
Abstract
Purpose:
To describe fecundity in female survivors of childhood cancer and consider the correlation with quality of life (QOL).
Materials and Methods:
Of 1744 women treated for childhood cancer before the age of 15 years at one of eight French cancer treatment centers between 1948 and 1992, 1187 who were alive in 2005 were sent a self-administered questionnaire, including questions about health status, QOL (MOS SF-36), and fecundity. A standardized fecundity ratio (SFR) was calculated (SFR: observed/expected number of children) for each individual based on a national reference.
Results:
Of the 972 individuals (82%) who responded, 53% had at least 1 child. The overall SFR, 0.65, was dependent upon the initial diagnosis, more decreased in Central Nervous System tumors (0.24; p < 10−3) than in Germ cell (0.46; p = 0.03) or Sympathetic Nervous System tumors (0.79; p = 0.02). The average QOL motor score was 72.5 ± 19.5, and the average mental score was 61.4 ± 16.7. After adjusting for age, pathology, and self-reported sequelae in the questionnaires, it was determined that SF-36 mental (p = 0.002) and motor (p < 0.0002) scores correlated positively with fecundity, and SF-36 scores correlated negatively with locomotor late effects (p < 0.0001), growth insufficiency (p = 0.002), and psychological disorders (p < 0.001). Gonadal insufficiency was correlated with neither motor nor mental scores.
Conclusion:
Women treated for childhood cancer demonstrated impaired fecundity that correlated with poor QOL, as registered by the SF-36. Patients should be warned of the risk of impaired fecundity early during the follow-up. If possible, preservation of fertility should be prioritized at initiation of therapy.
Introduction
P
In this study, we investigated the fecundity of female, childhood cancer survivors (CCSs) for the purpose of evaluating risk factors associated with decreased fecundity, and the effects of reduced fecundity on overall quality of life (QOL).
Materials and Methods
Patients
The population was derived from two previously described cohorts:
The French population of the Euro2K cohort included 5-year survivors of childhood cancers from five different French oncology centers, whose cancers were diagnosed before 18 years of age between 1948 and 1985. 12
The Childhood Cancer Registry of the Rhône-Alpes Region (ARCERRA) cohort included patients who were residents of the Rhône-Alpes administrative district at the time of diagnosis. These patients were treated between 1987 and 1992 for a cancer that was diagnosed before 15 years of age. 3
Of the 1744 women treated in France, 1385 were still alive in 2005 (Fig. 1 and Table 1).
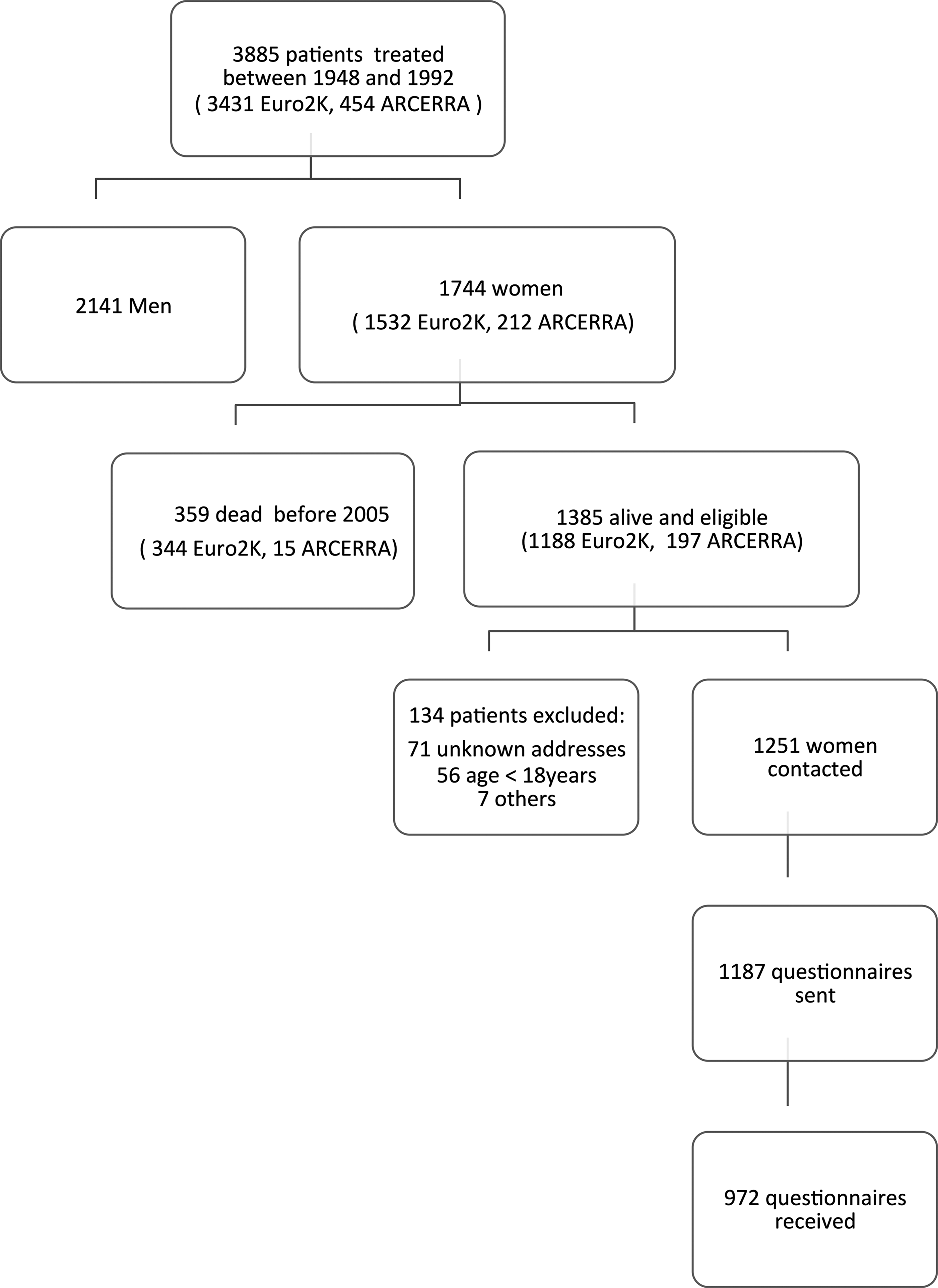
Flowchart of the cohort selection.
NS, not significant.
The vital status of the individuals chosen was verified using the French National Directory for the Identification of Individuals (RNIPP), which has been maintained by the National Institute of Statistics and Economic Studies (INSEE) since 1946. 13 Each patient gave written, informed consent to participate, which was accepted by the French ethics committee.
To be included, it was required that patients be alive and be older than 18 years of age at the time of questionnaire completion (between 2005 and 2010).
Patients with leukemia were excluded and studied in the French childhood cancer survivor study for leukemia cohort. 14
Data Collection
The French Society of Childhood and Adolescent Cancer (SFCE) developed a self-questionnaire based on one that was similar to the Childhood Cancer Survivor Study (CCSS). 6
In this study, responses received between 2005 and 2010, from survivors to questions relating to general situation, QOL, health status, and gynecological history were analyzed. QOL was measured using the MOS SF-36 Health Survey Version 2, the reliability of which was demonstrated for survivors of childhood cancers.15,16 A French version of the survey that was adapted in 1992, for a study concerning inhabitants of Geneva, Switzerland, between the ages of 18 and 44 years, allowed for the definition of standards to develop for young adults.17,18
A letter was sent to former patients requesting their participation, which included an authorization agreement granting permission to contact general practitioners. The SFCE self-questionnaires were sent to the patients who returned their signed agreements. If no answer to our initial correspondence was obtained, a second letter was sent. If there was still no response received, a follow-up phone call was attempted.
Data concerning initial pathology and the treatment that was received at each center were collected from the medical records.
Procedures and Statistical Analysis
The purpose of this study was to analyze fecundity, that is, the ability of an individual to conceive and give birth to a child. From the self-declared questionnaires, women with at least one child were identified, as well as those who had tried unsuccessfully to have a child, and those who did not want or had not decided whether or not they wanted a child.
The fecundity rate is the average number of children born to a given generation of women throughout their reproductive lives, not taking into account the mortality of children who were born. The number of children expected from our study population was estimated by applying the fecundity rates by age in the French reference population, which were published by the INSEE annual census. 13 The estimated expected numbers of children were calculated by multiplying the appropriate number of people at risk by the year of response and the age-specific fecundity rates. Because fecundity rates varied during the period of the survey, we chose fecundity rates for each year of response (2005–2010).
A standardized fecundity ratio (SFR) expressed as the number of actual children observed (O) to the number that would be expected in women of the same age in the general population (E) (SFR = O/E) was calculated for each patient. A chi-squared test was applied to determine if SFR value differed significantly from 1; a p-value <0.05 was considered statistically significant. Poisson exact method was used to calculate the 95% confidence interval (CI) of the ratios. 19
The overall SFR was analyzed in relation to factors such as frequent health problems, initial pathology, and age at questionnaire completion. As usually done in the French literature, we considered the age of 45 years as the upper limit to have a first child. This is why we used this limit of age to study the average number of children in women who had completed their reproductive lives. However, the SFR was compared using the limit of 40 years because data from the French general population were available only by age groups of 10 years (i.e., 30–40 and 40–50 years). Group characteristics were compared using the chi-squared test for the categorical variables, and Student's t-tests for the quantitative variables (α = 0.05).
The following self-reported health problems were selected because they were most frequently described in the population and most likely to be involved in the fecundity process 20 : growth insufficiency, gonadal insufficiency, locomotor, cardiac, vision, hearing, neurological, and psychological disorders (Appendix A1).
For each of the eight dimensions of the SF-36, a linear transformation was used to analyze the scores in a common metric ranging from 0 (worst possible health) to 100 (best possible health).
A multivariate analysis of fecundity was performed and a generalized linear model was used (PROC GLM; SAS, Inc., Cary, NC) to demonstrate the difference between the number of children observed and expected (difference = observed−expected). Self-reported sequelae, which were significantly related to fecundity in univariate analysis, were included in the model with age at questionnaire completion and initial pathology. The variables that were significantly related to fecundity or QOL in the univariate analysis were included in a multivariate model-type multiple regression to examine the relationship between QOL and fecundity.
Results
Population characteristics
Of the 1385 women who were initially identified as eligible for the study, 78 were lost during follow-up (71 unknown addresses and 7 for other reasons) and 56 were excluded (under 18 years of age at the time of the study). The questionnaire was sent to 1187 eligible women, and 972 (82%) returned it (Fig. 1). During the course of the study, 41 women died. The initial pathologies of the 972 women included kidney tumors (24.7%), sympathetic nervous system tumors (16.5%), lymphomas (13.6%), cerebral tumors (8.9%), bone tumors (6.8%), germ cell tumors (6.7%), soft tissue sarcomas (6%), and retinoblastomas (3.9%). The median age of diagnosis was 5 years (range: 0–17). There were significantly more renal tumors observed in responders, and more brain tumors observed in nonresponders (p < 10−3) (Table 1). The median follow-up was 29.1 years (range: 13.9–55.6), and the median age at the time of questionnaire completion was 35 years (range: 18–65).
According to medical records, treatment that patients received for their childhood cancers included particularly sterilizing doses of chemotherapy (9 cases), surgery that prevented reproduction (hysterectomy; 9 cases), abdominal radiotherapy, or craniospinal irradiation leading to ovarian and uterine issues, which caused difficulties for both ovulation (10 cases) and implantation (20 cases).
Fecundity
General fecundity
Of the 972 study subjects, 53% of women (n = 512) had at least 1 child, 50% (n = 486) had at least 1 biological child, and 3% (n = 26) had an adopted child or adopted children only. Furthermore, 38% of subjects (n = 368) did not want or had not decided whether or not they wanted to have a child, whereas 12% (n = 93) had tried unsuccessfully to have a child. A total of 41 children were born with fertility assistance among the 929 children. Among women older than 45 years, who had completed their reproductive lives, the average number of children was 1.4.
At the time of questionnaire completion, 58% of women lived with a partner. Less than 1% of subjects reported that they would have preferred to have fewer children, and 27% preferred to have more. Of the subjects, 25% of them had the number of children desired. Of the 972 women, 83 were seeking to have or adopt a child. Thirteen patients underwent a hysterectomy, or removal of both ovaries, before the age of 21 years, which prevented them from having a biological child.
Table 2 summarizes the frequency of health problems reported in the self-questionnaire. Women with growth (p < 0.001) and gonadal insufficiency (p < 0.001), as well as those with locomotor late effects (p < 0.005) or psychological disorders (p < 0.001), had significantly fewer biological children than the others (Table 2).
Univariate analysis according to presence or absence of each late effect
Compared to other French women in the same general population, age group, and time period, the SFR was 0.65 (95% CI, 0.61–0.69) (Table 3). This ranged from 0.60 to 0.70, depending on the age of the subject at the time of completion. The lowest values were observed from women younger than 40 years who were still in their reproductive years.
In comparison with the entire cohort.
Observed, number of children observed in female childhood cancer survivors; expected, number of children that would be expected in women of the same age in the general population; CI, confidence interval; CNS, central nervous system; SFR, standardized fecundity ratio; SNS, sympathetic nervous system.
The frequency of women who had at least one child varied significantly according to initial pathology. Decreased fecundity was significantly highest among survivors of cerebral tumors (SFR = 0.24; p < 10−3), followed by germ cell tumors (SFR = 0.46; p = 0.003); the highest fecundity was observed in survivors of sympathetic nervous system tumors (SFR =0.79; p = 0.02) (Table 3). As expected, patients with gonadal insufficiency had significantly less children than the general population (SFR = 0.09; p < 10−3), as did patients with growth insufficiency (SFR = 0.4; p < 10−3), locomotor late effects (SFR = 0.54; p = 0.04), and/or psychological disorders (SFR = 0.58; p = 0.02) (Table 3).
After adjustment for age, growth insufficiency, gonadal insufficiency, and locomotor and psychological disorders, the SFR was lower in survivors of germ cell (p = 0.009) and cerebral tumors (p = 0.005), and higher in survivors of sympathetic nervous system tumors (p = 0.03) compared with other tumors (Table 4).
SE, standard error.
Impaired fecundity
Of the 93 women who tried unsuccessfully to have a child, 31 stopped attempting pregnancy without having had children, 10 had a change in their marital situation, 20 experienced a spontaneous miscarriage, 2 had ectopic pregnancies, and 30 unsuccessfully attempted other methods of conception such as the donation of oocytes, or because they had learned their sterility was due to early menopause. One woman stopped trying to have a child when she discovered she had breast cancer.
Medical assistance
Only 25% of the women studied had discussed the issue of fertility with their doctors. Nearly 10% (n = 100) consulted because of difficulties with child conception. In 93 of these cases, additional tests were required to determine the couple's capacity to have a child.
Sixty-four women received treatments to become pregnant: clomiphene citrate (48 women), artificial insemination (13 women; 2 with donor sperm and 11 with partner sperm), and in vitro fertilization (IVF) (23 women). Several women received more than one treatment. Twenty five of the 64 women (40%) were able to have a biological child.
QOL score
QOL score for all women and according to age
The average SF-36 value was 69.2 ± 16.9 (range: 4.9–95.8). The average motor score was 72.5 ± 19.5 (range: 4–100), and the average mental score was 61.4 ± 16.7 (range: 5.3–94.7). The overall SF-36 value decreased with age at the time of questionnaire completion, from 70.7 in women younger than 45 years to 62.0 in those older than 45.
Compared to women of the general population, a significantly lower score was found in each of the eight dimensions of the SF-36 (Fig. 2).

QOL scores of the CCS cohort and the general population in each of the eight dimensions of the SF-36 questionnaire. CCS, childhood cancer survivor; QOL, quality of life.
QOL according to fecundity and risk factors
The SF-36 value increased with increasing SFR (Table 4), even after adjustment for age at the time of completion, the type of cancer, and self-reported iatrogenic events, and for both motor (p = 0.0002) and mental (p = 0.002) scores. In contrast, multivariate analysis demonstrated lower SF-36 values in older women (p < 0.0001) and those having declared locomotor late effects (p < 0.0001), growth insufficiency (p = 0.002), or psychological disorders (p < 0.0001) (Table 5).
Discussion
The response rate to the questionnaire (82%) was satisfactory. We observed a response from a significant number of kidney tumor survivors, whereas survivors of cerebral tumors responded less frequently, as noted in other studies. 20 Survivors of cerebral tumors might have intellectual difficulties for filling out the questionnaire.
Fecundity
In our cohort, the SFR was 0.65 and ranged from 0.24 in survivors of cerebral cancers to 0.79 in survivors of Sympathetic Nervous System tumors, which increased with an increasing SF-36 score. The overall SFR rate was lower than the rates estimated in most other published CCS cohort studies.9,21 Nevertheless, in the CCSS population, the relative likelihood (risk) of ever becoming pregnant was 0.81 among survivors compared with their sibling cohort. 9
We suppose that some causes of decreased fecundity in our cohort were related to the treatments that patients received for their childhood cancers (sterilizing doses of chemotherapy, hysterectomy, abdominal radiotherapy, or craniospinal irradiation). Based on the results of a German study, 21 in which 77% of women participating between the ages of 19 and 37 desired to have a child compared to 90% in their general population, other possible explanations for decreased fecundity in the subjects may include fear of their children developing cancer or their own cancer recurring during pregnancy. Indeed, in our study, survivors of retinoblastomas had one of the lower SFR values, which we suppose was associated with an awareness of the heritability of that particular cancer. Other explanations could be male factors, young age of the woman or her partner, and inability to conceive.
Only 25% of women discussed the issue of fertility with their doctors. Among these, some received treatments that did not impact fertility. The number of women who may not have discussed these issues due to fear, however, is unclear. It may suggest that not all had the same understanding of the question, “Did a doctor speak with you about fertility after treating your illness?” The questionnaire contained free response questions, which led to difficult and subjective interpretation of the answers given. Such questions may be interpreted in different ways and should be modified in the future for better clarity. Women who indicated that they did not want children were not asked for their reasons.
The responses that indicated a lack of exchange between the subjects and their doctors regarding fertility after treatments suggested that oncologists did not adequately inform their young patients about the risk of impaired fertility. Similarly, in Zebrack's study, 22 59% of survivors reported uncertainty about their fertility status; and only 50% recalled a parent or healthcare provider ever mentioning potential reproductive problems associated with their past cancer treatment. Only 41% of women who saw a doctor because they could not get pregnant finally had a biological child.
These findings demonstrated the importance of providing childhood cancer patients with clear and accurate information and the importance of repeating this information throughout their monitoring. In addition, women from the Rhône-Alpes cohort were young and most of whom were still in their reproductive years. Therefore, this study may have underestimated the total number of children conceived. In contrast, differences in therapeutic protocols for patients included in the Euro2K cohort, who were diagnosed between 1948 and 1985, from current treatments, may have affected fertility outcomes. Methods of assisted reproductive technology (ART) were not as well developed as they are at present and allowed only some women to give birth. Some women have benefited from IVF or ovarian stimulation, and ART has aided the births of 41 children. Indeed, we have methods to offer patients with cancer today, which can preserve their fertility, including ovarian preservation or transposition.23–25
Fecundity, QOL, and risk factors
Compared to the general population, the scores of the QOL of the women of this cohort of CCS were significantly decreased in each of the eight dimensions of the SF-36. 17 Zebrack's team found similar results: evidence that children and young adults monitored for cancer during childhood in the United States had difficulties in their social lives and relationships, and felt more psychologically fragile. 22 Overall, the QOL score was correlated to and proportional with the intensity of subfertility.
Scores of mental QOL did not differ significantly between women with or without children or among the different subgroups of women studied. Nevertheless, not having children affected the scores of global and motor QOL of women in this study, as the QOL score was proportional to the SFR. It is also possible that women with serious sequelae did not want to have children. In addition, QOL did not differ significantly between women who had biological children and those who adopted.
In a Dutch cohort, as well as in studies of the general population, QOL was reported to be significantly lower in infertile women than in women with children. 26 However, it is difficult to compare populations with different cultures. In some countries, giving birth is one of the most important roles of a woman. 27 The lack of differences may be explained by the small number of women who failed to conceive; however, it may also be considered that these young women may have thrived because of their awareness of post-cancer treatment difficulties associated with having a child after their treatment and developed other priorities. It would be interesting to learn about their psychological, social, and professional profiles.
Conclusions
Overall, adult female survivors of childhood cancer demonstrate decreased fecundity that impacts their QOL. Efforts should be made to avoid the risk of future infertility when considering therapeutic strategies in pediatric patients with cancer.
Footnotes
Acknowledgment
The research support for the study
Ethical Standard
Research involving human participants and/or animals: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Author Disclosure Statement
No competing financial interests exist.