
Abstract
Adult hepatoblastoma (AHB) is a rare liver tumor with a poor prognosis in adolescents and adults. This contrasts with hepatoblastoma in children and is not fully understood. Here we describe two adolescents with AHB who were treated in our hospital. Adolescents are likely to receive less intensive chemotherapy protocols and are treated in hospitals with less experience in pediatric oncology, resulting in poor outcome. More research is necessary for optimal treatment of AHB in adolescents. Adolescents with AHB should be referred to hospitals experienced in pediatric oncology and receive intensive chemotherapy, followed by hemihepatectomy.
Introduction
A
Patient 1
An 18-year-old otherwise healthy female was admitted to our hospital in 2010 with progressive fatigue, pain, and a growing swelling in the right upper abdominal quadrant. Her weight was stable and she had no other gastrointestinal complaints. Her family history was negative for liver malignancies or liver disease. On physical examination, a healthy young female was seen. The liver was palpable 5 cm below the right costal margin, mobile with respiration.
An elevated alpha-foetoproteine (AFP) of 114,000 μg/L (<20 μg/L) was the only abnormal laboratory result. Hepatitis serology was negative.
Computer tomography (CT) and additional magnetic resonance imaging (MRI) revealed three liver lesions in segments 2, 3, and 4 (Fig. 1). All three lesions showed inhomogeneous enhancement on multiphase CT. There was no arterial or slow venous enhancement. The largest lesion had a diameter of 8 cm (Fig. 1A–D). Tumor invasion in the venous portal system was seen (Fig. 1C). On MRI, a washout phenomenon was present in the lesions, as were signs of an enhancing (pseudo-) capsula on delayed scans (Fig. 1D–H). No lymphadenopathy or metastases were seen.
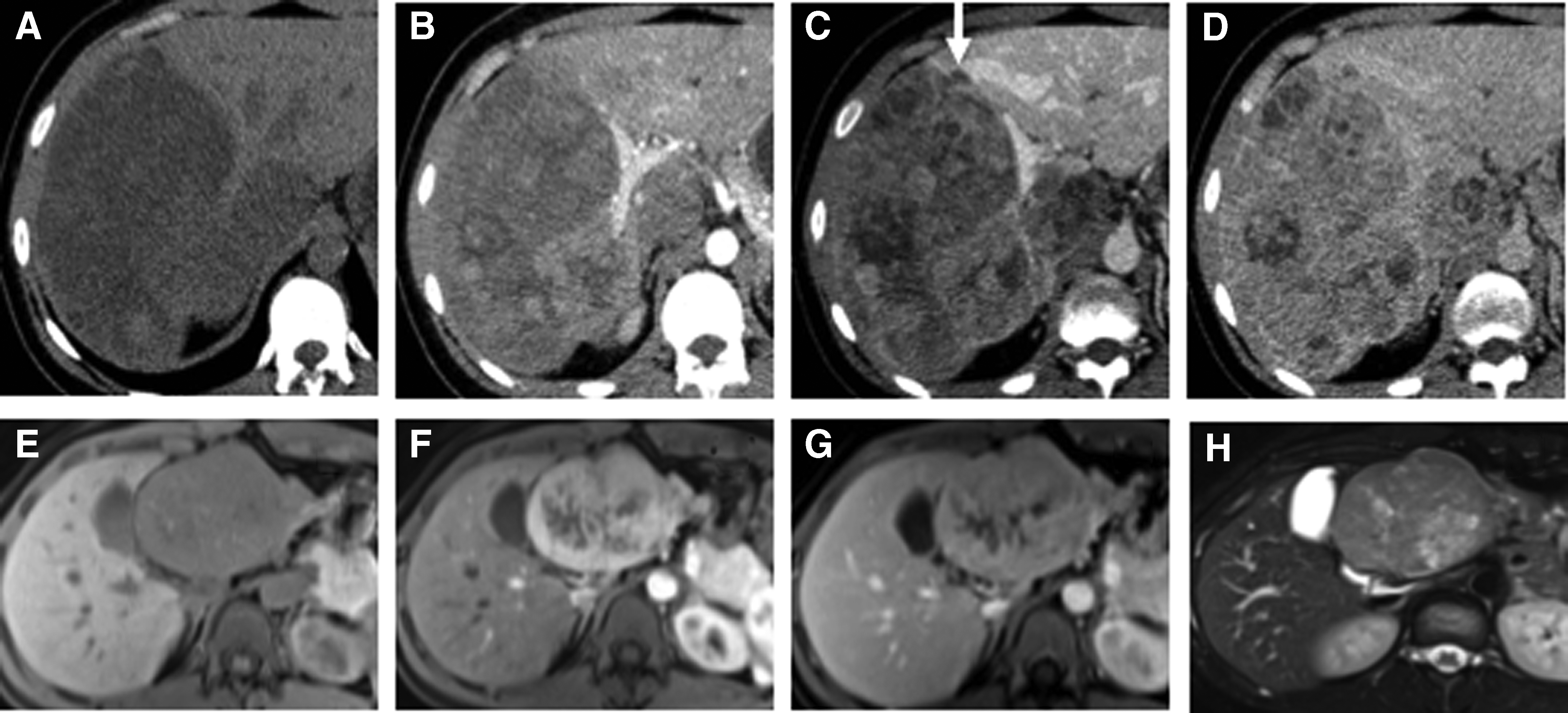
Transversal CT and MRI sections of the liver tumor in patient 1. Transversal multiphase CT
Microscopical examination of an ultrasound-guided biopsy proved malignancy. The distinction between AHB and hepatocellular carcinoma (HCC) was difficult, but the histomorphology (Fig. 2A, B) and clinical presentation, with a very high AFP, made the diagnosis of AHB most likely. Preoperative chemotherapy followed by hemihepatectomy was indicated. After two courses of cisplatin induction chemotherapy resulting in reduction of tumor size and AFP, an uncomplicated extended left hemihepatectomy was performed with partial resection of segment 8. Pathology showed tumor-negative resection margins and the diagnosis of an AHB was confirmed. In the histological sections, cuboidal cells, dense sheets architecture, and small tumor cells could be recognized, resembling fetal liver cells, typical for the fetal type AHB (Fig. 2A, B). Two adjuvant cycles of cisplatin were given after resection. This patient is currently well with no evidence of disease 5 years after surgery.

Histological sections of the tumor pathology specimens after resection from patient 1
Patient 2
An 18-year-old man, healthy except for hypercholesterolemia, presented in 2013 with 20 kg weight loss within 3 months, nausea, vomiting, and a sharp pain in the right upper abdominal quadrant. His family history was negative for liver malignancies or other liver disease. On physical examination, a healthy adipose male with normal vital parameters was seen. The liver was palpable 3 cm below the right costal margin.
Additional examinations showed abnormal laboratory findings: alkaline phosphatase 352 U/L (<125 U/L), gamma glutamyl transpeptidase 668 U/L (5–50 U/L), aspartate aminotransferase 115 U/L (<45 U/L), alanine aminotransferase 167 U/L (<50 U/L), and AFP 110,000 μg/L (<20 μg/L). Hepatitis serology was negative.
The CT sections showed a lobulated inhomogeneous mass of 17 cm in diameter. In addition, on MRI a lobulated mass consisting of multiple nodular lesions with intermediate signal on T1w was seen (Fig. 3). The tumor had arterial enhancement except for large irregular central lesion that showed partial enhancement and central feeding arteries (Fig. 3B–E). There was a high signal intensity, suggesting a scar-like tissue was present. (Fig. 3F).

Transversal MRI sections showing the liver with the tumor of patient 2. In images
Biopsy showed a multinodular and predominantly embryonal type AHB. Preoperative chemotherapy followed by hemihepatectomy was indicated according to the pediatric protocol. The patient received standard neoadjuvant cisplatin chemotherapy of two courses, to which doxorubicine was added for two cycles, because of a poor response. Reduction of the tumor and a decrease of plasma AFP were seen after the two additional cycles of chemotherapy. An extended hemihepatectomy of the right hepatic lobe including segment 4 was performed (Supplementary Fig. S1A; Supplementary Data are available online at www.liebertpub.com/jayao). The right adrenal gland was also resected en bloc due to tumor ingrowth. A cavatomy was necessary to resect an intravascular tumor thrombus (Supplementary Fig. 1B). The tumor was radically resected with tumor-free margins and the patient received adjuvant chemotherapy.
Definitive pathology confirmed a tumor with histological so called light and dark pattern. Areas with small cuboidal cells with eosin cytoplasm and round nuclei were also seen, suggestive for a fetal type AHB (Fig. 2C). However, compact tumor fields with cells containing less cytoplasm, a high nuclear–cytoplasmic ratio, and more mitosis were present, suggestive for a component of embryonal type AHB (Fig. 2D). The patient died 1 year and 3 months after the resection due to widespread metastasis, for which he received both palliative chemotherapy and radiation therapy.
Discussion
Including the present 2 cases, there are 70 cases of AHB currently reported in the literature. Both our patients presented with gastrointestinal complaints, hepatomegaly, extremely high AFP, and a liver mass on imaging. The second patient had hypercholesterolemia, which is very uncommon at this age. This has been reported previously as a first manifestation and negative prognostic factor in children with hepatoblastoma. 10 First the differences in survival are discussed, followed by suggested explanations for these discrepancies, the histology, or the differences in treatment. Lastly, better treatment of hepatoblastoma in adolescents is suggested.
When diagnosed with AHB, both patients were 18 years old. The mean age at diagnosis of AHB is reported to be 42 years. 1 Wang and Liu reported that prognosis is relatively better in patients <50 years, with a 1-year survival of 41.2% compared with a 1-year survival of 10% in patients older than 50 years. 8 Darbari et al. reported four cases of hepatoblastoma between 15 and 19 years old with a 1-year survival rate of 75% and a 5-year survival of 25%. 11 These survival rates are very poor compared with the 85% 10 years survival reported in children. 9 Differences in histological identity, pathological behavior, or treatment strategies at different ages could explain this remarkable gradual decline in survival rate with age.
Although tumor characteristics of AHB and HB overlap, there are some interesting differences in histological hallmarks and their metastatic behavior. In HB, pulmonary metastasis may be seen as in AHB, but in the latter, lymph node and peritoneal metastases have been found, which do not occur in children.1,7 Furthermore, there is a close histological resemblance between AHB and HCC in contrast to HB in children. Differentiation between HCC and AHB is essential, because the (A)HB is chemosensitive but HCC is not. Differentiation between AHB and HCC may be difficult as there can be both morphological and immunohistochemical overlap.2,7,12,13 Moreover, AHB and HCC have been described in patients simultaneously, both as mixed tumors and sequentially.4,14,15 The difference in survival rates, close histological resemblance, and difference in metastatic behavior between HB in children and AHB suggests that AHB cases may have been misdiagnosed for HCC or contain contents of HCC as stated by Rougemont et al. 7 Obviously, these cases will negatively influence the overall survival in the AHB group.
In addition, the pathological diagnosis of AHB is extremely difficult and can only be made with support of laboratory findings, imaging, and the clinical context. AHB can histologically be divided into the epithelial type and the mixed type, which contains epithelial and mesenchymal cells. 16 The latter is the most common type, accounting for 45% of AHB. 17 The epithelial type hepatoblastoma can be subdivided into fetal and embryonal subtypes. Both patients had an AHB of the fetal subtype. The second patient, however, also had parts with characteristics of an embryonal subtype. The embryonal subtype is less differentiated than the other types and has a poorer prognosis. 7 These subtypes, however, are equally distributed in both HB and AHB.
Worse outcome in adolescents has been observed in other pediatric malignancies that occur in adolescents and could explain the differences in overall survival. Adolescents are more likely to receive insufficient treatment in comparison to children.18,19 This phenomenon has been described in both hematological and solid tumors. Adolescents with hematological tumors have a better outcome with intensive chemotherapy regimens, which are standard therapy in children compared with less intensive adult hematological protocols.20,21 Young adults, however, receive more likely adult chemotherapy regimens and cannot always endure pediatric protocols, resulting in a worse overall survival. Furthermore, adolescents with hematopoietic malignancies who are not referred to specialized hospitals for pediatric malignancies risk a worse outcome.19,21 These studies suggest that adolescents with AHB benefit from referral to a hospital with a multidisciplinary team specialized in care for pediatric tumors, where they should receive intensive chemotherapy according to pediatric protocols.
The cornerstone of therapy in pediatric HB is surgery and chemotherapy according to the SIOPEL protocols. 22 Limited evidence suggests that both strategies also improve survival in AHB.7,23 Surgical resection of AHB in adolescents improves 1-year survival from 0 to 44%–60% compared with patients who did not undergo resection. 8 Evidence for improved survival rates after chemotherapy in AHB is not available, but is evident in HB. 22 Neoadjuvant chemotherapy is advised in AHB since chemotherapy reduces the risk of bleeding and reduces tumor size for surgery, which was also observed in both of our patients.24,25 Liver transplantations have shown good results in children with HB, wherein radical resections seem difficult and unlikely. 7 This could be considered in selected patients with AHB. The overlap between HB in children and AHB in adolescents supports the suggestion that this is the same entity, and that adolescent and pediatric HB should be treated identically.
In conclusion, despite the lack of evidence, we believe that AHB in adolescents should be regarded as a variation of pediatric HB. Current literature for treatment of AHB is insufficient and inconclusive. Therefore, more research is necessary for optimal treatment. Adolescent AHB may well be classified according to the PRETEXT score and treated according to the SIOPEL protocols with neoadjuvant chemotherapy followed by radical liver resection (www.siopel.org). Treatment of adolescents with AHB should be limited to hospitals with multidisciplinary teams experienced in pediatric malignancies, particularly in HB, combining intensive chemotherapy regimens and surgery as applied to children.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.