
Abstract
Adolescents and young adults (AYAs) 15–39 years old face unique challenges during cancer treatment as developmental and social needs are often disrupted to achieve cure. Developmentally appropriate supportive care for AYAs across the cancer trajectory is needed. The purpose of this review is to identify and describe instruments that measure AYA development across physical, psychological, and social domains, commenting on the instruments' psychometric properties and usefulness in clinical practice and research. A computerized literature search published in English from 1950 to January of 2017 was conducted utilizing the following databases: Mental Measurements Yearbook (MMY), Health and Psychosocial Instruments, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, and Google Scholar. The following instruments were identified and described: the Child Health and Illness Profile–Adolescent Edition (CHIP-AE); the Course of Life Questionnaire; the Developmental Task Questionnaire (DTQ); the Impact of Cancer scale for childhood survivors and AYAs (IOC-CS and IOC-AYA); the McCleery Scale of Adolescent Development (MSAD); and the Minneapolis-Manchester Quality of Life Adolescent and Young Adult Form (MMQL-AF and MMQL-YA). Among currently available instruments, the IOC-AYA and MMQL-AF were relevant to AYAs undergoing or completing cancer therapy. However, validation for the IOC-AYA occurred in cancer survivors off treatment so further psychometric evaluation is needed in AYAs currently undergoing cancer treatment. Furthermore, the MMQL-AF has been validated for use during active cancer treatment, but is limited to adolescents 13–20 years. Further research may be needed to create or refine instruments measuring the developmental impact in AYAs, particularly emerging adults undergoing active cancer treatment.
Introduction
D
Implementing and testing developmentally appropriate interventions presume that outcomes or behaviors targeted for change are relevant for AYA populations. An evidence base that accurately reflects appropriate psychosocial and developmental outcomes for this population is nascent and relies predominantly on standardized measures developed for and administered to older adults 18 without any evidence to support the measures' reliability and validity when applied to AYAs. For example, the Brief Symptom Inventory (BSI-18) is a commonly used instrument for detecting psychological distress in cancer patients, originally developed for an older adult population. In psychometric analyses of the BSI-18 among AYA survivors of childhood cancer, Recklitis and Rodriguez 19 reported that sensitivity and specificity were low when using published population-based norms for scoring; the investigators suggested that an alternative and lower threshold score was optimal for detecting clinically significant distress.
A number of instruments measuring quality of life (QOL) exist for cancer populations. However, few instruments assess how cancer and its treatment disrupt normative development and achievement of developmental tasks for AYAs, including (1) autonomy and emotional separation from parents, (2) establishing an identity, (3) developing intimacy through healthy peer attachments and dating, (4) fostering a positive body image, (5) acquiring academic achievement, and (6) making decisions about careers, employment, higher education, and future family.2,20–22 Measures are needed to detect the developmental needs and developmental interruptions that may occur during cancer treatment and into survivorship.
The wide age range of AYAs defined by the National Cancer Institute 23 presents a unique and potentially difficult challenge during cancer treatment, as many developmental changes occur in adolescence through young adulthood. AYAs living with cancer experience these developmental challenges, including acquiring one's identity and forming a peer group during adolescence. The tasks carry over into young adulthood where identity formation continues 24 while mastering intimacy and deepening relationships. Although developmental milestones differ among individuals, a common task is establishing personal identity while building and strengthening intimate relationships. 5
The purpose of this integrative review is to identify and describe instruments that measure constructs specific to AYA development across physical, psychological, and social domains. An adjoining purpose is to evaluate the instruments' psychometric properties and comment on their usefulness in clinical practice and AYA oncology research.
Methods
Integrative review search strategy
This study utilized an integrative review method to critically evaluate literature pertaining to the assessment of AYA developmental milestones.25,26 A computerized literature search published in English from 1950 to January 2017 was conducted by the lead author and two librarians specializing in education, psychology, and health sciences. Our search dated back to 1950 to capture instruments based on the early work of prominent developmental theorists (e.g., Erikson, Havighurst, Kohlberg, Piaget, and Vygotsky). The following databases were used: Mental Measurements Yearbook (MMY), PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Health and Psychosocial Instruments (HaPI), and Google Scholar.
Search terms to locate studies of instruments that measured global development during adolescence and young adulthood included adolescent OR young adult AND development OR physical development OR social development OR psychological development AND chronic disease OR healthy. We specified “instrument construction” on major headings or specified “developmental” OR “adolescent development” as the subject to narrow findings. Medical Subject headings (MeSH terms) included neoplasms/psychology AND interpersonal relations OR family relations AND instrument development. Inclusion criteria were any study design resulting in a quantitative instrument measuring multiple aspects of AYA development.
We sought to identify instruments that could be used pragmatically in research and practice to holistically capture the developmental impact of cancer during this life stage. Each database yielded from 3 to 546 articles depending on the search terms. Abstracts were carefully reviewed by the lead author to determine whether an instrument measured multiple constructs of AYA development, such as: (1) autonomy, (2) identity, (3) intimacy, (4) body image, (5) academic/career achievement, and (6) decisions about the future.
The review method is illustrated in Figure 1. After removing duplicate titles, we applied the following exclusion criteria while reviewing abstracts: instruments measured only one aspect of AYA development (e.g., identity27,28 or sexual development 29 ), development measured through qualitative interviews and/or instruments used to identify defensive mechanisms or high-risk behaviors across developmentally appropriate domains.30–32 The exclusions resulted in a yield of seven instruments. After full-text review, one article was eliminated because the instrument items were written in French and full-scale testing was not done. 33 We searched the reference lists of the remaining six articles, as well as Google Scholar (first author's last name and name of instrument), to identify additional articles pertinent to the instruments of this review. Through this approach we added 16 articles describing aspects of instrument development, testing, or translation into another language resulting in 22 articles for our final review.
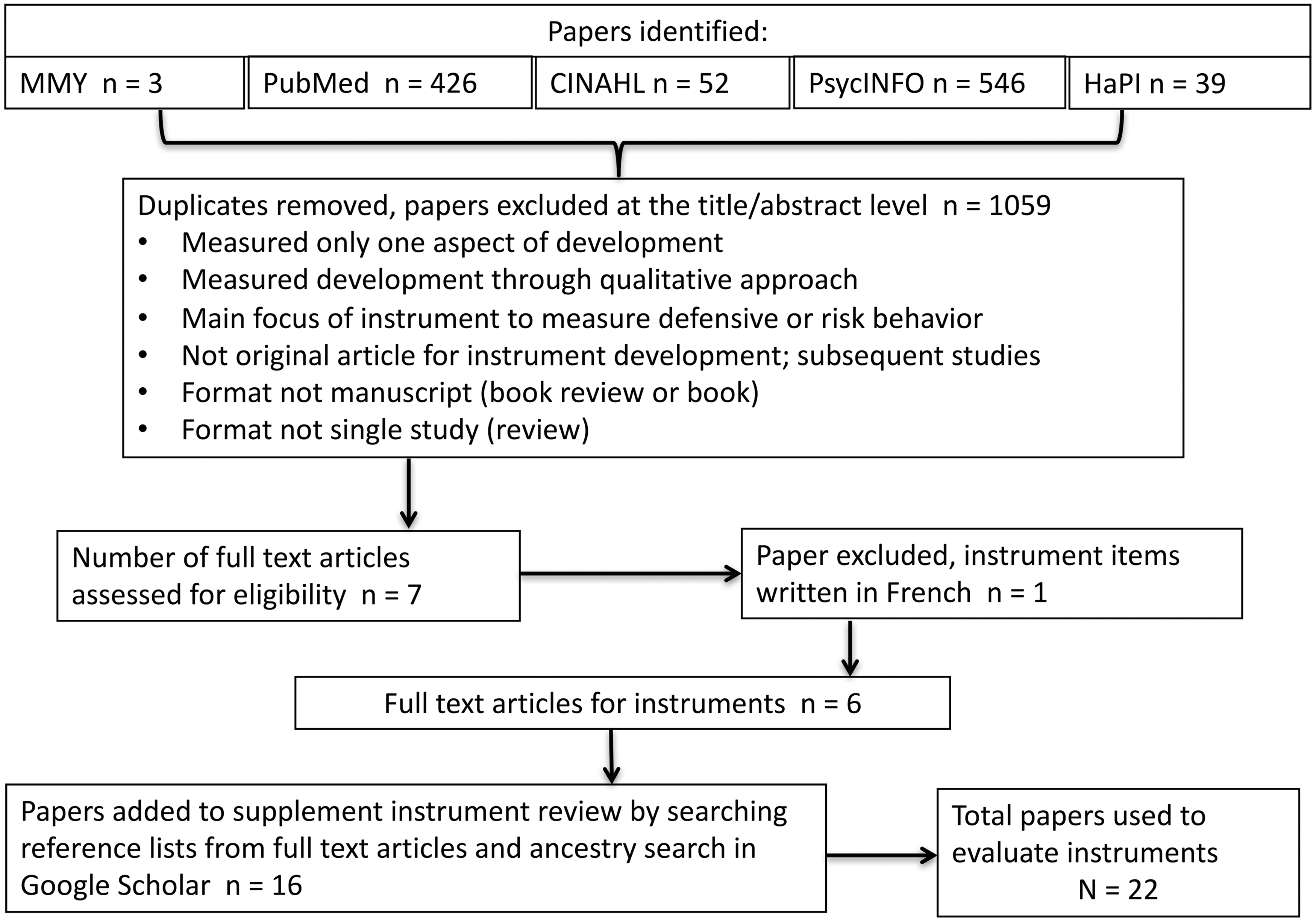
Review method utilizing PRISMA: preferred reporting items for systematic reviews and meta-analyses. CINAHL, Cumulative Index to Nursing and Allied Health Literature; HaPI, Health and Psychosocial Instruments; MMY, Mental Measurements Yearbook.
Assessment of selected instruments
Two authors independently rated each of the six instruments that met our inclusion criteria. The instruments were evaluated utilizing recommendations initiated by the Scientific Advisory Committee of the Medical Outcomes Trust. 34 We assessed key attributes proposed for health status and QOL instruments, 34 including recommendations for cross-cultural adaptation. 35 These stringent quality criteria are further described in Table 1 and include: (1) content validity, (2) internal consistency reliability, (3) construct validity, (4) reproducibility, (5) responsiveness, (6) variability (floor and ceiling effects), (7) interpretability, (8) burden/acceptability, and (9) cross-cultural and language adaptations (translations).34–38
Criteria for evaluating instruments are based on consensus of expert opinion in scale development using the following Ref.34–38
AUC, area under the curve; CFI, comparative fit index; ICC, intraclass correlation coefficient; MIC, minimal important change; RMSEA, root mean square error of approximation.
Results
We identified six instruments measuring AYA development that fit our review criteria, including three instruments with separate AYA versions.39–41 The instruments, developed between 1953 and 2012, fell into two categories: (1) instruments that measured developmental milestones or developmental tasks and (2) instruments that measured physical, psychological, and social aspects of development during adolescence and young adulthood.
An overview of each instrument and the relevant constructs specific to AYA development is provided, with comments on each instrument's usefulness in clinical practice and research. Further descriptions of the six instruments are in Table 2, and a summary of the assessment of quality criteria is provided in Table 3.
This table briefly summarizes descriptions of what each instrument measures and includes the number of items, reliability statistics, and strengths and limitations.
AYA, adolescent and young adult; QOL, quality of life.
This table rates whether or not the reliability, validity, and other quality criteria were met based on the definitions and recommended scoring rubric in Table 1.
+, criteria met; −, criteria not met; U, unknown or not found in literature; N/A, not applicable.
IOC-CS, Impact of Cancer-Childhood Survivors; IOC-AYA, Impact of Cancer-Adolescent and Young Adult; MMQL-YA, Minneapolis-Manchester Quality of Life-Young Adult Form.
Instruments measuring developmental milestones or developmental tasks
The Course of Life Questionnaire (CoLQ), 42 Developmental Task Questionnaire (DTQ), 40 and McCleery Scale of Adolescent Development (MSAD) 43 are three examples of instruments that measure developmental tasks or milestones. The CoLQ was developed for use within oncology, whereas the DTQ and MSAD were developed to assess developmental tasks in general AYA populations. CoLQ and DTQ were originally developed in Europe and their English versions have not been validated in U.S. populations.
Course of Life Questionnaire
The CoLQ was originally developed for use in Dutch populations to retrospectively gather information about achieving developmental milestones and assessing developmental gaps after the diagnosis and treatment of cancer. 42 Item development was based on literature, clinical expertise, and input from an academic medical center's psychosocial department. Factor analysis was not applied to determine dimensionality. Rather, Pearson correlations were used to examine each subscale indicating r < 0.30 on all subscales except Antisocial Behavior and Substance Use and Gambling subscales, which were correlated at r = 0.49. Stam et al. 42 deduced that subscales measured distinct constructs. Furthermore, the internal consistency reliability was low (α = 0.46–0.49) on some of the subscales.
Two of the articles referencing psychometrics of the CoLQ were only available in Dutch, affecting our ability to fairly evaluate the instrument. For example, for reproducibility the test-retest reliability is reported as “good” with reference cited in a Dutch publication. The time frame for the repeated measure and statistic (e.g., intraclass correlation coefficient [ICC] or weighted Kappa) was not reported in English. Responsiveness and floor or ceiling effects were not described. However, the scale was dichotomized to a yes/no response, indicating that the developmental milestone was either achieved or not achieved for most items. The way the scale was developed clearly affected evidence of scale variability.
The CoLQ was initially tested in AYAs with a history of cancer (n = 353) and peer controls (n = 508) with means and standard deviations provided. 42 After initial testing it was used in other AYAs with a history of chronic illnesses (N = 650). 44 The CoLQ was translated into German and tested in a population of 820 AYA cancer survivors and 1027 young adults with no history of cancer. 45 The Psychosexual subscale was the only subscale with sufficient internal consistency (Cronbach's α = 0.74) and, therefore, the only subscale retained in the German study. 45 The CoLQ is available in English, but it has not been validated in a U.S. population. Details on how the instrument was translated into other languages were not provided in the literature. No information was found on respondent burden.
CoLQ usefulness in clinical practice and research
Because the CoLQ was validated and tested in a Dutch population, it has limited usefulness in English-speaking clinical practices until it is tested in an adequate English-speaking population to determine reliability. Once this step is taken, the CoLQ may be helpful for use in survivorship clinics and/or survivorship research studies as much of the instrument measures achievement of developmental tasks or developmental milestones across the growing-up years and into adulthood. The questionnaire detects failure to achieve developmental task/milestones once an individual has reached adulthood. Its usefulness in clinical practice is limited during cancer treatment for adolescent patients because many questions focus on life after high school. Furthermore, there may be response bias, as the questionnaire probes for information the participant must recall starting from elementary school. Several responses are yes/no, limiting the ability to measure increments of change across time.
Developmental Task Questionnaire and McCleery Scale of Adolescent Development
The DTQ40,46 and MSAD 43 measure AYA developmental tasks. Both instruments are based on Havighurst's Theory of Developmental Task Attainment, 21 which suggests that individuals must achieve key developmental tasks at critical periods in life based on biological and psychological development, as well as social and cultural norms. The theory suggests that attainment of developmental tasks leads to personal satisfaction and confidence to move toward the next set of tasks in life, and failure to attain developmental tasks creates internal turmoil and hinders developmental progression. 21 For both instruments, perceived importance of key developmental tasks that occur during adolescence or young adulthood is subjectively assessed on a three-point scale (not important, somewhat, or very important). However, the DTQ also assesses AYA perceived attainment of key developmental tasks using a three-point scale (not yet, just starting, already developed).
The DTQ is a relatively short unidimensional instrument. The original version was developed in 1984 where 11 developmental tasks were identified as important with a representative sample of 2000 adolescents participating in the Berlin Longitudinal Study on Youth Development. 40 The initial 11 developmental tasks were reduced to 9 for the adolescent (DTQ-A) and 8 for the young adult (DTQ-YA) in subsequent studies.46–48 Details on content validity for the young adult version were absent in English reports and there was no mention of pilot testing the DTQ-YA in a sample of young adults. Furthermore, only 50% of the original version hypotheses were congruent with a priori hypotheses for the DTQ-YA,47,48 so this instrument did not meet our quality criteria for construct validity for the young adult version.
The DTQ yields three scores. Item means are totaled to yield a total score for Current Developmental Status (AYAs' perceived attainment of developmental tasks), a total score for Aspired Status (AYAs' subjective importance of developmental tasks), and a third score for Developmental Pressure (derived by calculating the difference between current developmental status and aspired status). In Seiffge-Krenke's studies,40,46–49 the importance and achievement of developmental tasks vary with age and health status.
The DTQ has been widely used in prospective longitudinal studies (in Germany and Belgium) of healthy AYAs and AYAs with insulin-dependent diabetes.40,46–49 The means, standard deviations, and progressive change in developmental scores were reported across time.40,46–48 In studies comparing AYAs diagnosed with insulin-dependent diabetes versus healthy controls, both groups had similar aspired status.40,49 However, significant differences in the actual attainment of developmental tasks were found, with diabetic adolescents scoring lower on tasks involving physical maturity and increasing autonomy from parents. 40
References were provided for the psychometrics of the original DTQ instrument development; however, some reports were nonpublished theses or studies referenced in German, 40 leaving several evaluative criteria unknown (e.g., reproducibility, responsiveness, and floor and ceiling effects). The DTQ is available in English and German, but evidence of cross-cultural adaptation or respondent burden was not described in the English literature.
DTQ-A and DTQ-YA usefulness in clinical practice and research
Before use in U.S. clinical practices, further cognitive interviews (face validity) with English-speaking AYAs would be beneficial to test clarity of item wording, particularly for the items, “establishment of an autonomous identity” and “achievement of sociopolitical awareness” and items tapping into the importance and attainment of developmental tasks for emerging adults. Finally, confirmatory factor analysis to verify the unidimensionality of the scale would be useful since this was not done on the original instrument.
The MSAD measures the importance of adolescent developmental tasks 43 and consists of 150 items. However, details were not provided on item selection or use of experts and target population during pilot testing. 43 Furthermore, the instrument was only administered to adolescent males, and factor analysis was not used to determine dimensionality, so it is uncertain how the 10 subscales were determined. This instrument was developed in the United States almost 60 years ago when Cronbach's alpha was just starting to emerge as an extension of the split-half coefficient of Kuder and Richardson. 50 Therefore, we assessed reliability based on a split-half reliability coefficient for the total scale and 10 subscales. The Spearman–Brown formula was used to predict reliability. 43
The MSAD item wording may not be appropriate for today's youth. For example, terms such as going steady, being liked by my neighbor, or knowing how to act when out in company might not resonate with today's youth. The author claims that other studies utilizing the instrument were conducted in New Jersey, Ohio, and Nebraska; however, we were unable to find additional publications using this scale in the literature.
MSAD usefulness in clinical practice and research
The instrument has not been tested in female populations. Caution is encouraged before using the MSAD in clinical practice or research.
Instruments measuring physical, psychological, and social AYA development
Three instruments capture aspects of development across physical, psychological, or social domains. Two have been specifically developed for use in cancer populations: the IOC Scale 41 and the Minneapolis-Manchester Quality of Life (MMQL) Instrument. 39 The Child Health and Illness Profile–Adolescent Edition (CHIP-AE) 51 has been widely used in both chronic disease and healthy populations of adolescents who are 11–17 years old.51–54 In addition, all three instruments measure aspects of health functioning and well-being.
Child Health and Illness Profile–Adolescent Edition
The CHIP-AE measures participation in developmentally appropriate tasks and activities in addition to aspects of health and well-being, including behaviors that promote and threaten health. 51 In recent studies, the CHIP-AE has been used to compare risk activities in adolescent survivors of childhood cancer.55,56 This instrument was solidly developed with input from adolescents, parents, and pediatric professionals, and evidence of construct validity was clearly established. 54
Items that capture development describe (1) educational outcomes and school performance, (2) work performance, (3) self-acceptance, (4) age of first sexual intercourse, ongoing sexual activity, and (5) social interactions with family and friends. In addition, developmentally relevant adolescent risk behaviors (e.g., smoking, drinking alcohol, using illegal drugs, or acquiring sexually transmitted diseases) are measured.
Reliability and validity testing were conducted in a large sample (N = 3451) of rural and urban youth 51 with solid content and construct validity noted.51,54 However, the internal consistency reliability of five of the subdomain scales had Cronbach's alpha below 0.70, and the stability of the instrument 1 week later reported ICCs of <0.70 on all three of the Discomfort subdomains (physical, emotional, and limitations of activity) and one of the Resilience subdomains (problem solving). 51
This instrument does not allow for a total score. Instead, factor analysis is completed within domains to determine subdomains. Measurement and interpretation are most accurate at the subdomain level. 51 We did not find reports describing floor and ceiling effects. Studies using the CHIP-AE were cross-sectional, lacking data on responsiveness to change across time. The CHIP-AE is a lengthy measure and was the only instrument to report respondent burden (∼30 minutes). It met the quality criteria of forward and backward translation and cross-cultural adaptation of a Spanish version for use in Spain, 57 but warrants further testing for use in other Spanish-speaking populations.
The CHIP-AE usefulness in clinical practice and research
The CHIP-AE is used widely in educational and research settings and demonstrates potential usefulness in clinical practice for oncology patients under the age of 18. The CHIP-AE is a lengthy scale of 107 items. However, clinicians could pick and choose the domain and/or subdomains of interest to screen adolescent satisfaction with health and self-esteem, emotional or physical discomfort, academic achievement, or resilience, including family involvement. The instrument does not need to be used in its entirety since each domain acts as a separate scale.
Impact of Cancer scale
The IOC scale has two versions, one for AYAs who were diagnosed with cancer during childhood (IOC-CS) 41 and one for AYA survivor (IOC-AYA) 58 who had cancer between the ages of 15 and 29. Psychometric analyses were recently published on the IOC-AYA and are included in this review. 58 The IOC measures subjective experiences across developmentally relevant QOL aspects of cancer survivorship. Items are rated on a five-point Likert scale from not at all to very much for the IOC-CS and from strongly disagree to strongly agree for the IOC-AYA. The original scale was generated from qualitative interviews with 64 U.S. cancer survivors. 59
Impact of cancer–childhood survivors
Items for the IOC-CS were evaluated to establish content validity by oncology clinical and research experts and AYA cancer survivors to determine the final item content. 59 Psychometric evaluation occurred in 519 cancer survivors from three U.S. hospitals with means and standard deviations provided. 41 Factor analysis was used to determine dimensionality and subsequent item reduction. Subscales were evaluated for convergent and discriminant construct validity with established instruments that measure QOL, stress, and symptom burden with expected associations observed.
Significant differences in IOC-CS subscales across relationship status, cancer type, and overall health criteria were consistent with reports from the literature. 41 IOC-CS subscales were more highly correlated with measures of psychological well-being, mental health functioning, and distress than with the Physical Component Score of the Short Form-36 (SF-36). This suggests that the IOC-CS subscales tap into the psychological and subjective experiences of how cancer continues to impact survivorship in both positive and negative ways. 41 Previously unreported aspects of long-term QOL survivorship were evident in the Health Literacy and Personal Growth subscales, which were not related to any of the other established QOL instruments used for construct validity. 41
Floor and ceiling effects were not reported on individual items. However, 51% of the respondents reported floor effects for the Financial Problems subscale, and 20.8% and 33.9% reported ceiling effects for the Socializing and Talking with Parents subscales, respectively. 41 These figures exceeded the 15% threshold for floor and ceiling effects described in our evaluation criteria.
Impact of cancer–adolescent and young adult
Items from the final IOC-CS scale were evaluated for relevance by researchers, clinicians, AYA advocates, and AYA survivors. Some items were deleted, and additional items were suggested to generate a comprehensive list of 91 relevant and acceptable items for the IOC-AYA. Psychometric evaluation occurred in 173 survivors of AYA cancer (Hodgkin and non-Hodgkin lymphoma, leukemia, testicular cancer, soft tissue sarcoma, and bone tumors) with means and standard deviations provided. 58 Factor analysis was used to determine dimensionality and subsequent item reduction for 65 items answered by all participants. Two additional subcategories containing 26 items related to “relationships and dating” and “having children” were not answered by everyone and therefore excluded from factor analysis.
Construct validity was evaluated with established instruments yielding expected associations. Multitrait scaling confirmed the scale structure of the IOC-AYA. 58 The final instrument contains 31 items across 7 developmentally relevant domains.
IOC-CS items that capture development include concerns about (1) physical appearance; (2) relationships with friends, family, and intimate partner; (3) sexual intimacy; (4) cognition; and (5) future goals in life. The IOC-AYA contains developmentally relevant items related to (1) social life, (2) relationships and family planning, (3) purpose and life goals, and (4) identity.
The IOC-CS and IOC-AYA usefulness in clinical practice and research
Both IOC scale versions are relevant for AYAs in survivorship clinics who were diagnosed with childhood or AYA cancer. Several items are written as “having had cancer” in the past. Before the instrument is used in clinical practice for AYAs currently undergoing cancer treatment, the items would need to be modified to the present tense with psychometric evaluation completed within research studies before clinical use. Furthermore, testing the IOC-AYA to confirm factor structure in a larger sample representing all cancer types would be beneficial.
Minneapolis-Manchester Quality of Life Instrument
While developing the MMQL, 39 the authors took into consideration the differing developmental stages of the child, adolescent, and young adult. They created three versions of the instrument: the MMQL-Youth Form for children 8–12 years of age, the MMQL-Adolescent Form (MMQL-AF) for adolescents 13–20 years of age, and the MMQL-Young Adult Form (MMQL-YA) for adults aged 21–45 years. Psychometric analyses have not been published on the MMQL-YA and therefore appear as unknown in Table 3. Information related to the Adolescent Form is reported in this section.
The MMQL-AF is a standardized self-report patient measure that assesses developmental aspects of QOL. Items that capture development include (1) difficulties with school work, (2) feelings about body development, and (3) interactions with friends, including intimate relationships. 39 Item development was based on the input of adolescent cancer survivors, their parents, and clinicians. 39 It was further refined during adolescent interviews and then tested in two groups of adolescent cancer survivors. Factor analysis was applied to determine dimensionality, resulting in seven subscales with Cronbach's alphas ≥0.80 on all subscales except Intimate Relations (α = 0.67). 39 Because all items could be summed for a total scale score, we used the total scale Cronbach's alpha of 0.78 to evaluate internal consistency reliability.
Psychometric evaluation occurred in a sample of 397 adolescents (n = 129 adolescents without cancer, n = 110 adolescents currently undergoing cancer therapy, and n = 158 adolescents off cancer therapy for at least 1 year). 37 MMQL-AF reliability and validity were initially established in adolescents treated for cancer across nine institutions in the United States. 39 Additional discriminate validity was established in a larger sample of 362 adolescent cancer survivors across 20 Children's Oncology Group institutions and 134 healthy controls. 60 Means and standard deviations were provided in the first study for three subgroups of more than 50 people. 39 In the second study, means and standard deviations were provided across three groups and differentiated by sex, diagnosis, age group, and race. 60
The stability of the MMQL (test-retest reliability) was tested after a 2-week interval. The ICC was 0.71 for the total scale. The instrument was tested in cross-sectional studies. Therefore, longitudinal responsiveness is unknown. Floor/ceiling effects and respondent burden were not reported. The MMQL-AF is available in English and has been cross-culturally adapted for use in Japanese, Korean, and Swedish populations.61–63 Psychometric analysis is strong across diverse cultures of adolescents with the ability to distinguish on-treatment cancer patients and off-treatment cancer survivors.39,60–63
MMQL-AF usefulness in clinical practice and research
The MMQL-AF shows great promise for use in diverse adolescent cancer populations. The instrument has been widely tested and may be useful in clinical practice and research settings for adolescents 13–20 years old. Further psychometric evaluation of the young adult form is needed in research studies so that clinicians may benefit from a tool for their young adult population.
Discussion
This integrative review has revealed a very limited number of well-validated instruments applicable to the U.S. AYA patient population, indicating need for further validation or development of new instruments. In addition, as developmental norms change over time, updates are crucial to make existing instruments more suitable to current and upcoming AYA generations. Most instruments, except the DTQ, were used in cross-sectional studies. Measuring longitudinal development across the trajectory of cancer treatment and survivorship may be particularly useful in identifying needs and improving care for AYAs living with cancer. AYA development occurs across time within the context of social interactions.
All instruments identified in this review included items measuring aspects of AYA development across physical, psychological, and social domains. However, instruments varied in how development was assessed. Some instruments measured developmental tasks/milestones resulting from physical, psychological, and social growth and development. Other instruments measured developmentally relevant features across physical, psychological, and social QOL domains. It is noteworthy to recognize that QOL instruments are not always tailored to detect aspects of AYA development. Therefore, both clinicians and researchers must be acutely aware of normal AYA development and look for representation of developmental domains when selecting appropriate instruments for this age group.
Among currently available instruments, the IOC-AYA and the MMQL-AF are the most appropriate for use in AYAs who are undergoing or have completed cancer therapy. Both instruments detect the influence of cancer on developmental domains. However, the IOC-AYA has only been used in cancer survivors who are off treatment, and the MMQL-AF is limited to adolescents. The DTQ-A is another useful tool for determining developmental tasks that have not been achieved but remain important to adolescents undergoing or completing cancer treatment. This instrument has not been used in cancer populations on or off therapy. Furthermore, the distinct developmental differences during the stage of emerging adulthood (18–25 years old) have not been adequately captured by the DTQ-YA. Research may be needed to create or refine an instrument specifically measuring unique developmental tasks/milestones of the emerging adult.
Limitations
Our literature review was limited by our search terms and subsequent literature retrieved on instruments used to holistically measure multiple aspects of AYA development. Search terms and subsequent instruments measuring specific developmental constructs (e.g., identity) were not included in this review. We used stringent criteria for evaluating the selected instruments, recommended by experts in the field of instrument development.34,35,36 Some studies did not report all of the specifications we used to assess the performance of each instrument and therefore some quality criteria were unknown. The ratings in Table 3 were dependent upon information available in the literature in English and the quality of reporting information. Consequently, our assessment was likely to be biased. Moreover, developmental norms may be culture specific, thus cross-cultural adaptation may not necessarily be adequate or possible.
Conclusion
The only instrument validated for use during active cancer treatment is the MMQL-AF. Longitudinal research is needed with appropriate developmental instruments to detect responsiveness to change across time and to identify the developmental interruptions that may occur during cancer treatment in AYA populations. Accurate assessment of unmet developmental needs is necessary for forming strategies and interventions to support AYAs, a unique understudied cancer population, along the trajectory of cancer and into long-term survivorship or to end of life.
Footnotes
Acknowledgment
The authors thank Beth Langelier for her excellent editorial assistance with the preparation of this article.
Author Disclosure Statement
No competing financial interests exist. No animal or human studies were carried out by the authors for this article.