
Abstract
Adolescents and young adults (AYAs) with cancer have unique needs around education and vocation during and after treatment. This narrative review series aims at documenting the unique needs of AYAs from the current literature and at providing recommendations to inform an update of the Australian National Service Delivery Framework for AYAs with Cancer. AYAs with cancer may experience impairments to cognitive, physical, and psychological functioning and health, which can adversely affect their academic grades, peer relationships, and likelihood of entering the workforce. Treatment expenses and time off work can stifle AYAs' financial independence from their parents. The combined effect of disrupted education, vocation, and financial dependence can reduce AYAs' sense of identity. Although support is available in some countries, support efficacy is yet to be clearly established. Continued research is required to deliver successful education and work reintegration programs that build the confidence of AYAs with cancer to achieve their best. Educational and vocational support, as well as financial advice, may improve AYAs' financial security and quality of life during survivorship.
Introduction
T
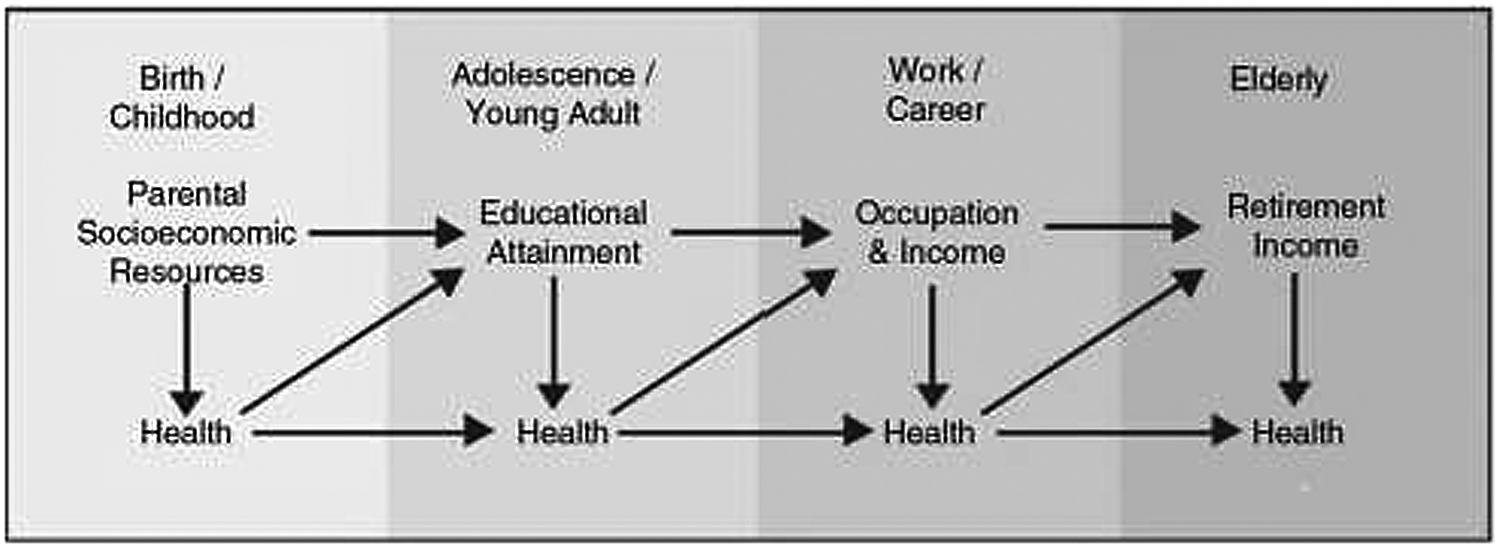
The dynamic and reciprocal relationships between socioeconomic status and health through the life-course (Source: Adler 1 ).
Cancer diagnosis and treatment can lead to cognitive impairments and changes to physical functioning and appearance.5,6 Due to ongoing school absenteeism and unique cancer experiences, AYAs with cancer may struggle to establish their personal identity or maintain high-quality peer relationships.7–10 AYAs with cancer may miss opportunities to develop social skills and the capacity to complete work tasks that are necessary for obtaining ongoing employment and financial security. 9 Further, not studying or working in the years after diagnosis can lead to greater distress among AYAs with cancer.3,11,12
Poor education and vocation outcomes can reduce later financial security, which, in turn, can impair AYAs' capacity to maintain good health in survivorship. The financial costs of treatment in addition to time spent away from work or education can slow AYAs' progression to financial independence from their parents, stifling their development of autonomy. 10 During treatment, AYAs and their families are impacted by out-of-pocket expenses (e.g., travel, accommodation, use of work-related entitlements, and changes in employment). 7 Financial burdens can extend beyond treatment, with AYAs incurring significant ongoing medical costs during survivorship. 8
In this narrative review, we examine past research exploring the impact of cancer during AYA years on education, vocation, and income. We aim at exploring the available evidence and gaps in the literature, providing recommendations for future research and practice.
Methods
We conducted a narrative review consistent with Economic and Social Research Council recommendations. 13 A narrative review is ideal for providing a broad overview synthesizing current empirical evidence and theoretical approaches. 12 We searched published peer-reviewed literature by using Medline, EMBASE, and PsycINFO (see Table 1 for search terms). Relevant reports were also identified by using two gray literature databases (OpenGray and Gray Literature Report). Key references published between 2010 and 2016 (inclusive) were identified by title and abstract review (J.E.F. and Kate Marshall [see acknowledgments]) to inform an update of the Australian National Service Delivery Framework for AYAs with Cancer. Additional key articles were obtained from reference list review. We screened articles for relevance, importance, quality, and potential clinical practice impact before inclusion (J.E.F., U.M.S.-D., C.E.W., A.L.). We included international articles of AYAs' experiences, adopting the broadest scope of ages defined as AYA (i.e., 12–40 years). 14 We included all cancer types.
“$” indicates truncation.
Results
Education
A combination of cognitive, physical, and psychological factors impact school attendance and functioning of AYAs diagnosed with cancer. Treatment-related cognitive impairments to memory, attention, and concentration occur in up to 50% of AYAs, and they may persist till 25 years post-diagnosis.6,11,15,16 Reduced emotional well-being and global self-esteem after cancer treatment can impair academic functioning and peer relationship quality and cause ongoing absenteeism. 3 Physical side effects of cancer treatment include hair loss, vision/hearing impairments, weight changes, scarring, amputation, and fatigue, which can reduce AYAs' desire to attend school and their capacity to complete schoolwork.2,3 Unsupportive teachers can reduce AYAs' sense of school belonging, causing AYAs to disengage from their schoolwork and peers.3,11,15 Ongoing absenteeism before, during, and after treatment can accumulate to between 40 days and 9 months off school, with irregular attendance up to 3 years post-diagnosis.2,3,11,15 This combination of risk factors adversely affects AYAs' capacity to complete schoolwork, and some AYAs may need to repeat a grade.3,11,15,16
Despite their additional needs, few AYAs report receiving additional or effective educational support. 11 Some charities offer AYAs tutoring or school reintegration support, but in other cases, parents pay tutors to help their child “catch up” on missed schoolwork, creating additional financial strain on the family. 15 Strong peer support can improve school reintegration by reducing AYAs' body image concerns, promoting AYAs' self-esteem. 2 Good communication between parents, health professionals, and school personnel can also significantly improve the likelihood of successful school reintegration.11,15 Further communication and coordination support between hospital, home, and school can be implemented by trained education professionals in the health setting, such as education liaison officers and learning mentors.2,3,15,17
We identified multiple gaps in the literature, such as the lack of research examining the impact of cancer on academic grades or special education provision (including education while homebound or hospitalized) of AYAs. We were also unable to identify AYA-specific intervention-based education research that used robust research designs, such as randomized controlled trials.
Recommendations from the literature
School reintegration support should begin at diagnosis and continue during and after treatment. 5 At diagnosis, health professionals can inform AYAs and their parents of cancer and treatment-related impairments to cognitive and educational functioning, and they may inform school personnel about treatment side effects that may affect completion of class activities, assignments, and exams.11,15,18 Schools can support the maintenance of peer friendships and school reintegration by providing opportunities for peer interactions in hospital, at home, or at school, or by using online technologies. 5 A structured liaison pathway between the hospital, home, and school can facilitate information sharing throughout treatment and improve AYAs' school reintegration experiences. 19 The most effective liaison pathways include a single, assigned personnel in both the school and hospital, as well as an external liaison coordinator to manage communication. 5
Vocation
Although the literature on employment in AYA cancer survivors is limited, some evidence indicates that employment rates of AYA survivors are below the general population,8,20 and that they experience limitations in work, housework, or education. 8 However, not all studies report reduced employment rates. 21 Poor cognitive functioning or reduced educational achievements, cancer of the central nervous system, cranial irradiation, and being female have been associated with higher rates of unemployment.6,9,19,21 AYA survivors are more likely to be part-time employed, older when starting their first occupation, 21 and in lower skilled jobs with lower pay compared with the general AYA population.8,20 AYA survivors report being unable to work due to illness or disability more often than the general population, 8 and some AYAs report discrimination and lack of employment opportunities as a result of having cancer. 22
Returning to work after treatment can be challenging for AYAs. One study of AYAs with non-central nervous system cancers reported that ∼70% of AYAs who were employed at diagnosis returned to full-time work or study 15–35 months after treatment but up to 50% reported ongoing difficulties with work or study. 23 Compared with employed AYAs, those who were unemployed before diagnosis were more likely to remain so. 23 AYAs report that their career plans were negatively impacted by cancer, 24 and that treatment caused them to miss opportunities for employment that may never be regained. 22
Work may provide a sense of identity and a social-professional network that promotes the psychological development of AYA survivors. 20 However, negative beliefs and feelings of hopelessness about their present situation can lead AYAs to have difficulties in making career decisions. 25
Considerable gaps in the vocation literature for AYA cancer survivors exist. Although some evidence is available regarding employment, stronger research designs are required to provide robust findings regarding employment rates (including terms of employment both during and after treatment), predictors of unemployment, satisfaction with vocation, and psychosocial and developmental factors associated with employment during adolescence and young adulthood, such as identify formation.
Although many hospital-based counseling and education programs support AYAs' vocational needs,26,27 few have been formally evaluated regarding the efficacy at promoting employment opportunities, ongoing engagement, and satisfaction with work.
Recommendations from the literature
Recommendations for AYAs' vocational needs are scarce in the literature. Strauser et al. 20 have proposed a model of career development in AYAs with cancer, which takes into account the context of the individual and their environment, their stage of career development (e.g., educational attainment), and their capacity to participate (Fig. 2). Service providers can use the model to identify AYAs' specific needs and strengths, and implement tailored strategies to improve AYAs' vocational success. 20 Combining datasets through international collaborations may help establish stronger evidence related to vocation in this niche population, and provide more robust evidence to inform services to support AYAs in their career choices and development.
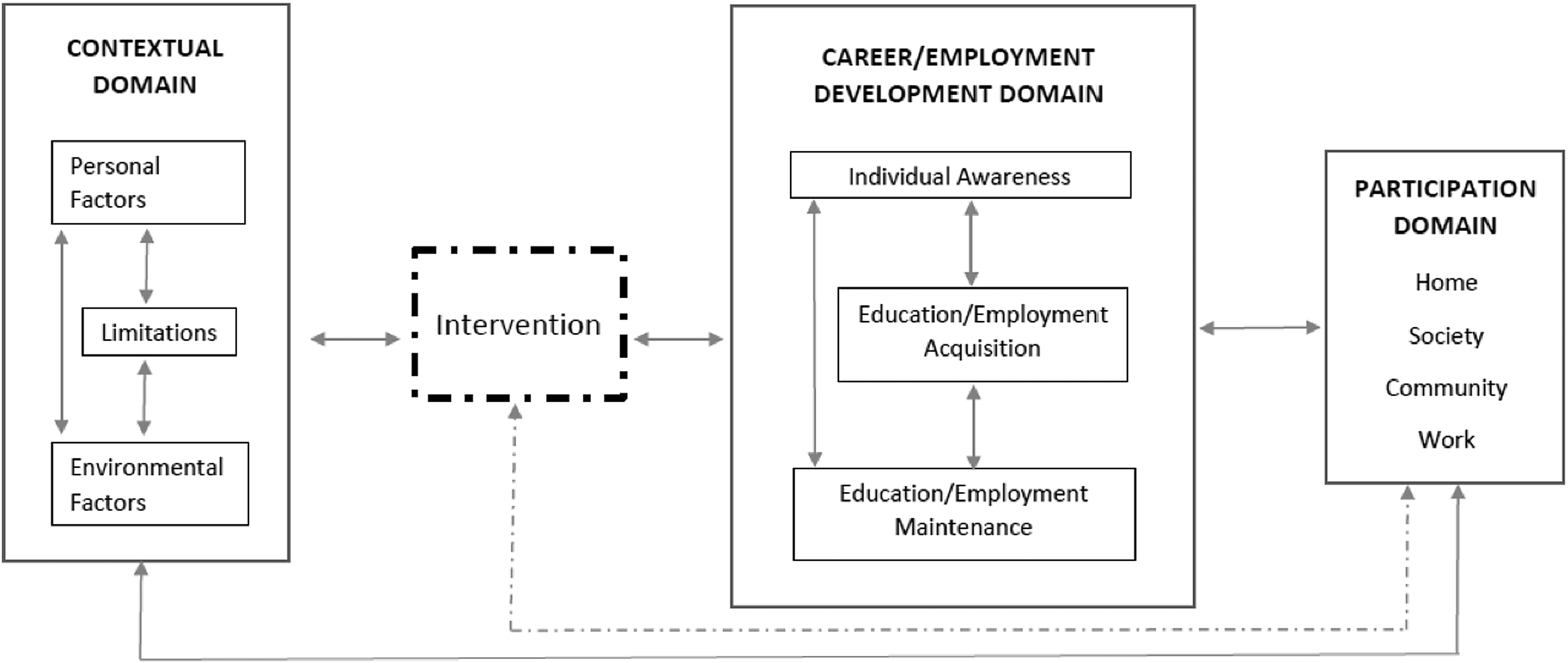
Conceptual model for career development for young adult cancer survivors (Source: Strauser et al. 20 ).
Financial
The financial cost of cancer treatment impacts AYAs and their families both during and after treatment. Parents rate the financial burden of treatment as one of the greatest challenges, and often struggle to return to full-time work after AYAs return home from hospital-based treatment due to ongoing care needs. 28 The combination of treatment expenses not covered by health insurance and time away from paid work may mean that young adult survivors are faced with a “double whammy” that stifles financial independence from parents and causes significant personal debt during survivorship. 29 Approximately 60% of AYAs report that cancer has a negative impact on their financial situation, 24 with indications of higher annual medical costs (US$7417) and lower family incomes compared with adults of a similar age (US$4247). 8 AYAs with higher socioeconomic backgrounds may be able to better access care for ongoing health concerns, whereas AYAs with fewer socioeconomic resources are at risk of further reduced physical health and quality of life. 29
Norwegian AYA cancer survivors are more likely than the age-matched population to be reliant on funding from a national insurance scheme for ongoing care-related costs, or disability due to cancer and its treatment. 30 AYAs in the United States who lack public, private, or employment-based healthcare cover or insurance are more likely to decline recommended follow-up care or screening due to costs when compared with AYAs with health insurance. 23 In Australia, although many residents are privately insured, most of the costs of medical treatment are covered by a universal healthcare scheme, Medicare, financed by a levy administered through the tax system. However, in a study by Cohn et al., the “hidden costs” of survivorship care for Australian childhood cancer survivors were identified as a significant barrier to attendance at survivorship clinics. 31 Although there may be no cost to the clinic itself, the hidden costs, including the loss of a day's employment and travel costs, are unlikely to be covered by insurance, thus adding further financial strain to AYAs and their family.
There is little evidence available to draw firm conclusions regarding the financial status of AYAs after cancer diagnosis. The costs associated with treatment and returning to work are likely to be different both within and across countries, meaning that cross-cultural generalizations may be unreliable. Psychosocial experiences associated with financial burden or insecurity related to AYA cancer are also largely unknown.
Recommendations from the literature
Affordable ongoing care should be a priority. AYAs and their parents may require support and information on how to manage their finances after treatment. As the financial implications of cancer treatment are likely to be country specific, further research on financial costs of cancer during AYA years in the context of a country's available healthcare is needed. Further research should also examine the use of private health insurance for cancer treatment among AYAs and its financial implications, including out-of-pocket expenses. Research exploring the dollar value of specific hidden costs is also warranted to better understand how the financial impact can be addressed (e.g., insurance coverage of health-related travel).
Conclusions
The educational, vocational, and financial needs of AYAs diagnosed with cancer may be significant. A range of cognitive, physical, and psychological factors related to cancer and its treatment can adversely affect the process of reintegration into education and employment, and of gaining financial independence. Some AYAs may no longer be able to achieve their pre-diagnosis aspirations. Support models are available (particularly regarding educational supports), but there is insufficient evidence on the effectiveness of these models. Further research is needed to ensure the delivery of evidence-based practices promoting developmentally appropriate education, employment, and financial security for AYA cancer survivors.
Structured hospital-to-school liaison pathways to inform educators and provide peer interactions are currently available in some countries, yet require further empirical evaluation in terms of their benefits to AYAs' physical and psychosocial health and academic outcomes, including grades and education attainment.5,19 Research exploring support pathways for AYAs to start or return to work post-diagnosis based on their individual level of skills and functioning as well as the vocational climate in which they live is warranted. 20 Such research should focus on translatable outcomes, for example, the location of support pathways (i.e., the hospital or community) and the timing of support delivery. A fuller understanding of the costs of cancer is required, including costs related to treatment, follow-up, lost employment, and psychosocial implications. 28 Research that explicitly links the impact of cancer on education, vocation, and finances in AYAs will enhance researchers' and support providers' capacity to deliver targeted support that benefits AYAs' independence and development.
Footnotes
Acknowledgments
The authors would like to thank Kate Marshall for her contribution to this research. This research was supported by CanTeen. C.E.W. is supported by a Career Development Fellowship from the National Health and Medical Research Council (NHMRC) of Australia (APP1067501). J.E.F. is supported by The Kids Cancer Project. U.M.S.-D. is supported by an Early Career Fellowship from the Cancer Institute of New South Wales (ID: 14/ECF/1-11) and an Early Career Fellowship from the NHMRC, Australia (APP1111800). The Behavioural Sciences Unit is proudly supported by the Kids with Cancer Foundation and by the Kids Cancer Alliance as well as a Cancer Council New South Wales Program Grant PG16-02 with the support of the Estate of the Late Harry McPaul.
Author Disclosure Statement
The authors wish to declare no competing financial interests.