
Abstract
Communication plays an essential role in social relationships. Yet it is unclear how young cancer patients and survivors communicate with peers, and whether this contributes to increased rates of social difficulties. We aimed to analyze how childhood cancer patients and survivors communicate about their cancer with family and peers. We systematically searched Medline, Embase and PsycINFO for peer-reviewed studies on cancer-related communication among patients and survivors (any cancer, <25 years at diagnosis). We screened 309 articles, and included 6 qualitative studies. Studies were assessed using a standardized quality assessment tool. Participants were adolescents and young adults, 16–34 years of age at the time of study. Included studies related to different forms of cancer-related communication, benefits, and challenges. We found that cancer-related communication was an individual, complex process, addressing medical, existential, and emotional aspects of cancer. Communication occurred on a spectrum with variation in who information was shared with, as well as differences in the frequency at which information was shared, and the amount and type of information shared. Communication often occurred at uncertain or significant times for participants, or was initiated by others. Communicating about cancer yielded benefits as a coping strategy, prompted social support, and appeared central to significant relationships. Barriers to communication, including fear of stigma and poor peer reactions, hindered willingness to disclose. The number of studies analyzing this topic was limited. Communicating about cancer is a significant yet complex process for young patients and survivors. Further research is needed to complement the existing literature and to establish the evidence base for the development of future effective interventions promoting social and communication skills.
Introduction
C
Childhood and adolescence are times of transformation and development, when identity formation along with social network establishment is critical for transitioning into adulthood. 15 Many survivors demonstrate good psychosocial functioning, showing resilience and positive growth as a result of their cancer 16 ; these survivors tend to do well socially, develop closer relationships, and show increased maturity, suggestive of posttraumatic growth. 17
However, recent studies also highlight how childhood cancer can negatively impact social outcomes for some survivors.18,19 Young cancer patients have very high rates of school absenteeism, twice the rates of other chronic illnesses, and are likely to experience disruption of tertiary education and employment.8,20,21 This may reduce opportunities for social interactions and development of social skills. 22 While early school reintegration is protective, it can be complicated by social difficulties. 1 Between 25% and 34% of survivors experience social difficulties upon school re-entry.23,24
Research on young survivors has shown increased rates of isolation, bullying, and difficulties relating to peers.8,25 Some adolescents and young adults (AYAs) also experience cancer-related discrimination in the workplace, such as being refused jobs.8,26 Moreover, these social difficulties can affect survivors in the long term, all the way into adulthood. Systematic reviews examining social outcomes among young cancer patients and survivors show higher rates of social isolation, concerns about sexual intimacy and romantic relationships, strain on family relationships and higher rates of separation, illness-related employment difficulties and unemployment, as well as financial concerns and dependency.1,8,18
Psychosocial support is essential in maintaining long-term quality of life,21,27,28 and may predict lower psychosocial distress in young cancer patients. 1 Peer support in particular has been related to successful adaptation to cancer. 29 However, young patients and survivors can feel peer support is lacking,21,30 often at a stage in life when peer relationships are integral to development. 16
Self-disclosure and communication are essential for the establishment and nurturing of significant relationships and intimacy. 31 These skills promote social support,32,33 as well as the development of personal identity and self-confidence, 31 which can all be compromised by a cancer diagnosis at a young age. A qualitative study exploring the experiences of adolescents with cancer found that participants benefited from discussing cancer-related issues with others who had shared similar circumstances and understood them. 16 However, many studies have shown that this is not the case with healthy peers, as young patients and survivors often report lack of understanding from healthy peers and feel “left behind” socially.1,8,16,25–27,34
Maintaining and reintegrating into existing social groups, as well as forming new relationships, is one of the greatest difficulties reported by survivors.8,24,27 These findings suggest the importance of promoting communication about cancer. A cross-sectional survey study in adult survivors showed that cancer-related communication within the family setting was linked to improved mental health and well-being, and that avoiding discussion about cancer had negative consequences on the family.35–37 Therefore, equipping patients and survivors with strong social and communication skills to talk about their cancer may foster acceptance and integration; the foundations of socialization. 38
Appreciating how this unique population communicates about cancer with the major players in their life is critical for the development of evidence-based interventions to support survivors' healthy adaptation to their cancer experience. Indeed, over 25% of survivors have reported a need for more information regarding talking about cancer with their friends 39 ; yet the literature regarding cancer-related communication is, to date, mainly restricted to practitioner–patient and family communication, and largely focused on adult cancer patients and survivors.
The aim of this study was therefore to systematically review the literature surrounding cancer-related communication among childhood cancer patients and survivors with family, friends, and school staff. In synthesizing this literature, we aimed to provide guidance and direction for future research and intervention development. Our research questions were:
(1) How do childhood cancer patients and survivors communicate about their cancer: specifically, about what, when, to whom, and why do childhood cancer patients and survivors choose to disclose their cancer? (2) What benefits and difficulties are experienced when childhood cancer patients and survivors communicate about their cancer?
Methods
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, 40 including the development of clear eligibility criteria, and description of information sources and search strategy. We have also reported on the process of study selection, data collection, and identification of study bias in accordance with these guidelines.
Eligibility criteria
Our review concentrated on studies examining cancer-related communication between AYA cancer patients/survivors and their family, friends, or school staff. We excluded studies conducted within the healthcare system, for example addressing patient–provider communication. We included all cancer types, with participants diagnosed under 25 years. The age of diagnosis cutoff was set at 25, to align with definitions of AYAs used in Australia and Europe. 41 We acknowledge that other definitions and age ranges for AYAs have been used, and despite the importance of the definition, it remains controversial. A cutoff for age at diagnosis at 25 allowed us to select a more homogeneous population regarding social development and social issues, which may differ significantly for patients under or over 25. 1 For studies where age at diagnosis was not mentioned, we accepted descriptive terms, including “adolescents” and/or “young adults.” We included all study types, but rejected duplicates, conference abstracts, single cases, case reports, dissertations, and book reviews.
Search strategy
We searched Medline, Embase, and PsycINFO in title and keyword fields (Table 1), to ensure a comprehensive search across both medical and psychosocial science journals. Filters included English language and humans. We did not restrict the search to a certain time frame. The search was conducted on February 27, 2017. An additional search was performed by checking the reference lists of eligible articles.
AYA, adolescent and young adult.
Study selection
Our search located 309 studies, excluding duplicates (Fig. 1), screened in 2 steps according to the inclusion and exclusion criteria. To check the clarity of these criteria, 3 reviewers (M.M.H.J., S.J.E., J.E.F.) screened the first 30 titles and abstracts before discussing the criteria to ensure consensus. Two reviewers (M.M.H.J., S.J.E.) then independently reviewed the remaining titles and abstracts to determine eligibility. We calculated the percentage agreement: interrater reliability was 96%. 42 Each full text was subsequently examined by one reviewer (M.M.H.J.). The third reviewer (J.E.F.) checked discrepancies and uncertainties, and made the final decision in discussion with the reviewers. Where the age at diagnosis was unclear, the full article was read and we included those with explicit mentions of adolescents and/or young adults.
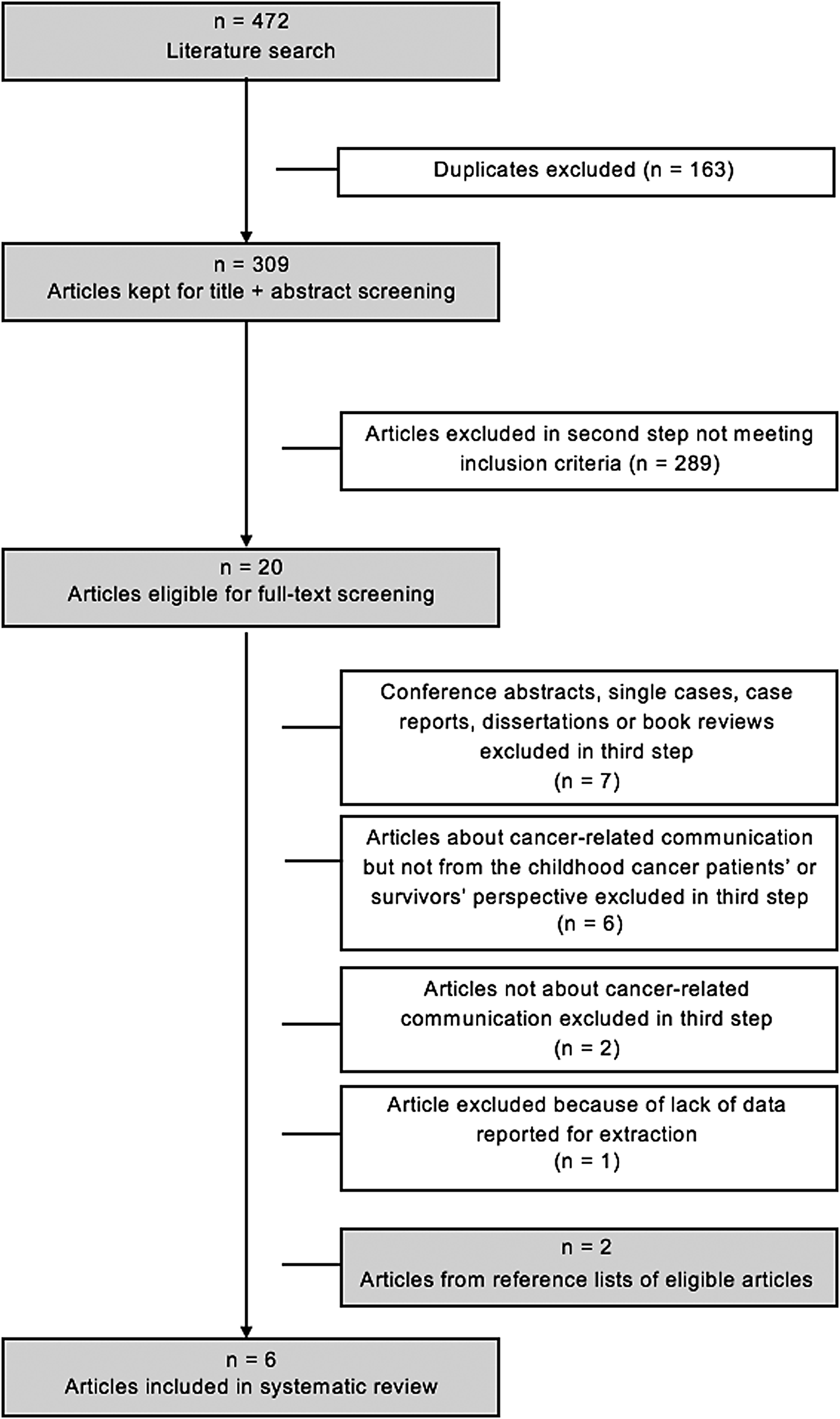
Flow diagram of study selection and review.
Quality assessment
The quality of eligible articles was examined using Kmet et al's 43 checklist for assessing qualitative studies. We chose this tool for its breadth, and because it was suitable for studies which employed interview and online-based methods, such as online discussion groups and blogs. To check the clarity and suitability of the checklist, two reviewers (M.M.H.J., S.J.E.) did an independent pretest of two articles and discussed their results. The number of disagreements was 2 out of 20. After discussion of the discrepancies, one reviewer (M.M.H.J.) reviewed all remaining articles.
Data extraction
Data were extracted using a standardized data extraction form by one reviewer (M.M.H.J). Another reviewer (S.J.E.) also extracted data from two articles (33%) to confirm reliable extraction; reliability was 95%. We gathered material relating to study design and population characteristics. Data extraction items included authors, year, title, journal, date of search, database source, abstract, study type, method, country, number of participants and genders, response rate, recruitment, study time frame, population name, mean age at diagnosis, age at time of study, cancer patients or survivors, treatment phase or time since treatment, treatment type, types of cancer, center or hospital, and ethnicity. To generate analytical themes, we gathered details of cancer-related communication, including who was involved, and what, how, when, and why it occured. 44 We also identified the benefits and challenges associated with communicating with peers reported by each article. 44 Themes for data extraction were developed to comprehensively represent multiple aspects of communication and were further adapted throughout the process to reflect data thoroughly. Generating analytical themes allowed us to synthesize data in a way that answered the research questions of our review. 44 According to Thomas and Harden, 44 this method also allows us to synthesize qualitative studies in a transparent and explicit manner. One study was excluded at this stage as insufficient data were reported for extraction.
Results
Our review analyzed six studies addressing cancer-related communication with family and peers (Fig. 1 and Table 2). All studies were qualitative, representing the experiences of childhood cancer patients and survivors, with diverse cancer diagnoses. Data were collected through semistructured and narrative interviews (n = 3, 50%), or from online communication, such as online discussion groups and blogs (n = 3, 50%), between 2000 and 2014. Where data were available (n = 3, 50%), age at the time of participation and time since treatment ranged from 16 to 34 and 0 to 22 years, respectively. In studies where age at the time of participation was not specified (n = 3, 50%), the population was referred to as “adolescents” and/or “young adults.” Over 134 participants were represented and sample sizes ranged from 7 to 46 participants, including both genders (proportion of females ranged from 56.8% to 100%). Quality scores ranged from 75% to 95% and were above the 75% threshold for the exclusion of qualitative articles according to Kmet et al. 43 The most commonly neglected item was reflexivity (n = 2, 33.3%), but all studies demonstrated connection to a theoretical framework and description of systematic data collection methods (n = 6, 100%).
CNS, central nervous system; N/A, not available.
Talking about cancer
Most patients and survivors communicated about their cancer with others, but described it as a complex process with many obstacles.
What young people talk about when they talk about their cancer?
AYAs reported that disclosing their diagnosis was one of the hardest aspects of having cancer, and felt they had to contain their emotions to protect loved ones. 45 Medical aspects of cancer were discussed in the context of treatment failure/success, treatment-related side effects, or to exchange views on different treatment options.46,47 Changes in physical appearance were also discussed by some survivors who found them burdensome. 47 In one study of online blogs, participants expressed how they were physically isolated, for example during long hospital stays. 47
Survivors communicated medical information illustrating attainment of survival milestones, such as time since diagnosis. 46 The paradox of survivorship was also highlighted: prolongation of the cancer experience was characterized by mixed feelings of excitement and worry about the future.46,47 Some participants reflected on profound existential issues in their online blogs.46,47 Patients and survivors expressed thoughts about their own death or peers' death, 46 but this was rare among patients with advanced disease, 47 who discussed concepts of limited time and transitoriness, in the context of having to face their own mortality. 46 Future uncertainties were communicated in terms of cancer prognosis and general future life plans.47,48
Patients and survivors explored cancer as part of their identity. Many described cancer as a battle, whereas some framed it as something to live with rather than fight against. 47 There was wide diversity in the frequency and amount of information participants were willing to share; females appeared to disclose more routinely and extensively in two studies.45,49 Three studies showed that factual details were more frequently and easily shared compared with emotional aspects.45,49,50 For survivors in one study, this was found to be predominantly true in romantic relationships. 50
Who do young people talk to about their cancer?
Participants in the reviewed studies varied in who they were willing to divulge cancer-related information. In three studies, participants shared information online, demonstrating a desire to share their experience with a wider audience, although this forum provides some anonymity and most users were other patients and survivors.46–48 Many patients were open about their cancer diagnosis with friends, colleagues, and family, but did not wish the information to be “general information” or well known. 45 The decision about who to disclose to was often influenced by recipients' age, personal experience, and relationships.45,49 For example, older recipients, such as teachers and parents of friends, or people with similar experiences were described as easier to talk to, and more sympathetic.45,49,50 Survivors' willingness to disclose appeared strongly associated with the anticipated closeness of the relationship 49 ; however, some survivors found it particularly difficult to discuss the emotional side of their cancer with romantic partners. 50
When/why do young people talk about their cancer?
Communication was often prompted by others. Participants reported having to share cancer-related information when questioned about visible side effects, such as alopecia and scars.45,47,49 When communication was initiated by the participant, it typically occurred at times of uncertainty or clinically meaningful times, such as diagnosis, treatment failure or success, and survival milestones.46,48 Although a minority wished to leave their cancer behind them, most survivors considered cancer a continuing experience rather than a finite event. 49 It was therefore relevant to talk about cancer for most participants, especially in significant relationships.46,47,49 Cancer was discussed when planning for the future; for example, therapy-related infertility in the context of having children. 45 However, a minority of survivors in one study (12%) were reluctant to share their diagnosis, either because they detached cancer from their identity, or considered their treatment as “easy” and felt undeserving of sympathy. 49
Methods of communication
One study of 26 survivors found that survivors disclosed information about their cancer verbally (65.4%), written (30.8%), or behaviorally (23.1%). 49 Written disclosure occurred through multiple mediums, such as school essays, assignments, 49 and online blogs and communication.46–48 Whereas behavioral disclosure included participating in activities and events related to cancer, such as survivorship groups. 49 Participants often used humor and communicated through perspectives of acceptance and gratitude.45–47 When patients divulged news about their cancer, this was commonly presented in a dichotomous framework as either “good” or “bad.” Patients also tended to take a pragmatic, clinical approach when sharing their results with others, but appeared less likely to expand on emotional implications. 46
Benefits and challenges of cancer-related communication
The reviewed studies found patients and survivors had an overall disposition to disclose, which was encouraged by a supportive environment. Participants generally described cancer-related communication as helpful, and sharing the burden with others was used as a coping mechanism.45,46,49 In contrast, keeping the diagnosis secret was felt as dishonest by some patients; others found public disclosure useful in preventing rumors.45,46 Online communication was a source of support, which helped survivors deal with uncertainty, thanks to the support of others. 48
Three studies reported barriers to self-disclosure. A recurrent obstacle was negative peer reactions, such as surprise, incomprehension, or immaturity. 49 Participants were often disappointed by peers' lack of curiosity and reluctance to talk about their cancer.49,50 They also feared it might affect their relationships such that friends or partners would treat them differently, or exclude them from social groups.45,49,50 They were especially apprehensive of being perceived as weak, or being subject to undesired pity and excessive sympathy.45,49,50 One study showed that cancer types affecting sex organs, such as cervical or testicular, were also associated with fear of stigma and exclusion. 45
Discussion
Our review contributes to the literature surrounding social late effects of cancer in AYAs. We identified 6 studies looking at cancer-related communication in young patients and survivors, representing over 134 participants. Although it became evident that communication was an individualized, complex process, we found recurrent themes and patterns relating to medical and existential aspects of cancer.45–50 Emotional topics were more difficult to discuss.45,49,50 Communication occurred on a spectrum with variation in who information was shared with as well as differences in the frequency at which information was shared and the amount and type of information shared.45–50 Communication about cancer often occurred at times of uncertainty or clinically significant times, or was also initiated by others.45–49 Most participants shared their experience orally, using humor and gratitude.45–47,49 Communication yielded benefits as a coping strategy, prompted social support, and appeared central to significant relationships.45,46,48,49 Nonetheless, barriers hindered participants' willingness to disclose, especially peer reactions and fear of stigma.45,49,50
This review also highlighted an intricate link between the extent of cancer-related communication and how significant the relationship is for the AYA survivor. 49 According to Erikson's theory of psychosocial development, 51 establishing one's unique identity may be a prerequisite for developing intimacy with others. Hence, survivors, who generally integrate cancer into their identity, found communicating about cancer important with loved ones. However, some survivors did report difficulties discussing cancer with romantic partners, potentially hindering the establishment of intimacy. We hypothesize that the relationship's importance, mixed with strong feelings and the desire to be loved, could exacerbate fears of stigma and rejection, or fears that the partner's attitude will change. While challenges developing and maintaining intimate relationships are common to AYAs, having cancer may complicate this process. 52 Social skills training with a focus on communication in close relationships could potentially assist AYA survivors with these issues.
Changes in physical appearance were discussed by participants, from both medical and emotional perspectives. One possible explanation is physical changes directly affecting patients' and survivors' body image and self-esteem.1,53,54 Self-ratings of physical appearance have been linked with degree of feelings of isolation. 53 Discussing physical side effects may help patients and survivors cope with them, consistent with the notion of cancer-related communication as a coping mechanism. Physical side effects also triggered communication: participants being questioned about them, 49 as they are often the only visible aspect of cancer. In addition to making patients and survivors feel different from peers, 23 physical differences are associated with increased risk of bullying and anxiety. 25 In two recent studies bullying was reported by over 33% of patients, three times the rates of healthy controls. These studies also found over 75% of cases of bullying related to the illness itself or physical changes,25,26 which may greatly impact patients' and survivors' social functioning and quality of life.25,55 Lähteenmäki et al. 25 found bullying incidence was lowered by educating classmates about cancer. Promoting cancer-related communication skills could enhance understanding and acceptance by cancer-free peers, assisting in a smoother education or occupational reintegration. 1
A major barrier to communicating about cancer, identified in this review, was concern about potential peer reactions. Participants found it easier to talk about cancer with older recipients.45,49,50 This may be due to differences in perspectives and priorities between participants and same-aged peers. 50 Having cancer has been correlated with increased emotional maturity, through posttraumatic growth. 17 Patients and survivors often develop a stronger sense of life purpose and a more optimistic and determined attitude.17,56 As a result, patients and survivors often perceive same-aged peers as immature and harder to relate to,57,58 which may explain why communicating with older recipients was found to be easier. Discussing cancer was also easier when recipients shared similar experiences. 49 Improved social support from peers has also been shown in studies focusing on oncology camps and other peer support interactions.59,60 Participants felt understood, accepted, and learned from each other's experiences. 61 Support from peer patients and survivors is extremely valuable, but maintaining and developing friendships with cancer-free peers remain a key desire of patients and survivors. 59 As cancer is rare in young people,21,62 healthy peers are unlikely to understand the cancer experience and what its impact is for patients and survivors. 63 A possible interpretation is that poor understanding causes avoidance of talking about cancer: peers may not know what to say and fear distressing their friend,34,64 which may be interpreted as disinterest. It is therefore important for young patients and survivors to be aware of these issues to be able to facilitate the conversation.
Limitations to our review included an overrepresentation of studies from developed, English-speaking countries and from female participants. Cancers with specific challenges, such as the central nervous system or sex organ tumors8,45 were included. This may have limited generalizability and biased our results, although it allowed for more diversity. The small number of studies identified by the initial search suggests that the search terms used may have been too restrictive. While a supplementary review of reference lists from eligible articles yielded several additional articles, the literature analyzing our topic is clearly limited. As a result, we included both patients and survivors across a broad age range, including adolescence and young adulthood in our review. The small number of studies and heterogeneous population also limited our capacity to identify variations in communication difficulties associated with particular treatment status or age groups, emphasizing the need for further research. A strength of this review was inclusion of studies using complementary in-depth interview-based and online communication methods. Interviews allowed for specific aspects of communication to be studied with predetermined questions and prompts, whereas online methods enabled participants to express themselves freely, discussing any aspects of cancer.
Our review found that participants were often asked about their cancer by other people. Although many AYAs reported being willing to talk about their cancer, some found it difficult to discuss with same-aged peers. This suggests that further research is needed about cancer-related communication with peers, to develop evidence-based interventions promoting awareness and social skills. This is essential because education and employment re-entry are major milestones, providing a sense of “normalcy,” but are commonly associated with social difficulties.1,8,18,23 Communication is important to strengthen social relationships and support.32,33 Improving understanding of healthy peers could also enhance acceptance.1,25 Our review also found that cancer-related communication was complex and personal. More research is needed regarding patients' and survivors' specific needs and preferences for interventions. Over 25% of survivors have reported a general need for information regarding talking about cancer with friends, 39 but very few interventions have been developed and examined to date, with most targeting brain tumor survivors specifically.65–68 Future research should be targeted at subpopulations, considering developmental and social differences between AYAs and the implications in terms of communication, social issues, and interventions suitability.1,62
We found that cancer-related communication was personal and circumstantial, influenced by both communicating parties as well as the situation. Cancer-related communication, including medical, emotional, and existential aspects of cancer, seemed important, yet complex, for young patients and survivors. Clear communication-related benefits, including coping and social support, emphasize the need to overcome difficulties faced by patients and survivors. Promoting social skills could enhance social functioning, maximizing quality of life. As such, social late effects should be of prime concern for oncology professionals treating young people, from diagnosis through to survivorship, to enable the provision of support and holistic care to their young patients.
Footnotes
Acknowledgments
The authors thank Sophie Newsome and Digby Allen for their writing assistance to this review. C.E.W. is supported by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1143767). J.E.F. is supported by The Kids Cancer Project. The Behavioral Sciences Unit (BSU) is proudly supported by the Kids with Cancer Foundation. The BSU's survivorship research program is funded by the Kids Cancer Project and a Cancer Council NSW Program Grant PG16-02 with the support of the Estate of the Late Harry McPaul.
Author Disclosure Statement
No competing financial interests exist.