
Abstract
Background:
Young people with cancer have distinct clinical and psychosocial needs during and after cancer treatment. However, as adolescent and young adult (AYA) cancer is rare, and only recently recognized as specialty, health professionals may not have the skills, competence, and confidence to meet the needs of the young patient with cancer. The aim of this study was to identify the learning needs of health professionals providing cancer care to adolescents and young adults before and following the introduction of a state-wide AYA cancer education program.
Methods:
A survey of educational needs of health professionals was undertaken in 2013 at the commencement of the Queensland Youth Cancer Service. The survey was used to develop the education program of the service. The education program was delivered across the state in a variety of formats, covering a range of topics throughout 2013–2016. The second survey was completed in 2017. Results were compared to identify if educational needs or the self-rated confidence of health professionals in regard to AYA cancer care had changed over time.
Results:
One hundred twenty-two participants completed the first survey and 73 completed the second. The most prominent educational needs in 2013 were palliative care and biomedical topics such as understanding AYA growth and development as well as specific AYA cancers and treatment. The second survey identified that palliative care education remained important; however, there was a shift toward health professionals request for more psychosocial and practical education on topics including fertility, sexuality, and managing late effects.
Conclusion:
To provide high-quality healthcare to AYAs with cancer, health professionals require ongoing opportunities for education and training.
Background
N
As an emerging new subspecialty, the distinct clinical and psychosocial needs of adolescents and young adults during and after cancer treatment are prominently described in the literature.4–8 Health professionals caring for these patients need to be skilled in communicating with AYA regarding a wide range of topics, including specific AYA cancers (biology, genetics, and epidemiology); biomedical treatment; psychosocial needs; clinical trials; fertility preservation; sexuality and intimacy; education and vocation; and relationships with family and peers. At different stages during the trajectory of cancer treatment, the young person will need information and support regarding diagnosis, treatment, late effects, and survivorship, including palliative care (if required). 5
AYA oncology educational and training programs are scarce.2,5 While pediatric and adult training models are more common, they do not provide all the necessary components specific to AYA needs and concerns. 3 As a result, health professionals report being inadequately prepared to provide the care required to meet the needs of AYA. 9
To address the educational needs of multiprofessional AYA cancer care specialists, a multileveled approach is required to build upon the fundamental principles of teamwork, alliance, and innovation, and to consciously expand learning. An important aspect of the learning process is that individuals critically reflect on assumptions and beliefs about their own practice and challenge both themselves and the accepted norms in service delivery. 10 Health professionals' knowledge of biomedical, psychosocial, and practical factors specific to AYA cancer care are key outcomes that may be used as measures to assess the quality of care for AYA cancer services. 4
For these reasons, AYA cancer services should have extensive multiprofessional education programs, which include the assessment of health professional's knowledge, and addresses satisfaction with the education, practice standards, emerging issues, and local learning needs. 3
Recognizing the unique needs of AYA with cancer, international groups have established youth-specific services in many nations. 11 In Australia, Youth Cancer Services (YCS) provide support and care to AYA with cancer aged 15–25 years. The development of the national YCS network is underpinned by the key principles outlined in the National Service Delivery Framework for Adolescent and Young Adults with Cancer. 12 This framework includes specific guidelines regarding training of health professionals in adolescent health.
The Queensland YCS (QYCS) is one of five national YCS and faces unique challenges in the provision of AYA cancer care associated with the vast geography of the state. Queensland is a large state, over 1,700,000 square kilometers—seven times the size of Great Britain—and with a widely dispersed population of just 4.5 million. 13 YCS staff who provide specialized AYA cancer care are employed only in the five major cancer centers in Queensland; however, some adult cancer services are provided widely across the state. While the majority of AYAs with complex cancer diagnoses are treated in one of the five major cancer centers affiliated with YCS, AYAs also receive cancer care in services that have no formal links with YCS, and from health professionals who may have limited experience, knowledge, and understanding of AYA-specific needs.
QYCS education for health professionals
As a statewide service, the QYCS aims to address the educational needs of health professionals across the state. Established in 2014, the education program of the QYCS is a crucial component of the service and aims to increase the awareness, knowledge, competence, and confidence of the workforce who provide cancer care to AYA. A survey to identify learning needs of health professionals was undertaken in 2013. The outcomes of the survey, along with AYA cancer care education frameworks,12,14,15 were used to inform the development of content and format of the QYCS education program. The statewide program was coordinated by a nurse educator with post-graduate training in AYA cancer care, in collaboration with other multidisciplinary colleagues.
An example of the content of the program is summarized in Table 1. The education program was designed to cover the principles, knowledge, skills, and desired attitudes of health professionals in AYA cancer care. The program provides learning opportunities with the aim of supporting the development of skilled, confident, and dedicated professionals to increase workforce capacity in AYA cancer care.
COSA, Clinical Oncology Society of Australia; AYA, adolescent and young adult; YCS, Youth Cancer Service; HSCT, hematopoietic stem cell transplantation.
PowerPoint presentations on a variety of topics were developed and disseminated to YCS-affiliated sites to facilitate access to consistent education content at clinician convenience. Regular workshops and seminars are undertaken in both metropolitan and regional locations, and because of the geography of the state, videoconferencing is regularly utilized to connect health professionals dislocated by distance. All videoconference education sessions are didactic in nature, with the ability for participants to ask questions throughout the presentation. Videoconference sessions are also recorded and made accessible on the Queensland Health intranet site. In addition, funding scholarships to support post-graduate AYA oncology education were provided to clinicians in YCS-affiliated cancer services through CanTeen. 16
The aim of this study was to identify and describe the learning needs of health professionals regarding AYA cancer. Secondary aims were to assess overall changes within the culture of AYA education over time, and to consider the effects of the QYCS education program on health professional confidence with providing AYA cancer care.
Methods
The first survey of learning needs was developed and distributed through professional networks to health professionals working in cancer care in 2013. The survey was reviewed and administered again in 2017. Both surveys were performed as quality activities and the Children's Health Queensland Hospital and Health Service Human Research Ethics Committee endorsed the work, and provided permission to publish the study as a quality activity. Data regarding attendance and feedback of educational sessions were prospectively collected and reviewed to inform the direction of the educational program.
Survey development
The 2013 survey was developed from themes identified in the AYA cancer literature5,12 and input from an AYA working group, which included Cancer Council Queensland, CanTeen, Redkite, multidisciplinary cancer team members from adult and pediatric centers, and other relevant stakeholders. The survey was piloted with nursing staff working in cancer services and feedback was incorporated into the final survey by study author RE. The first survey was an 86-item questionnaire that included demographics, participant experience with AYA cancer care, preferences for format and delivery of education, importance of topics, and self-perceived knowledge and confidence with aspects of AYA cancer care.
The follow-up questionnaire in 2017 was purposely reduced to 21 items by using different formatting to simplify the process of obtaining information. Some items were removed because questions had been confirmed as adequate in the first survey (e.g., access and availability of email and videoconferencing). Multiple other questions were collapsed into single questions. For example, in the first survey, participants were asked to provide a yes/no answer for eight different options for the type of education format that would be most beneficial, resulting in eight individual questions. The second survey listed all possible eight educational formats in the one question and asked participants to tick all options they would find beneficial. In this way, the survey was simplified to reduce the overall length without reducing the information.
In both surveys, closed questions with multiple-choice answers were used, along with questions answered by a five-point Likert scale, drop-down box/tick a box, and percentage scales. Following a section on demographics and experience with AYA cancer, participants were asked to rank the importance of specific topics for education subjects such as palliative care, psychosocial support, or fertility preservation. Participants were asked how frequently they wanted AYA-specific education, for example “once per month,” “every 3 months,” “every 6 months,” or “yearly” and in what formats. Participants were also asked to rate their confidence with topics such as discussing sexuality, AYA risk taking, or providing career advice to young people with cancer. Free text space was also provided for additional comments.
Survey administration and analysis
Both surveys were administered electronically (Survey Monkey®) and by paper copies. A purposive convenience sample of health professionals identified through professional cancer networks was used. An email with a link to the survey was sent to senior medical and nursing clinicians across cancer networks involving multiple public and private institutions. The email described the purpose of the survey, the potential of the findings to influence educational programs, and assurance that the survey was anonymous. Managers were requested to forward the email onto relevant clinicians involved in AYA cancer care. One reminder notification was sent after 2 weeks and the surveys remained open for 4 weeks.
Clinicians were also invited to participate in both surveys by completing paper copies when attending local education events or at local healthcare facilities. Results from the surveys (both electronic and paper based) were collated using excel. Data from the five-point Likert scale were collapsed into positive, negative, and neutral responses. Results were reported using standard descriptive statistics, including sums and means, and survey items were analyzed with Chi-square calculations to assess the significance (p value <0.05) of differences between and within the two time periods. Qualitative comments were grouped into themes.
Results
Educational program
Between 2013 and 2016, over 100 individual education sessions were undertaken, reaching an estimated 1400 individuals. Feedback from the videoconference series, workshops, and in-service sessions was generally always positive with the majority of responses indicating sessions were valuable or extremely valuable. Most negative comments related to technology problems with video/audio communication. Comments for improvement generally suggested alternative topics, such as transitioning patients to the community, strategies to engage with AYA, and survivorship care.
Survey results
It was not possible to know the exact numbers of clinicians who were approached to complete the surveys through email, and we are unable to report a response rate. There were 122 participants who completed the first survey in 2013 and 73 participants in the second survey in 2017. Because both surveys were anonymous, it is not possible to know how many participants completed both surveys.
The characteristics of participants were comparable between 2013 and 2017; the majority of participants were nurses or allied health clinicians with a smaller proportion of medical staff (Table 2). In 2013, most participants identified as working in either pediatric or adult hematology/oncology settings. By 2017, the QYCS was well established and some participants identified as working specifically in AYA cancer care. Most participants in both 2013 and 2017 worked in the public healthcare sector and in metropolitan locations; however, regional locations were proportionally represented. In 2017, the survey included the option of nominating a workplace as a Non-Government Organization in recognition of their unique position supporting AYA with cancer.
Does not sum as some participants nominated > one type of specialty or facility.
Other includes community and primary health settings.
NGO, Non-Government Organization.
Similar proportions of participants reported experience with caring for AYAs with cancer in both 2013 and 2017 (n = 101, 83% and n = 62, 85%, respectively). Of those who reported working with AYA cancer patients in 2017, the mean proportion of AYA cancer workload was 31%. Two (3%) participants from 2017 reported achieving post-graduate qualifications in AYA cancer care.
Education needs and format
Participants were asked to rate the importance of receiving education on a range of AYA topics. Education on palliative care for AYA was rated as a high need in both surveys. In 2013, participants rated biomedical topics such as understanding AYA growth, development, disease trajectories, and care requirements more importantly than in 2017. Participants in 2017 valued more specific and practical information in relation to psychosocial care, late effects, fertility and sexuality, education, and careers (Fig. 1).

Most valuable information for adolescent and young adult cancer education.
This suggests that between the two survey time points, health professionals have developed greater understanding of the biomedical aspects of caring for AYA and that psychosocial and practical issues are now taking prominence in educational needs. Online and/or videoconferences and 1–2 hour education sessions were the most valued format in 2017. This was a change from 2013 where workshops and in-person presentations were more valued, demonstrating the impact technology has had on our ability to readily access education. In both surveys, formal study and achieving post-graduate qualifications were less valued. Monthly educational opportunities were the most preferred frequency of education delivery in both 2013 and 2017.
Resources most accessed for AYA cancer
Participants were asked what resources they would access for concerns regarding provision of care to an AYA with cancer. Participants could nominate all resources they would likely access. There was a difference between survey results between 2013 and 2017 (Table 3). Respondents in 2017 were more likely to identify numerous sources of information, with 89% identifying they would access AYA oncology health professionals in 2017 compared to just 31% in 2013. This is likely a result of greater awareness and development of the QYCS over that time period. Results suggest more awareness of the availability of resources as well as an increased preponderance to consider accessing multiple sources for support.
Youth Cancer Fact Sheets were not available in 2013.
COG, Children's Oncology Group.
Skills confidence
Participants were asked to rate their confidence in caring for AYA with cancer. In both surveys, all participants were most confident in communicating with AYA with cancer and providing psychosocial care and support (Fig. 2). There were some changes in overall confidence ratings between years 2013 and 2017; however, these changes were not significantly different between years, indicating that respondents from both surveys shared similar confidence levels; most clinicians rated their confidence as either neutral or not confident across all other domains.
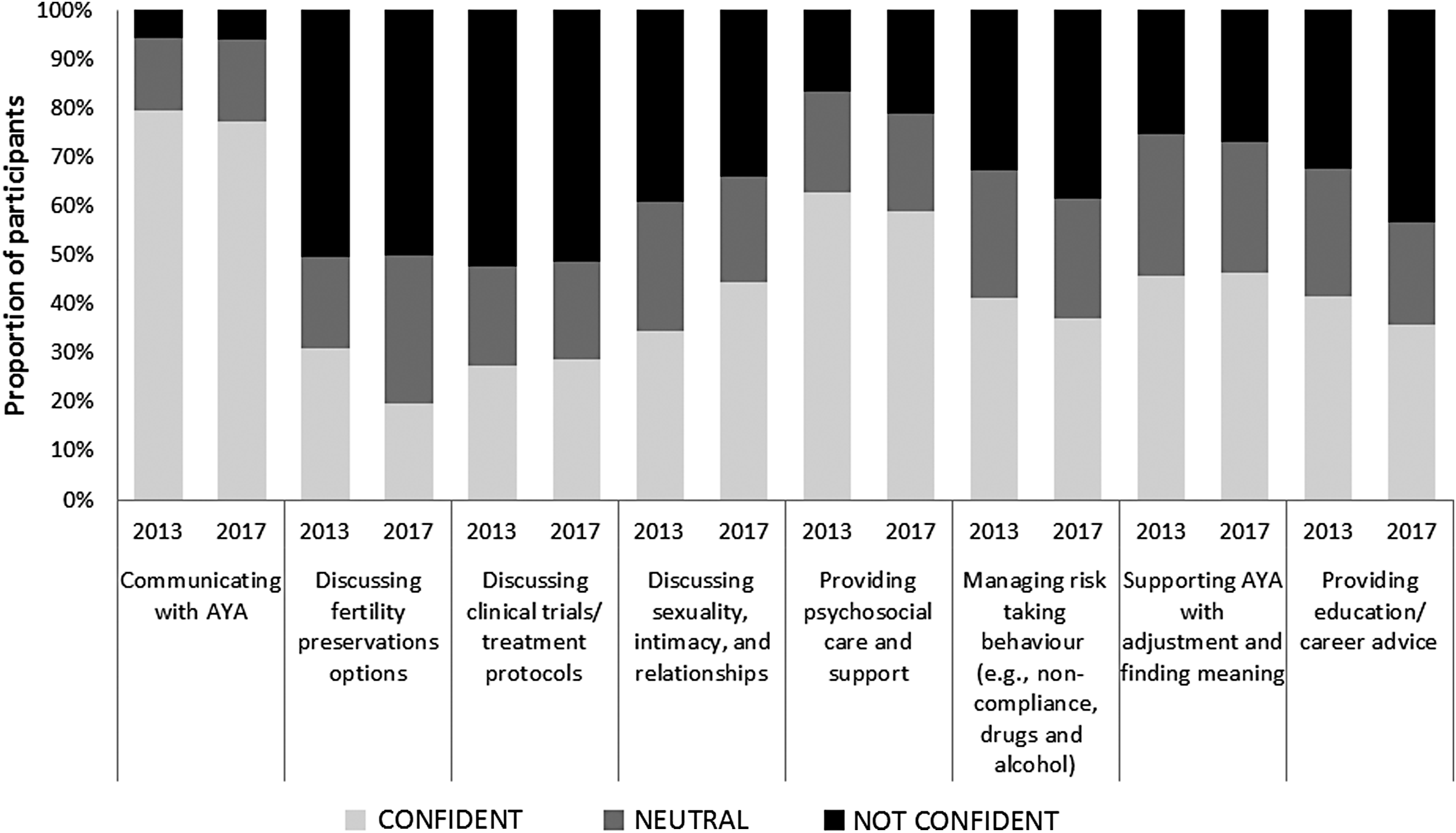
Self-rated confidence with AYA cancer topics.
Subanalysis by discipline of nurses and allied health in 2017 demonstrated that nurses were more likely than allied health to be confident discussing clinical trials and treatment protocols (p value = 0.01) and allied health was more likely than nurses to be confident in discussing post-treatment/survivorship issues, or identifying and referring to services for post-treatment follow-up (p = 0.02).
Barriers to education and professional practice
Participants identified a number of barriers to participating in education sessions and providing care to AYA. Time, resources, and being relieved from clinical duties to attend education sessions appeared frequently, with several participants proclaiming:
“It is extremely important to be working from an evidence based perspective but this can be hard when time restraints and case-loads prevent this.” (Metropolitan, adult cancer service, 2013 survey).
“It takes time to gain the respect and trust of a teenager, they need to have a sense of independence yet they are to some extent dependent while unwell. The team needs to be coordinated in the care they give these young people, they need extra time to spend time with the patient but also to communicate well with the treating doctors.” (Metropolitan, paediatric cancer service, 2013 survey).
“Due to budget restraints, our adolescent unit closes frequently. This gives an insecure feeling around our ability to have confidence in treating this group” (Regional paediatric cancer service, 2017 survey).
Participants recognized the importance of education and training, but were not always able to access these opportunities. Having dedicated time and resources to provide high-quality AYA care competes with other priorities. Another identified barrier was the rarity of an AYA with cancer in an adult-focused facility, where staff identified they did not have the required expertise to manage the patient and provide quality healthcare.
“AYA patients are the hardest to deal with in many ways sometimes… and extra knowledge in how to deal with this would be greatly appreciated!!” (Metropolitan paediatric cancer service, 2013 survey).
“We have very limited experience with adolescents and young adults. The staff would require extensive education and training in caring for AYA patients with cancer.” (Regional, adult cancer day unit, 2017 survey).
“We see lots of family dynamics, and have trouble with specific issues such as non-compliance, that most nurses on the ward feel ill-equipped to handle” (Metropolitan adult cancer service 2013 survey).
Health professionals may feel out of their depth when providing care to young people with cancer, or may not be aware of their specific needs. The provision of accessible education, and allocation of time to attend educational sessions, is imperative to improve the confidence and competence in providing cancer care to young people.
Discussion
We explored the self-identified educational needs of health professionals who care for AYA with cancer before and after implementation of an AYA educational program in Queensland, Australia. Palliative care education was identified by health professionals as a strong need in both the 2013 and 2017 survey. Palliative care in this age group is a challenging concept to most healthcare professionals, even those who have received training and work in the field. 17 In addition, with advances in targeted therapies, some patients are living indefinitely with incurable diseases. Palliative care for AYA is thus a further subspecialty requiring additional and ongoing education and training for health professionals.
Other findings from the surveys indicated a change in focus from biomedical AYA cancer topics in 2013 to more psychosocial and practical topics in 2017. This may be attributed to the emphasis of the educational program during the preceding years and indicates health professionals are more aware of issues such as normal growth and development during adolescence, and there is a desire for greater information regarding psychosocial and practical information in relation to AYA cancer. The QYCS education focus across the years 2013–2016 was broad and encompassed topics including cancer epidemiology and biology, adolescent health and well-being, as well as aspects of psychosocial care. It may be that having become more familiar with the biomedical aspects of care, health professionals are placing more importance on these other aspects of care. The second survey may also have been completed by a different group of health professionals.
Our sample in both surveys contained high proportions of health professionals who had experienced caring for an AYA with cancer; as cancer in AYA is rare, our sample may not be representative of health professionals who provide cancer care in Queensland. Despite having experience in caring for AYA with cancer, of note was the lack of change between the two surveys regarding confidence of respondents with specific aspects of AYA cancer care, despite the education program. There was little or no change in between surveys regarding confidence level with discussing fertility preservation, clinical trials, managing risk taking behaviors, or providing education or career advice. There were only two areas where more than 50% of health professionals reported they felt confident with their practice, communicating with AYA, and providing psychosocial care and support. These findings are somewhat contradictory as respondents also identified as wanting more education targeting these areas. This may be related to particular topics such as palliative care, which was also expressed as a high learning need in both surveys. Highlighted by Hayes-Lattin, continued progress in AYA cancer care requires a deep understanding of the contributors to poor outcomes for this group and thus research, and a cadre of competent healthcare professionals trained in this area is imperative. 5 Our findings indicate health professionals consistently report low confidence across a number of domains important in providing cancer care to AYA. This is likely due to of the rarity of cancer in AYA and the lack of opportunity to develop skills and confidence in this area. We acknowledge that cognitive knowledge alone is likely insufficient to change practice; a comprehensive educational program requires a framework that considers broader initiatives. In addition, results from this study may be used to help drive policy regarding education in this area and to advocate for recognition of the minimum skills required to provide care to AYA with cancer.
The lack of a trend over time to demonstrate a change in confidence may be attributed, in part, to staff turnover and the relative rarity of AYA cancer in most cancer services. High staff attrition in nursing is a worldwide phenomenon. 18 In Australia, high staff attrition is particularly difficult for regional cancer centers, where there may be little available expertise in rarer cancers such as those found in the AYA population. While childhood cancer is also rare, in Queensland, pediatric cancer care is centralized; all children will have their cancer care managed by the only tertiary pediatric hospital in the State. Staff at this facility receive training and education specific to pediatric cancers and are familiar with providing care to children and families. There are established programs to support regional facilities that share the care with the pediatric cancer center. 19 Since November 2014, the pediatric cancer service has admitted patients up to 18 years of age and therefore more AYAs are receiving care within pediatric settings where staff may not have received specific AYA training. Cancer care for adolescents and young adults is not centralized; over the age of 15 years, an individual may also be referred to a wide range of cancer facilities. Most of these facilities, including private cancer centers, treat adult cancer patients, and for many services, a young person will be a rarity. Without experience in caring for the young person with cancer, it is not possible to develop confidence and competence in this area.
For these reasons, young people with cancer are referred to as living in a “middle world,” in a no man's land that is not well recognized by the existing health system. Being neither adults nor children, their needs are often not met by services that fail to appreciate or respond to factors that impede quality healthcare for this group. 20 Health professionals are simply not familiar with providing cancer care to this age group. As a result, AYA with cancer report high unmet service needs that affect negatively upon their quality of life. 21
The current status of AYA cancer education
Around the world, AYA cancer is emerging as a new subspecialty. 11 To respond to the needs of this group, appropriate education and training opportunities are required. 5 In Australia, the range of education and training opportunities for professionals is limited by the vast geography and relatively small population. In 2010, several national and jurisdictional projects were federally funded to address these issues, including development of post-graduate education (Certificate in Adolescent Health and Well-being—Oncology) 22 and a freely accessible online learning module in cancer. 23 While there is a range of useful sources of information, including Cancer Australia's Cancer Learning website, 14 for the bedside clinician, awareness of, access to, and availability of education and training remain limited. Participants in our study repeatedly reported their inability to attend educational and training opportunities because of clinical responsibilities. Our findings have identified there is an on-going need for the provision of educational opportunities, with a greater emphasis being placed on improving the knowledge and confidence of clinicians who provide care to this vulnerable group. Opportunities to work with the healthcare services to enhance access to education should be investigated, considering the issues highlighted by the health professionals who responded to our surveys. Our plans are to revise the content and format of the education program and continue to promote the education and support available through the QYCS with regular newsletters to cancer services throughout the state. An education framework is currently under development to provide learning opportunities for all classifications of health professionals from the beginner to advanced level, with the aim of supporting the learning needs of health professionals across the state.
Our study has notable limitations. Queensland is a large state with a widely dispersed AYA cancer population and a unique healthcare setting. Our findings may not be generalizable to other settings. However, given the consistent report of a need for education in palliative care for this age group, we believe this need is likely true of health professionals across the nation and internationally. The response rate for both surveys was low, even after a reminder notification; however, typical response rates for online surveys have been reported as low as 4%. 24 As a cross-sectional survey, our findings are suggestive rather than conclusive evidence of the educational needs of health professionals. In addition, we do not know what percentage of participants participated in the educational activities; while some participants completed paper surveys after attending workshops, this was a small proportion of the overall participant numbers in both surveys. The second survey was based upon the first survey, but did not go through the same process of review with an external expert group. Nevertheless, we have confirmed an ongoing appetite and desire for education and training opportunities for AYA cancer care professionals and this study has helped us to prioritize the content of topics.
Conclusion
We developed an educational program and investigated the educational needs for health professionals providing cancer care to adolescents and young adults. In two surveys undertaken in 2013 and 2017, we identified that majority of respondents had provided care to a young person with cancer. A high need for education regarding palliative care was reported in both surveys. Priorities for educational needs changed from a trend of biomedical aspects in 2013 to more practical and psychosocial aspects in 2017. Despite several years of delivery of the education program, there was no trend in responses over time that suggested improvement in self-reported confidence across domains. There is an ongoing need to provide regular and consistent education and training opportunities to support the developing workforce in AYA cancer care.
Footnotes
Acknowledgments
We wish to acknowledge the contributions of QYCS staff who developed the education framework and the many people who contributed to the development of the QYCS. The YCS receive federal funding through CanTeen as well as state and territory government funding. We would also like to acknowledge the work of Dr. Danielle Tindle (deceased), who advocated for the need for AYA cancer services in Queensland and contributed to the development of the initial survey.
Author Disclosure Statement
No competing financial interests exist.