
From the outset, recognition of the need for close engagement, collaboration, and shared leadership with pediatric and adult oncology services guided the founding principles and development of QYCS. Because there was an existing model of centralized services for pediatric cancer within the same geographical area of Queensland, QYCS was purposefully developed with central leadership based in the pediatric cancer center for the state.
With a population of only 4.6 million, there was an argument to focus YCS to a single facility. However, this was deemed impractical because of the existing structures and attitudes in public and private facilities, and thus a consultative model was a pragmatic way to move forward in a timely manner. AYA cancer services across both the pediatric and adult cancer sectors were thus linked through formal partnerships and agreement between different services.
The QYCS strive to improve the collaboration between the pediatric and adult, public and private services by developing and maintaining professional relationships. Collaboration between services are complex processes and require intentional sharing of information and joint responsibility for patient care.10,11 Clear communication and agreement on defined roles, responsibilities for care provision and decision-making, can ensure patient needs are addressed across and between services. 10 However, referral barriers associated with “ownership” of a patient can prevent access to appropriate services.12,13 To overcome these institutional barriers, QYCS advocate for referral pathways based on individual patient needs.
The QYCS comprise a consultative central team, as well as clinical positions located across partner sites. The clinicians work in partnership with primary oncology treating teams to provide additional psychosocial support specific to AYA needs. The medical management of the majority of patients remains the responsibility of either pediatric or adult disease-specific oncologists or teams in the local center. The QYCS coordinate psychosocial multidisciplinary team meetings, using videoconferencing to facilitate access to specialist AYA staff, across partner sites. Medical leads, cancer care coordinators, and allied health clinicians at each partner site are responsible for AYA clinical care and navigation with hospital treatments.
The goal for optimal quality of care is to ensure access to appropriate AYA cancer support services (including location of care) and facilitate access to relevant clinical trials. 14 Achieving these goals requires the development of service models that are sustainable and accessible to patients in a variety of healthcare settings. 15
Guidance for successfully developing, implementing, or redesigning health services is limited. There are challenges with ingrained medical cultures and health systems that may not recognize the need for AYA-specific oncology services. 2 Understanding how services approach these challenges can provide guidance for other developing services. Hence our aim was to describe the goals and development of QYCS and document the outcomes achieved in the service over a 2-year period.
Methods
Design
We used mixed methods to address the aims of the study in two stages. In stage 1, we developed a logic model to describe QYCS' goals, service development, and desired outcomes. Models are useful for understanding goals and objectives, for inclusion of participatory planning, and to facilitate transparency, communication, and collaboration with stakeholders. 16 The model was developed to visualize and describe the many resources and components required to achieve outcomes, which then contribute toward evaluation of QYCS' goals.
In stage 2, we evaluated the outcomes of the service through review of key performance indicators and comparison of service activity data with incidence of AYA cancer data across Queensland.
Data collection and analysis
Stage 1
Interviews were completed with QYCS team members. Interviews focused on the role of stakeholder organizations, the structure (inputs), processes (activities), and objectives of QYCS. Field notes were documented during informal participant observation undertaken during team meetings. Qualitative data from interviews and field notes were organized according to themes regarding the structure, processes, and objectives of QYCS. The quality aspects of service delivery were measured using Donabedian principles to assess the fit of the structure and processes with the outcomes of QYCS.17,18
The structure of QYCS provides an indirect measure of quality related to facilities and personnel characteristics that are anticipated to produce outcomes. The structure of QYCS was assessed by documenting availability and skill mix of staff, and workforce capacity. The processes were assessed by examining the degree to which the QYCS delivered care consistent with the current evidence base and best practice. Key performance indicator measures, agreed nationally in partnership with CanTeen, included referrals to multidisciplinary team treatment meetings, enrolment on clinical trials, fertility preservation, and access to multidisciplinary psychosocial assessment and support. The proportions of AYA cancer patients referred to QYCS and the subsequent proportions of patients referred to specific AYA support services were calculated.
The short-term outcomes of QYCS were documented in terms of changes to processes, education of health professionals, and coverage of services.
Stage 2
As a new and developing service, the mechanisms to capture QYCS activity data were developed over time, and before 2015, data were not consistently recorded in a central location. In partnership with the Queensland Cancer Control Analysis Team (QCCAT), 19 processes were developed to reliably record QYCS referral and activity data across all partner sites in the Queensland Oncology Online (QOOL) database, a web-based system that enables data entry and review of cancer patients across all Queensland Health hospitals. 19 Activity data were assessed through examination of QYCS data between January 2015 and December 2016 entered into the QOOL database.
To facilitate comparison of AYAs referred to QYCS with the total population of AYA diagnosed with cancer in Queensland, verified epidemiological data were also collated from the Queensland Cancer Registry. These data included clinical as well as demographic information regarding location of residence (urban, regional, or rural/remote) and socioeconomic status. Because Queensland Cancer Registry data were only available from 2014, a 2-year time period (2013–2014) was used to compare incidence of cancer in 15–25 years olds with referral data to QYCS from 2015 to 2016. QCCAT was able to provide data regarding location of residence and socioeconomic status for QYCS data for 2015–2016. 19 Descriptive statistics were used to describe the characteristics of data.
To assess coverage of QYCS, Chi-squared tests were used to test for significance of differences between referrals to QYCS in 2015–2016 and the inferred expected total population of AYAs with cancer from Queensland Cancer Registry. This comparison assumes that a similar incidence pattern for AYA cancer occurred in 2015–2016, and provides an estimate of the proportion of AYA patients with cancer who are, and who are not, referred to QYCS. Further analysis of the population referred to QYCS was examined using descriptive statics and Chi-square tests to assess the significance of difference between variables.
Given that QYCS is a relatively new service, the intermediate to long-term outcomes described in the logic model were not assessed.
Results
The structure, processes, outcomes, objectives, and goals for QYCS developed as described above are outlined below and summarized in a logic model in Figure 2.
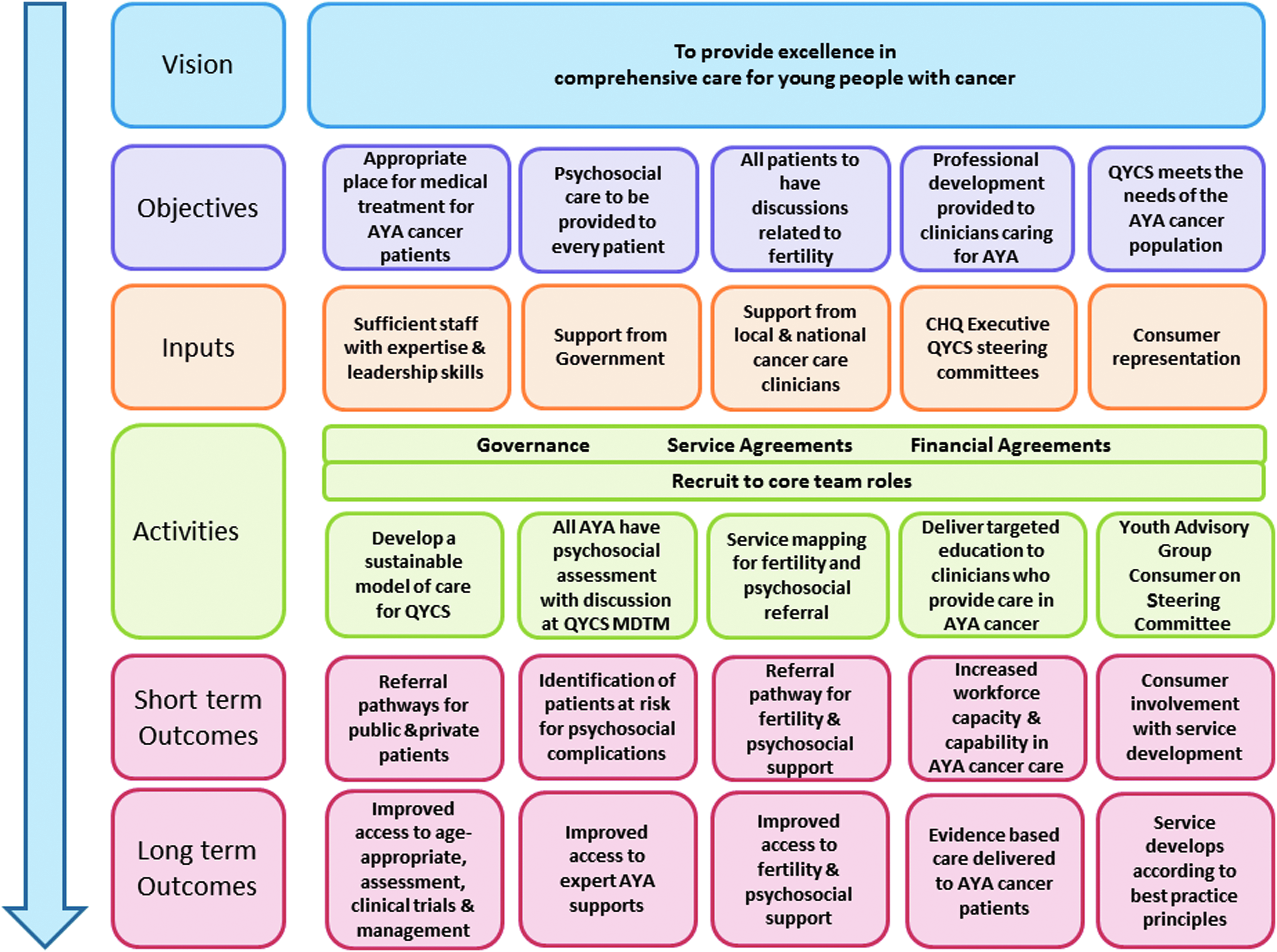
Logic Model of QYCS development.
Structure
The development of the workforce occurred in a purposeful, graduated process, with central team members recruited first, and extension to partner sites occurring over a 1-year period. The priority with initial service development was to establish coordinated referral pathways and data collection processes for Key Performance Indicators established by the National YCS. Service-level agreements, with Children's Health Queensland governance, were developed to formalize the relationships between the central and partner sites.
Public and private health facilities in Queensland have varying levels of capabilities, which are described in the Clinical Services Capabilities Framework (CSCF). 20 The CSCF identifies the capability criteria to deliver the minimum requirements of a service, including specific modules for cancer and pediatrics. The framework is used to plan health services and provides components of clinical governance, instilling confidence in clinicians and consumers that services meet the minimum requirements for patient safety. Clinical services can be classified by up to six levels, for example, level 4 or 5 cancer units may provide multidisciplinary services for common cancers, but rare cancers and highly specialized treatment will be treated at a level 6 service (Fig. 3). Detailed description of the QYCS at each partner site is outlined in Table 1.

Queensland Clinical Service Capabilities Framework (personal communication; Data manager, Queensland Children's Cancer Centre, 2016).
Processes
The processes and activity of QYCS were developed in collaboration with the National YCS, QYCS Steering Group, and over time, the Queensland Youth Advisory Group. The Youth Advisory Group consists of young people affected by cancer, has representation on the National Youth Advisory Group, and is an integral part of QYCS. The group meets quarterly and has contributed to the development of research plans, grant applications, presentations at conferences, as well as undertaking their own activities to provide peer-peer support to young people affected by cancer.
Clinical members of QYCS participate in the national YCS network through education and management committees. In this way, QYCS contribute to the strategic development of services across the country as well as in Queensland. Processes involving clinical staff include development of referral pathways, data collection, documentation, education dissemination, and development of local resources and information sheets. While treating health services retain responsibility for treating an AYA patient with cancer, dedicated YCS staff at each partner site assess and address AYA-specific concerns.
Outcomes
QYCS activity data for January 2015–December 2016 are presented in Table 2. Over the 3-year period since the QYCS started, there have been substantial changes to the processes for management of AYA patients, for example, the quaternary pediatric hospital has increased its age for new referrals to 18 years, and pediatric protocols are being used in adult facilities for certain diagnoses. Data suggest that the profile of patients who access QYCS is different to the 2013–2014 cancer registry incidence data for AYA cancers in Queensland.
Breast, cervix, ovarian, colorectal, and other carcinomas grouped and for calculation in contingency table.
Melanomas and other hematology excluded from chi-square calculation.
There is a statistically significant difference by gender; males were more likely to be referred to QYCS (p = 0.004). It is estimated that, of all AYAs diagnosed with cancer, 56% of males are referred to QYCS compared with just 35% of females. Patient age was also significantly associated with referral; 63% aged between 15 and 19 years were referred compared to just 35% aged 20–25 years (p = 0.001). There were no observed differences associated with location of residence or socioeconomic status with referral to QYCS.
There were differences noted with diagnoses: data suggest patients with leukemia, Hodgkin lymphoma, bone and soft tissue sarcoma, and brain cancer were more likely to be referred to QYCS partner sites compared to patients with non-Hodgkin lymphoma, germ cell tumors, colorectal carcinoma, and thyroid carcinoma.
Thus, these data confirm that patients with more complex disease, such as leukemia, bone sarcoma, or brain cancer, are more likely to receive treatment in CSCF level 6 cancer facilities affiliated with QYCS. AYAs with melanoma are rarely referred to QYCS; this is likely because the majority of melanoma diagnosed are early stage and do not require systemic treatment. Excluding patients with melanoma, these data suggest approximately 70 individuals, newly diagnosed AYA with cancer in Queensland are not referred to QYCS each year. Patients not referred to QYCS are more likely to be female, to be over the age of 20, and to have a non-Hodgkin lymphoma or carcinomas. While some patients will access treatment in the private sector, there are also likely to be patients receiving treatment in public hospitals not currently affiliated with QYCS.
Differences in referral to QYCS because of gender were notable; 135 males were referred compared to 99 females (Table 3). Gender differences in referral were significantly associated with diagnosis (p = 0.03), but not age group or location of residence. In males, the most common diagnosis referred to QYCS was germ cell tumors and leukemia (both 19% of all male). In females, the most common diagnosis was Hodgkin lymphomas (25% of all female) and carcinomas (15% of all female) such as cervix or breast.
Other not included in calculation of contingency table.
In addition to receiving medical treatment, the majority of patients referred to the QYCS receive the supportive services offered, including input from the psychosocial multidisciplinary teams, fertility preservation discussions, and psychosocial support. These services are standardized and patients are routinely offered the appropriate levels of support (Table 4). Enrolment on clinical trials remains low in this patient age group. Across years 2015–2016, we identified that only around 7% of AYAs with cancer were enrolled on a clinical trial in Queensland compared with 34% of children (personal communication; Data manager, Queensland Children's Cancer Centre, 2016). At the time of this study, the pediatric hospital moved locations, interrupting usual enrolment on Children's Oncology Group clinical trials; before moving, up to 60% of children were enrolled on clinical trials. Thus for AYA, clinical trial enrolment is low and only marginally better than the adult population who have an estimated 3% enrolment rate. 21 A review of open clinical trials for AYA across our partner sites identified that 22 trials were open during this time period; of the 18 patients enrolled on a clinical trial during 2015–2016, eight (44%) were treated in the pediatric cancer facility and the remaining 10 patients (56%) were in adult cancer facilities. Of the 232 new referrals to QYCS in 2015–2016, 100 (43%) were newly diagnosed patients treated at the pediatric facility and the remaining 132 (57%) patients were treated in adult facilities. From these data, it does not appear that treatment in a pediatric versus adult facility is associated with enrolment on a clinical trial.
The development of the workforce has been a crucial aspect of QYCS. One of the key roles of the service is to promote education in AYA cancer care, and to improve the confidence and competence of health professionals across the state. The education program, informed by a needs analysis, has focused on timely coordinated management of young cancer patients, with age-appropriate physical and psychological care. 22 Over a 3-year period (June 2013–June 2016), over 100 education sessions were delivered to over 1400 health professionals. This was achieved by engagement with the health community through workshops, monthly educational videoconferencing seminars, collaboration with existing statewide education services, and building relationships with existing health professionals around Queensland.
Discussion
We have described the goals, development, and short-term outcomes of QYCS between the years 2015 and 2016. The QYCS have developed strategically and systematically to build upon existing cancer services and foster new collaborations and partnerships with health professionals both in Queensland and across the nation. In line with the national services delivery framework, 5 the goal of QYCS remains to maximize the quality of care and promote consistency of practice provided to AYAs with cancer throughout the state of Queensland.
Notable outcomes of the service include the high proportion of AYA who receive psychosocial support, including having a documented care plan. There are also high proportions of AYA presented at multidisciplinary team meetings, and being provided with information regarding fertility preservation. Given that these were key goals of the service, we have achieved implementation of processes and laid the foundation upon which to further develop the service.
We identified that QYCS have a wide coverage of service provision to AYA diagnosed with cancer in the state, including a proportional representation of regional and rural patients. However, we also identified that younger patients (aged 15–19 years) were more likely to be referred to the service. This may be due, in part, to the location of the central team service in a pediatric hospital or because it is easier to promote the service in a site where care is already centralized; referral practices for adults, and for rare cancers, are not centralized.
Thus, AYAs may be treated in facilities not currently affiliated with QYCS. This includes a significant proportion of AYA who are treated in private hospitals. We estimate that approximately, only 10% of referrals to QYCS were from private hospitals, facilitated through our partnership with one private hospital at the time of this study. However, data suggest that an estimated 35% of AYA receive cancer treatment in private facility in Queensland.
While our data suggest that males are more likely to be referred to QYCS compared to females, we identified this was associated with diagnosis rather than gender per se. We therefore suggest that diagnosis and age are the strongest predictors of referral to QYCS. Patients with diseases that are recognized as complex to treat, such as leukemia, bone sarcoma, and brain tumors, appear more likely to be referred to major tertiary cancer centers, and hence QYCS-affiliated centers, whereas patients with diseases with established, effective, treatment regimens such as germ cell tumors and thyroid carcinomas appear to be commonly treated in other cancer services and not referred to QYCS. These patients may not receive access to age-appropriate psychosocial screening, support, and management.
Recruitment to clinical trials across the world remains a challenge for this population with numerous logistical and regulatory difficulties.14,23 Enrolment on clinical trials relies on suitable trials being available at treating cancer centers with the patients' age a limiting factor in clinical trial enrolment in both pediatric and adult facilities. 23
To better meet the needs and improve outcomes for this patient group, the International Charter of Rights for Young People with Cancer calls for recognition of 10 rights that include the following: (1) education about cancer and its prevention; (2) to be taken seriously when seeking medical attention and to receive the earliest possible diagnosis; (3) to have access to suitably qualified multidisciplinary specialists with significant experience in treating cancer in young people; (4) information about and access to clinical trials; (5) the need for age-appropriate support; (6) empowerment in decision-making to actively influence care; (7) fertility preservation information and counseling; (8) access to treatment in age-appropriate facilities; (9) financial and practical support; and (10) elimination of discrimination during and beyond. 24 The development of QYCS has been influenced by such advocacy, as well as national and state government policy directions and the establishment of AYA cancer programs in other nations, particularly that of the TCT in the United Kingdom. 6 With a smaller population, however, the Queensland model has developed to integrate with existing adult and pediatric multidisciplinary teams in a consultative model. This is similar to experiences in the USA where AYA programs or services are more likely to be consultative and linked to either pediatric or adult centers. 3 The consultative model relies on willingness to change and may limit recognition of Charter of Right for Young People with Cancer. A consultative model may also lack the critical mass required to drive change; this may compromise attraction and retention of staff with the appropriate skills and experience. As a result, the ability to influence other services can be limited.
Coverage and accessibility of QYCS are affected not only by the availability of the service but also by the awareness of health professionals that QYCS exist, and the appropriateness of QYCS for the individual patient. 25 Addressing the service needs of AYA with cancer requires a thorough understanding of needs that are both met and unmet. We identified that AYA patients referred to QYCS received access to services, including multidisciplinary team assessments, psychosocial care planning, and discussion regarding risk of infertility. Historically, these services were more likely to be offered on an ad hoc basis and particularly, for AYA patients in the adult oncology systems, access to psychosocial support and input from a multidisciplinary team were often the exception rather than the rule.
As highlighted in a recent study by Sawyer et al., major deficiencies exist for AYA treated in adult services in Australia. Unmet needs include access to psychosocial support, multidisciplinary team assessments, as well as other supports, including exercise physiology, dieticians, genetic counseling, peer support, and assistance with education and vocation; not meeting these needs is associated with emotional distress. 4 While our study included review of AYA patients referred to educational and vocational support, including metrics regarding access to other supports will help us understand how well QYCS are meeting the needs of AYA in Queensland. In addition, a greater effort is required to establish models of care with young people using technology to provide care across adult-focused cancer facilities. 26
While the use of videoconferencing is widely used for MDT meetings and education, there are few telehealth models of care in Australia, which are accepted as suitable for treatment for AYA cancer. 27 Telehealth services are not without challenges; common barriers include issues with coordination, adapting relationships and expectations, financial reimbursement across facilities, and the availability of clinicians.27–29 Although individual treating teams may choose to provide some aspects of care using videoconferencing, most commonly follow-up or supportive care, most young people living outside metropolitan areas are still required to travel to receive services.
A communications and marketing plan has been developed to promote awareness of the service; this includes monthly e-newsletters, an updated website, and local site visits to directly engage other cancer services. Research is planned to investigate telehealth models of care for survivorship. In this way, QYCS aim to promote awareness of the needs of AYA with cancer, prompt referrals, and address the geographical barriers in Queensland.
Limitations
The cancer registry data from 2013 to 2014 presented and used to estimate coverage of QYCS assume similar incidence patterns in 2015–2016 for AYA cancer. Because of the relatively small numbers of patients diagnosed with cancer in the age range of 15–25 years each year, number can fluctuate greatly year by year. Therefore, the calculations presented in this study are imprecise and results should be interpreted with caution.
A further limitation of our data is the reliance of data entry by multiple staff across different hospital facilities to identify patient enrolment on a clinical trial. At the time of reporting, we did not have accurate data recording systems to identify the number of participants who were eligible to participate in a clinical trial and the subsequent proportion that was enrolled on a clinical trial. As a developing service, including these metrics in our data collection will improve our understanding of the barriers to enrolling patients in this age group into clinical trials. These data, however, do provide valuable insight to guide the QYCS development and suggest target groups of patients where QYCS could be promoted.
Challenges
The challenges for the QYCS include the recruitment, and retainment, of appropriately skilled and trained health professionals for this newly developing area of oncology. To deliver high-quality, coordinated care to young people with cancer in Queensland, cancer services must work together, recognizing the need for, and the value of, services dedicated to AYA. The need to continue to advocate for this patient group and promote awareness and understanding of the need for a skilled and trained workforce for this relatively small patient group is an ongoing challenge.
In addition, it remains a challenge to establish a comprehensive youth cancer model of care for Queensland, which supports best practice treatment from diagnosis through to survivorship and/or palliative care, provided at the level of service capability of each cancer center. Testing new, innovative models of care such as the use of telehealth is important. Addressing disparities associated with age and diagnosis, and reaching broadly across the state, including primary care and local communities, are a focus for future service development.
Footnotes
Acknowledgments
We thank the members of the QYCS Steering Committee, the YCS teams within Queensland, and other jurisdictions—in particular the Service Managers and Lead Clinicians—who provided valuable input for the development of QYCS. The support and collaboration of all members of the YCS have been paramount to the development of services. This national approach has facilitated connections between clinicians at the service level. This work was presented in poster format at the Global AYA Cancer Congress 2017 and at the Clinical Oncology Society of Australia's 2017 Annual General Meeting. Youth Cancer Services receives federal funding through CanTeen as well as state and territory government funding.
Author Disclosure Statement
No competing financial interests exist.