
Abstract
Purpose:
Our goals were to evaluate young adult lymphoma survivors' perceptions regarding benefits of exercise after cancer treatment, to identify barriers to exercise, and to understand the types of exercise interventions that may be useful in this patient population.
Methods:
Young adult lymphoma survivors were invited to participate in a survey and focus group. Questions focused on elucidating barriers to exercise as well as potential opportunities for supporting patients in adequate exercise. Focus groups were audiorecorded and transcribed, and data were coded inductively for themes and applied findings.
Results:
Eight survivors participated. Findings were categorized into five main themes: barriers to exercise, facilitators of exercise, personal responsibility for being active, interconnectedness of exercise with a healthy lifestyle, and recommendations.
Conclusions:
Fatigue and frustration with postcancer physical limitations are major barriers to exercise for young adult survivors, whereas support from others, data tracking, and survivor-specific resources are facilitators. Interventions that incorporate fitness tracking technology, are individually tailored, and/or create a community with other young adult survivors may be successful in this population.
Introduction
A
Reflecting similar findings in the general population, studies in cancer survivor populations also show an association between physical activity and reduction in cardiovascular disease risk factors and cardiovascular events.9–14 Furthermore, physical activity has been shown to improve fatigue levels, increase QOL, and decrease risk of long-term complications.15–18 Disease history, treatment history, and lifestyle factors unique to survivorship in emerging adulthood come together for poorer health. Physical activity is a simple but powerful tool for combating late effects of cancer treatment.
Asking survivors how healthcare institutions can support healthy behaviors, including physical activity in age-appropriate ways can inform interventions that might be tested for efficacy. We sought young adult lymphoma survivors' stories and opinions to provide a better understanding of exercise in survivorship and to inform future interventions. The goals of our study were to evaluate young adult lymphoma survivors' perceptions regarding benefits of exercise after cancer treatment, to identify barriers to exercise, and to understand the types of interventions that might be successfully employed.
Methods
Research design and approach
A mixed methods approach, incorporating data from participants' electronic medical records, questionnaires, and focus group interviews, was employed to explore young adult survivors' perceptions and experiences of exercise after cancer treatment. Qualitative research is valuable for in-depth exploration of subjects' realities. 19 This study was grounded in interpretative phenomenological analysis (IPA), which is a qualitative methodology from social psychology that focuses on understanding individuals' personal experiences and how they make sense of their social worlds. 20
Recruitment
IPA provides flexibility for use with a purposeful sample in identifying research participants who are able to describe specific experiences, such as experiences with exercise after cancer treatment.20,21 Eligible participants were young adult survivors of AYA lymphoma who met the following criteria: ages 18–35 years, live within 120 miles of our institution, 6 months to 5 years posttreatment as well as those in disease remission who are being treated with immunotherapy, and English speaking. Fifty-four patients were identified as eligible from an institutional database and were invited to one of two focus group interview dates through mail invitation and follow-up phone call. Institutional IRB approval was obtained. Informed consent was provided by all participants.
Data collection
Data were gathered between June and August 2016. Background data for participants were collected from the medical record. General comorbidities as well as neuropathy and psychiatric diagnoses were pulled from the medical record to be analyzed with a modified Charlson Comorbidity Index. 22
Focus groups were conducted in the evening to accommodate young adults' busy schedules. “Part 1” of each focus group's evening involved participants individually filling out questionnaires and “part 2” involved the focus group discussion. For part 1, participants completed a questionnaire consisting of the cancer survivorship QOL questionnaire, 23 the Godin exercise questionnaire, 24 and additional questions to determine perceptions of the clinical evidence for exercise after cancer treatment. Following the questionnaires, part 2 involved an audiorecorded focus group interview, conducted using a semistructured interview guide. Two focus group sessions were ultimately conducted, with five participants in the first and three in the second.
Given that our participants may not have been in a group with other AYA survivors before, particular ethical consideration was made to ensuring emotional safety, including making participants aware that they did not have to answer any questions that they did not wish to, introducing the researchers and their backgrounds, and using warm up questions that allowed participants to share their stories if they chose to. A moderator guide established topic areas, but moderators were receptive to discussion that veered toward new topics participants found important. At the end of the event, participants were invited to contact a study team member through email should they have additional content to add. Two participants followed up with additional information and that was added to the data for analysis.
Data analysis
Godin Leisure-Time Exercise and Cancer Survivorship QOL measures were scored according to published algorithms.25,26 The Godin Leisure-Time Exercise questionnaire calculates a leisure activity score based on the number of periods of exercise for more than 15 minutes that a person participates in per week. 24 Those periods get weighted more heavily for strenuous greater than moderate, greater than mild activity, and a final score of active, moderately active, or sedentary is calculated. This tool assesses leisure-time recreational activity, or exercise, and does not necessarily assess nonrecreational physical activity, such as occupational activity or activities of daily living.
The Cancer Survivorship QOL questionnaire involves 41 items rated on a 10-point scale. 23 The tool attempts to quantify QOL using a biopsychosocial model, with questions in the physical, psychological, emotional, and spiritual realms. Questionnaire responses and chart review data were used as descriptive demographic data to aid in interpreting individual responses in the focus group interviews.
Audio recordings of focus group interviews were transcribed verbatim, de-identified, and the written scripts reviewed for accuracy. Transcripts were analyzed inductively using a thematic approach as described by qualitative researchers21,27–29 and principles of IPA. 20 In line with IPA, each transcript was analyzed with consideration to individual experiences as well as themes that emerged within and across different perspectives.
The analysis process involved reading the data and identifying important codes and themes. Two independent coders developed code lists based on an initial read. Similar themes were combined and definitions for the categories were developed and refined to create a code manual. The code manual was used for double coding of each transcript. Discrepancies in individual coding were examined, discussed, and debated until consensus was derived. Nvivo 10 software (QSR International, Pty. Ltd.) was used to manage data and facilitate analysis.
Results
Part 1: participant characteristics and questionnaire responses
Invitations resulted in eight participants for a participation rate of 15.4%. Reasons cited for nonparticipation included scheduling conflicts and distance from study location. Participant characteristics are summarized in Table 1. Demographic differences between those who agreed to participate versus those who did not agree to participate can be found in Table 2. Participants did not have chronic medical conditions measurable by the Charlson Comorbidity Index, but did have health conditions not included in the index that were diagnosed postlymphoma, including hypothyroidism, depression, and anxiety. QOL data can be found in Table 3 and self-reported exercise habits in Table 4. Data on perceptions of exercise benefit can be found in Figure 1. When asked about whether their doctor or someone from their doctor's office had talked to them about exercise recommendations, 87.5% indicated “yes, a little bit,” 12.5% indicated “yes, a lot,” and no one indicated “no, not at all.”
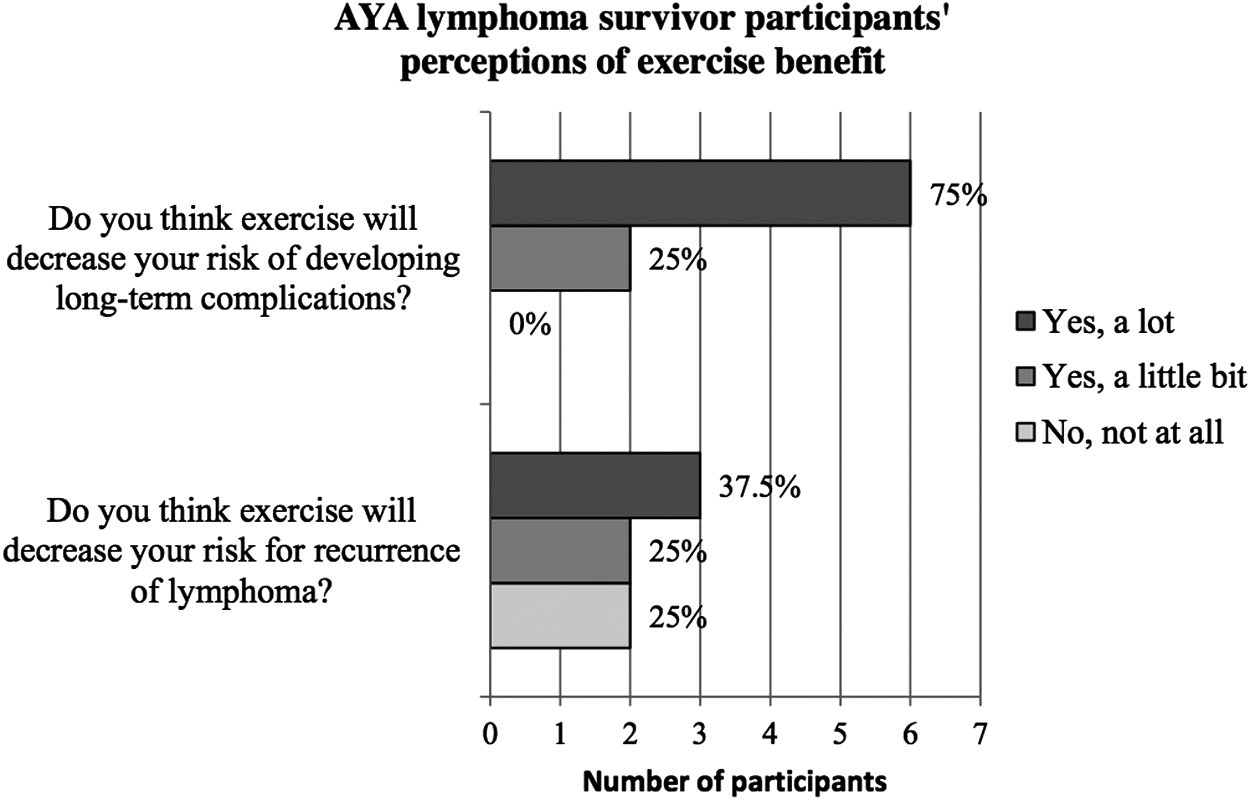
Perceptions of exercise benefit. Answering “Do you think exercise will decrease your risk for recurrence of lymphoma?” one patient wrote in “Yes,” but did not choose “Yes, a little bit” or Yes, a lot.” This response is not reflected in the above data.
BMI, body mass index.
Indicates value for which one participant was not included due to incomplete questionnaire.
Part 2: qualitative findings
Findings for this study are categorized into five main themes, which can be found with representative quotes in Table 5.
AYA, adolescent and young adult.
Barriers to exercise
Barriers reported include fatigue, frustration with postcancer physical limitations, lack of time, competing demands, boredom with exercise routines, and a lack of knowledge about AYA cancer survivor-specific resources. Participants described a need to budget energy, often putting exercise at the bottom of a long list of important tasks. Describing an often discouraging quest to return to a precancer level of physical functioning, participants talked about having to “relearn their bodies.” Anemia, pain, weight gain, loss of endurance, and reduced muscle mass after treatment were cited as contributing factors to posttreatment fatigue and a new, frustrating postcancer body overall. Additionally, participants described the compounding barrier of peers not relating to or understanding this new normal.
Facilitators of exercise
Support from others, ability to track activities, and easy access to cancer survivor-specific resources were identified as facilitators of exercise. Support from loved ones or even a doctor provided a level of accountability. This supportive network was also inherent to the cancer survivor exercise programs that participants identified as useful. LIVESTRONG at the YMCA was described as having been helpful for those with young families by providing free membership for children and spouses. Other programs geared specifically toward young adult survivors, such as First Descents, were found to be helpful in providing connection to other AYA survivors. Many participants also said that exercise is more fulfilling when they track their activities and other health-related data on apps or through wearable technology.
Personal responsibility for being active
Personal responsibility was reported as both a barrier to and facilitator of exercise. It was frequently cited as a barrier to a doctor or healthcare institution helping survivors become more active. They felt that a healthcare institution can put resources into facilitating exercise, but that a lack of intrinsic motivation will ultimately trump those efforts. On the side facilitation, some described an “aha moment” in which they made a decision to get fit after treatment and then succeeded in that plan because of intrinsic motivation.
Participants did not have specific advice on how to promote motivation, but they did report specific approaches that they felt do not work. In particular, participants felt that a physician telling them to exercise in a generic way is not helpful and that an exercise prescription would not be motivating. Some equated this to a dentist telling you to brush your teeth; patients already know that they should be brushing their teeth (or exercising, for that matter), and simply telling them to do so is ineffective.
Interconnectedness of exercise with a healthy lifestyle
The interconnectedness of different elements of a healthy lifestyle with exercise was discussed extensively. Many felt that eating healthy food was important for feeling energized to exercise. Individuals also discussed weight gain during or after treatment and emphasized that eating healthfully was important for getting back to their precancer weight. Some shared that they were under the impression that they should be eating prepackaged, unhealthy foods during treatment to avoid fresh fruits and vegetables. They felt that this impression was instrumental in developing poor eating habits while receiving chemotherapy and led to poor eating and exercise habits after treatment.
Participants also emphasized a mind–body connection. A healthy mental state was reported as vital to healing overall, let alone becoming physically active, after treatment. Some participants felt that their mental health was more shaken after cancer than their physical health, and that this aspect had yet to be addressed. Others said that for them, it would be impossible to become more physically active before their mental and psychological wellbeing was improved. Some described healing practices with a mind–body connection, such as meditation or yoga, as useful in addressing the health of AYA survivors on a more holistic basis.
Recommendations
Primary recommendations were fitness apps and wearable technology, cancer survivor-specific exercise groups, and personalized plans. Participants felt that fitness apps and wearable technology offer many beneficial potential features such as the ability to share data with their clinician, connect virtually with other cancer survivors, track progress, and incorporate other wellness aspects, including survivor-specific issues such as treatment-related symptoms that might affect activity level.
In terms of a cancer survivor-specific group, participants thought that such a group could provide social support in addition to exercise support. A group that is similar in age was viewed as the most important characteristic of a survivor exercise group, while being disease-specific was viewed as unimportant. Some even said that all young adults dealing with any chronic illness should be included. When asked about paying for or traveling to such a group, participants felt that it would have to be available within a half an hour of their home and at very little cost.
Highly individualized plans with attention paid to personal activity preferences as well as disease and treatment type were also described as significant. In addition to individualization based on activity preferences, participants also wanted individualized advice based on their particular wellness barriers.
Discussion
Our participants were aware of the importance of exercise in survivorship, and all indicated that someone from their healthcare team had talked to them about exercise in survivorship. As they elucidated in the focus groups, however, knowledge is not enough.
Research suggests that social networks can be beneficial in promoting exercise. 30 Our participants felt that survivorship groups should be similar in terms of age (oriented toward young adults), but that the particular disease subtype (lymphoma) was less important. Communities for AYA survivors that incorporate exercise exist already and supporting existing endeavors as well as connecting young adult survivors to these resources would be an accessible first step to better supporting this population. This would require providers to have a basic awareness of the AYA resources available, access to resource databases, and/or the ability to connect patients with another member of the healthcare team with this knowledge.
The participants in our study reported strong interest in fitness trackers and smartphone applications to manage activity data, share data with providers, and connect with other AYA cancer survivors around fitness. This has implications for providers, who could personalize recommendations based on individual data. There is significant interest in the oncology community for utilizing mobile technology to connect with patients outside of clinical encounters. A tablet computer-based self-assessment between clinic visits was shown to improve QOL, decrease emergency room visits, increase time on palliative chemotherapy, and improve survival in adults with advanced cancer.31,32 There is a need to study the role of mobile technology in our target population.
Our participants also felt that survivorship care should focus on the wellbeing of the whole person, rather than just specific aspects such as exercise. They felt that the timing of these survivorship wellness discussions should optimally occur 1–3 months after treatment, as opposed to 1–5 years later as they often do today. Participants desired comprehensive, highly personalized advice, such as detailed nutritional recommendations based on their cancer history.
We hypothesize that this need for intensive, individualized survivorship care may stem from the psychosocial needs of AYA survivors immediately after treatment. While being treated for cancer, patients have significant medical oversight and often build strong bonds with their cancer team. The transition from treatment to survivorship may feel abrupt. 33 Thus, they may need a more graded, hands-on approach to survivorship care than what is currently being provided. Participants suggested an interdisciplinary cancer rehabilitation program. These programs exist in some places, but are expensive to implement and may be difficult for patients who do not live near the facility to access.
Limitations to our study include low participation rate and small study size. However, because the focus group format allowed participants to build off ideas of one another, we developed a rich data set for thematic analysis. As shown in Table 2, the average distance between home and the study site was greater for those who did not participate compared to those who did. Also, there was a larger proportion of participants who underwent stem cell transplant who participated, compared with those who did not. We hypothesize that perhaps those young adults who have undergone more extended and intensive treatment may feel a greater desire to connect with peers who have undergone similar experiences, and thus may be more prone to participating in a focus group like this one.
A limitation for broad application of these findings was the racial and ethnic homogeneity of our study group, which is reflective of the demographics of our patient population as a whole. Because participants were recruited from an institutional database which is maintained by the adult hematology practice, our sample was also skewed toward the older end of the young adult age group. Another potential limitation was that our group reported more exercise compared with other cancer survivors.34–37 In comparison to another study which found only 48.7% of their AYA survivor participants to be meeting activity guidelines after treatment, we found 75% of our survivors to be sufficiently active. 38 It's possible that some of this difference may be due to a small sample size, but we cannot rule out self-selection bias.
Strengths of this study include similar characteristics between our group and cancer survivors as a whole and detailed qualitative data to elucidate a complex issue. To our knowledge, this is the only study of its kind that is lymphoma specific. Research suggests that lymphoma survivors area particularly at-risk group for being overweight or obese and for having poorer health-related QOL, highlighting the need for disease-specific research. 3 Furthermore, our study identified similar themes to those reported by other groups, strengthening the validity and generalizability of these findings.39,40 Our study is different from previous work in that we asked survivors about the particular kinds of resources or interventions that would be helpful to them, a theme which is summarized under “recommendations” in Table 5.
The results of this study are a call to reexamine the role of interdisciplinary care for AYA cancer patients and survivors. A truly integrative approach to health after treatment is beyond the scope of hematology/oncology practitioners alone. Primary care providers, social workers, psychologists, community groups, colleges and universities, and other players must be engaged to create the type of social network that will support wellness in this population. Hematology/oncology practitioners must also recognize the significance of and ask about psychosocial needs of AYA cancer survivors and address them adequately.
Conclusions
Fatigue and frustration with postcancer physical limitations are major barriers to exercise for AYA lymphoma survivors, whereas support from others, data tracking, and survivor-specific resources are facilitators. Many AYA survivors see exercise as inseparable from other aspects of wellness such as mental state and nutrition. Interventions that incorporate fitness tracking technology, provide variety, are individually tailored, and/or create community with other AYA survivors may be successful in this population.
Footnotes
Acknowledgments
This study was funded by Arnold and Kit Palmer Benefactor Award. It was approved by the Mayo Clinic IRB.
Author Disclosure Statement
No competing financial interests exist.