
Abstract
Purpose:
Adolescent and young adult (AYA) head and neck cancer (HNC) patients require longer term follow-ups as they age; yet, little is known about factors associated with survivorship in this population. We aimed to describe nonclinical factors associated with HNC survivorship among AYAs.
Methods:
In this retrospective cohort study, the Surveillance, Epidemiology and End Results 18 database from 2007 to 2014 was queried. Eligible cases were 15–39-year-old primary HNC patients with known cause of death (n = 1777). Kaplan–Meier survival curves stratified by age group (15–29, 30–34, and 35–39) and by health insurance status tested differences in HNC survival among groups with a log-rank test. Variables, including age, sex, race/ethnicity, county-level poverty, anatomic site, stage, and treatment, were controlled for in a competing risk proportional hazards model.
Results:
Patients were mostly male (64%), with mean age of 33.4 years. Survival rate was 73% after 8 years of follow-up. There were no significant survival differences based on age at diagnosis. However, AYAs who were on Medicaid (adjusted hazard ratio [aHR] = 1.61, 95% confidence interval [CI] 1.22–2.12) or uninsured (aHR = 1.51, 95% CI 1.03–2.21), had an increased hazard of death from HNC, compared with those with private insurance.
Conclusion:
Health insurance status is the main nonclinical factor associated with survival among AYAs with HNC, and individuals with Medicaid do not fare better than the uninsured. With a potential longer term follow-up in this AYA population, there is need to optimize survivorship irrespective of health insurance status.
Introduction
H
The incidence of HNC in the young has continued to increase since the 1970s.7,8 Across the United States, oral/tongue cancer in particular has increased dramatically in the last three decades in individuals younger than 45 years, with 60% increase reported in 2002, and an alarming 111% increase reported for young white women in 2011.9,10 Oropharyngeal cancer also significantly increased among white males, 18–49 years, from 1975 to 2007. 11 As adolescents and young adults (AYAs) with HNC live longer in the general population, it will become more important to track the potential for treatment effects, late toxicities, and comorbidities associated with their cancer. 12
While several studies have documented increasing incidence of HNC among AYAs,7–10,13 little is known about survival patterns in this population. The only known nationally representative study that described survival in the young adult HNC population 10 focused heavily on incidence and on white males and females, excluding blacks and other racial/ethnic minorities. With HNC survival disparity heavily skewed toward minority and the underserved populations,14–16 it is important to examine the patterns of survival-related disparities, if any exist, in the AYA HNC population.
The aim of this study was to characterize survival of HNC in the AYA population. Findings could help identify subgroups that may need more attention to optimize survival.
Methods
Data were retrieved from the Surveillance, Epidemiology and End Results (SEER) 18 database run by the National Cancer Institute (NCI). 17 SEER 18 encompasses about 27.8% of the total U.S. population from registries in 18 regions of the country 18 and includes cases diagnosed from 2000 to 2014. 17 Cases were selected from 2007 because the SEER database included the insurance variable from 2007. 19 Because SEER 18 is publicly available deidentified data, this study was exempt from consideration by the Saint Louis University IRB.
An NCI report in 2006 described AYA cancers as those diagnosed in patients between 15 and 39 years. 20 This age group definition, which has been extensively used in AYA cancer studies,21–23 was adopted for this study.
We included patients diagnosed with malignant first primary HNC between 2007 and 2014. HNC subsites were defined as the International Classification of Diseases O-3, site recodes for hypopharynx (C12.9–C13.9), larynx (C32.0–C32.9), nasopharynx (C11.0–C11.9), oral cavity (C00.0–00.9, C02.0–C02.3, C03.0–C03.9, C04.0–C04.9, C05.0–C05.9, C06.0–C06.9, C07.9–C08.9, and C14.8), oropharynx (C01.9, C02.4–C02.9, C09.0–C09.9, C10.0–C10.9, and C14.0–C14.2), and sinonasal areas (C30.0–31.9 excluding C30.1) and histologic types 8050–8076, 8078, 8083, 8084, and 8094. Patients were excluded if the only documentation of their cancer was from a death certificate or autopsy, if cause of death was unknown, or were listed as alive but had no survival time. Data were retrieved using SEER*Stat version 8.3.4 (Surveillance Research Program, NCI).
Measures
The outcome of interest was death from primary HNC. SEER provides a cause-specific death classification variable that considers patients' number of tumors, site of first cancer, and comorbidities to reduce cause of death misclassification, 24 and our analyses used this variable as the outcome of interest. SEER also provides patients' survival time in months from month of diagnosis to month of last contact.
The primary independent variable was age at HNC diagnosis, which was grouped as 15–29, 30–34, and 35–39 years for survival curve analysis and left continuous for multivariate analyses. Covariates included year of diagnosis, stage (I, II, III, IV, and unstaged/unknown), site (hypopharynx/larynx, nasopharynx, oral cavity, oropharynx, and sinonasal areas), surgical treatment (yes, no), race/ethnicity (Hispanic, non-Hispanic [NH] black, NH white, NH other [Alaska Natives, American Indians, Asians, and Pacific Islanders]), insurance status (insured, Medicaid, uninsured, and unknown), and county-level poverty percentage. We used health insurance as a proxy for socioeconomic status (SES), in the absence of individual patient data such as income and employment.25–27
Statistical analyses
Chi-squared tests and independent-sample t-tests, where appropriate, determined preliminary associations for age and covariates with death from any cause. Chi-squared test also determined if uninsured or Medicaid patients presented with advanced-stage disease compared with patients with private insurance. Kaplan–Meier survival curves were plotted over the entire follow-up time using cause-specific mortality from HNC in which those who died from a cause other than HNC were censored. The survival curves were stratified by age and insurance status, and log-rank tests with Bonferroni adjustments for multiple comparisons determined if there were significant survival differences overall among the strata.
Three multivariate proportional hazards models utilizing cumulative incidence functions to handle competing events as described by Fine and Gray 28 were fitted to determine hazard of death from HNC. The first model included demographic independent variables (county-level poverty percentage, age at diagnosis, year of diagnosis, sex, and race/ethnicity); the second included demographic and clinical covariates (stage, site, surgery, and radiation); and the third included demographic and clinical covariates along with insurance status. The event was death from HNC, and death from other causes during follow-up was considered a competing event using Fine and Gray methods. 28 Those who did not die from any cause during follow-up were censored.
Likelihood ratio tests were performed comparing each successive model that added covariates with the previous model (demographic vs. demographic/clinical and demographic/clinical vs. demographic/clinical/insurance) to determine if each expanded model yielded a better fit than the previous simpler model. These models yielded adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) to determine significant predictors of death from HNC. All tests were two tailed and alpha was set at 0.05. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Demographics and survival curves
Our patient population included 1777 AYAs diagnosed with HNC. The majority of patients were aged 35–39 (55%), male (64%), NH white (61%), oral cavity cancer (35%), and insured (67%) (Table 1). The average age at diagnosis was 33.4 years (standard deviation = 5.5 years).
SD, standard deviation.
At the end of the 96-month (8-year) follow-up time, the survival probability for the AYA HNC cohort was 0.73, and the cohort did not reach median survival (50%) during follow-up. When stratifying the survival curves by age group, the log-rank test did not find a significant difference between groups (p = 0.71) (Fig. 1). However, there was a significant overall difference among insurance groups (log-rank p < 0.001), and the curves indicated that the order of highest survival was insured patients, uninsured patients, and patients with Medicaid (Bonferroni p-values <0.001) (Fig. 2).
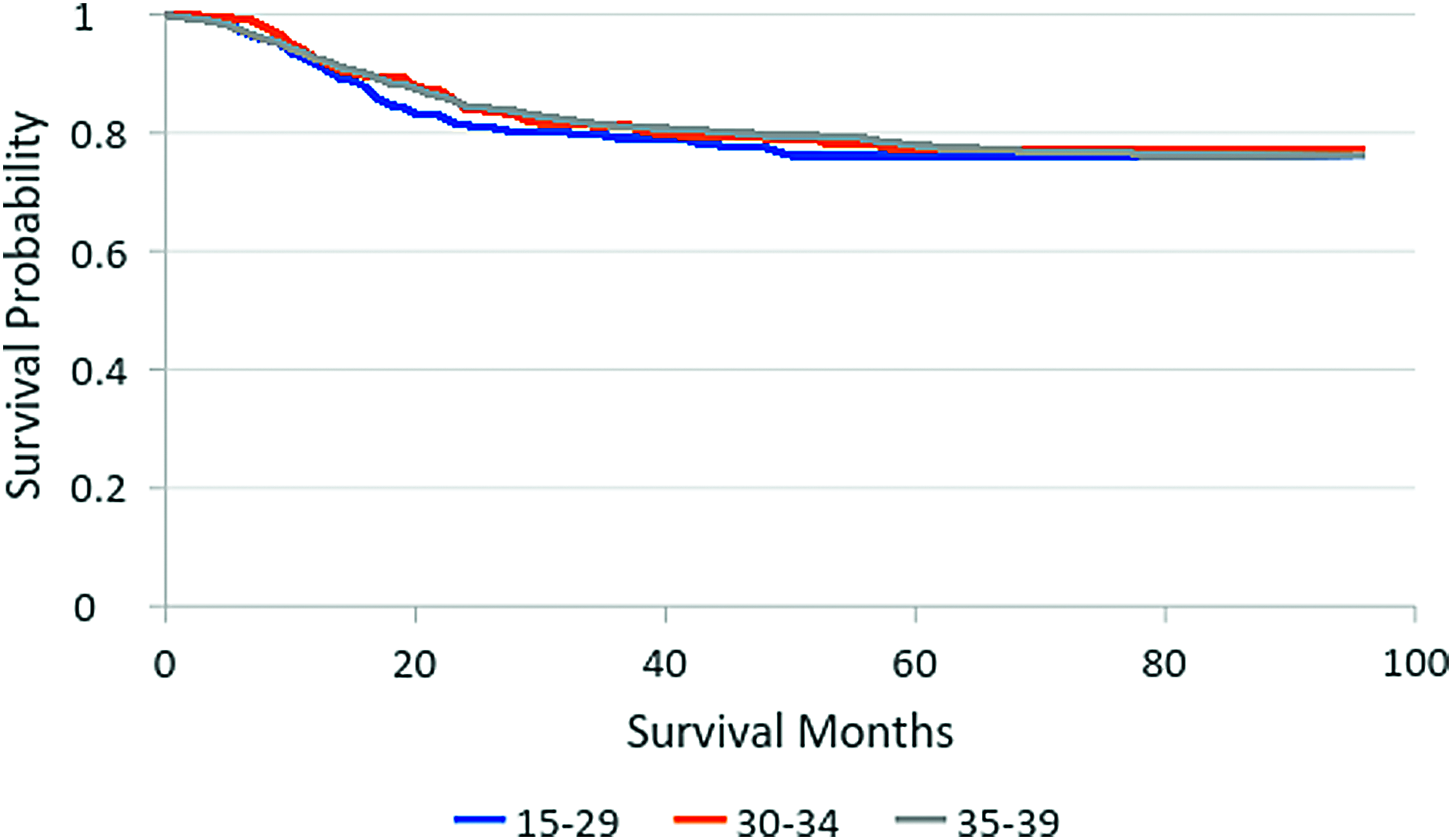
Kaplan–Meier survival curves stratified by age. Kaplan–Meier survival curve showing differences in survival rates based on age of diagnosis among the AYA HNC cohort in the study. Curves show that survival rates were not significantly different based on age groups (15–29, 30–34, and 35–39). AYA, adolescent and young adult; HNC, head and neck cancer. Color images available online at www.liebertpub.com/jayao

Kaplan–Meier survival curves stratified by insurance. Kaplan–Meier survival curve showing differences in survival rates based on health insurance status among the AYA HNC cohort in the study. Curves show that there is a difference in survival rates based on health insurance status, and AYA HNC survivors on Medicaid had the lowest survival rate, followed by those uninsured. Those with private insurance had the best survival rate in the cohort. Color images available online at www.liebertpub.com/jayao
Stage by insurance
The chi-squared test between stage of HNC presentation and insurance indicated an association between the two variables (p < 0.001). There was a higher percentage of insured patients presenting at stage I (28%) than those with Medicaid (13%) and who were uninsured (18%). There were only minor differences between insurance status for stages II and III, but patients with Medicaid (51%) and who were uninsured (46%) had higher percentages of presenting at stage IV than insured patients (33%) (Table 2).
Multivariate models
The three likelihood ratio tests indicated that each successive model (demographics [−2 log likelihood = 4409.7], demographics/clinical covariates [−2 log likelihood = 4182.6], and demographics/clinical covariates/insurance [−2 log likelihood = 4167.8]) fit the data better than the previous model (p < 0.01 for both likelihood ratio tests), indicating that the model with demographics/clinical covariates/insurance was the best fit for the data out of the three models.
In the model of best fit, insurance status was a significant predictor of death from HNC, with patients on Medicaid (aHR = 1.61, 95% CI 1.22–2.12) and who were uninsured (aHR = 1.51, 95% CI 1.03–2.21) being more likely to die from HNC compared with those who were insured (Table 3). Age at diagnosis was not a significant predictor of hazard of death from HNC (aHR = 0.99, 95% CI 0.97–1.01), nor was year of diagnosis (aHR = 1.02, 95% CI 0.96–1.08). Males also did not experience a different hazard of HNC death than females (aHR = 1.01, 95% CI 0.79–1.29), and while the model indicated that those of non-Hispanic other race were more likely to die from HNC during follow-up (aHR = 1.47, 95% CI 1.05–2.07) than non-Hispanic whites, the overall effect of the race/ethnicity variable was not significant (p = 0.16). County-level poverty percentage, however, was a significant demographic predictor of death from HNC (aHR = 1.03, 95% CI 1.01–1.05).
CI, confidence interval.
All clinical covariates except for radiation were significant predictors of death from HNC. Compared with patients with stage I HNC, patients with stages II (aHR = 5.10, 2.55, 10.21), III (aHR = 7.38, 95% CI 3.68–14.78), IV (aHR = 11.94, 95% CI 6.13–23.28), and unstaged/unknown (aHR = 5.31, 95% CI 2.65–10.63) HNC had an increased hazard of death from HNC. Patients with hypopharyngeal/laryngeal (aHR = 0.48, 95% CI 0.30–0.75), nasopharyngeal (aHR = 0.38, 95% CI 0.24–0.60), and oropharyngeal (aHR = 0.54, 95% CI 0.39–0.75) cancer had a decreased hazard of death from their primary cancers compared with patients with oral cavity cancer. Patients who did not receive surgery were 58% more likely (aHR = 1.58, 95% CI 1.17–2.13) to die from HNC compared with those who did receive surgery, while not receiving radiation did not significantly impact hazard of death (aHR = 1.00, 95% CI 0.72–1.40).
Discussion
The objective of this study was to understand survivorship and predictive factors of HNC among AYAs, aged 15–39 years. We found no significant HNC survival differences between AYAs based on age at diagnosis. Our results corroborate previous studies that found no significant survival differences in nasopharyngeal, oral cavity, and oropharyngeal squamous cell carcinoma in AYAs <40 years of age, based on age at diagnosis.29,30 This finding may be explained by the lower duration of exposure to carcinogens in tobacco and alcohol in the AYA population compared with adults. 31 Llewellyn et al. noted that smoking for 21 years or more increased the odds of acquiring a head and neck malignancy with lower odds in those <45 years of age. 32 Therefore, tobacco- and alcohol-related HNC risk factors may be more applicable to older adults. 33 This suggests that HNCs occurring in the AYA population may be due to causes other than tobacco and alcohol, for example, sporadic mutations and inherited syndromes.31,34
Oral cavity was the most common cancer site in our study, and these patients had higher hazard of death compared with the other subsites, except sinonasal cancer. This is significant because previous studies from the United States and Scandinavia have reported significant increase in the incidence of oral cavity cancer among AYAs, especially young women.10,35,36 Previous studies indicate that oral cavity cancer among younger patients could be a distinct disease, 37 different clinicopathologically, 34 and more aggressive than that found in older patients. 38 In addition, since younger patients are expected to tolerate optimal treatments and have significantly higher survival rates than older patients, 34 there have been calls for more aggressive treatments among younger HNC patients. 38
However, a superior survival rate does not eliminate treatment-related toxicities and quality-of-life issues these AYAs will face in their lifelong cancer survivorship journey. 39 Younger at age diagnosis has been shown as a predictor of poor quality of life among HNC survivors. 40 It is therefore important that these patients are provided adequate support post-treatment to optimize survivorship.
While age at diagnosis did not impact survivorship, one important question answered by our study is that insurance status is a main nonclinical risk factor associated with HNC survivorship in the AYA population. We found that AYAs who are uninsured or on Medicaid faced increased hazard of death from HNC compared with those who are insured. Previous studies on cancer and noncancer outcomes have used health insurance as a proxy for SES.25–27 Poor survival in AYAs with public insurance or no insurance has been documented in 11 major cancers affecting this population.19,41,42 However, there is limited research on how health insurance impacts survivorship in AYAs with HNC. Without health insurance, AYAs are more likely to experience delays in treatment initiation, 43 and present with advanced stage 44 or metastatic disease. 45
In addition, AYAs who are uninsured are less likely to receive definitive treatment 45 and have higher rates of treatment nonadherence.46,47 Even past the initial treatment phase, AYAs with no insurance are less likely to receive cancer-related medical care for long-term survivorship compared with those with insurance. 48 In addition, the quality of care may also differ, since uninsured patients are less likely to receive rehabilitative therapies. 49 This is significant because younger cancer patients typically have longer follow-up years based on their age of diagnosis; thus, any lack of optimal long-term survivorship plan for these patients is likely to impact not only their survival but also the overall quality of life.
The importance of health insurance status in the survival of AYA with HNC is heightened by the fact that this population is known to have the highest uninsured rates compared with children or adults. 44 In the absence of private insurance, a government insurance should ideally provide some access to care; however, our study showed that AYAs on Medicaid had significantly worse overall survival than those who were uninsured or with private insurance. The adverse association between being uninsured or on Medicaid and survival may be explained by stage of presentation. Previous studies have shown that cancer patients, including AYAs on Medicaid or uninsured, have higher odds of presenting with advanced-stage disease, and had higher risk of death from cancer.50,51
The fact that having Medicaid, compared with being uninsured, did not mitigate survival disparity is a concern for AYAs. It could be that individuals under Medicaid may be underinsured, 52 and that Medicaid may not cover all the major health expenses and services for optimal cancer care compared with private insurance. 53 A previous study found that HNC may be the most expensive cancer to treat in the United States and that individuals with commercial insurance are more likely to receive the multiple modality treatment needed than those on government insurance. 54 Thus, AYAs with HNC who are on Medicaid may be underinsured. This could manifest as deferring seeking cancer care, delays in filling prescriptions, or general poor compliance to treatment modalities, 53 all of which could contribute to poor survival outcomes.
Another potential explanation may be due to timing of Medicaid enrollment. Many HNC patients, including AYAs, are known to be enrolled into Medicaid only after their cancer diagnosis. 51 Since the majority of AYAs present with regional and distant stage disease at the time of official Medicaid enrollment,55,56 the apparent lack of survival benefits for Medicaid patients in this study may be due to the late stage of presentation of these patients. There is a need to further investigate the potential impact of Medicaid or uninsured status on AYA patients with HNC, especially since AYAs, due to their age at diagnosis, are likely to require longer term follow-up in the course of surviving their cancer.
Since more than 50% of HNC patients do not return to work due to their cancer and the side effects of treatment, 54 private insurance may be unattainable for many AYAs, and those who have private insurance through employment could lose coverage or more find it difficult to obtain adequate health coverage. 57 If these patients become disabled and are unable to return to work due to their cancer treatment and cannot afford private insurance, then there need to be interventions designed to optimize survivorship, thus closing the disparity gap between those with private insurance and those uninsured or on Medicaid.
This study has several limitations. First, given the retrospective nature of the SEER database, causal inferences could not be made. Furthermore, although being the largest population cancer database in the United States, SEER does not include common risk factors of HNC such as alcohol/tobacco use and HPV status. Individual patient income and level of education are also not available in the SEER database.
The small sample size in this study due to the rarity of HNC in young adults also limits the power of the analysis. The insurance variable was also only recently added to the SEER database (2007), further limiting our ability to analyze trends associated with insurance status and survivorship for earlier years, or for older data available through SEER. Also, any potential change in insurance status in the continuum of care is not captured in the SEER database, so we are unable to describe the potential effect of change in insurance status on cancer survivorship. SEER also does not have information on job or employment status of patients, which is also associated with possession of health employer-based private insurance. 57
Notwithstanding these limitations, this study does make a valuable contribution to HNC literature. Our findings show a significant relationship between health insurance status and HNC survivorship in the AYA population, highlighting a nonclinical factor that could significantly impact survivorship as well as quality of life of AYAs with HNC. This study also lends credence to past work that there is a strong, independent relationship between insurance status and risk of death due to cancer for AYA patients with cancer.58,59
In conclusion, our study showed that survival did not differ among the AYA HNC population based on age of diagnosis. However, we described the impact of health insurance status on survival, and highlighted survival disparity in the uninsured/Medicaid-dependent AYA HNC population. Since the lack of health insurance is a major issue in the AYA population, 44 it is critical that future interventions target cost-effective care in this population. With potential repeal of the Affordable Care Act and loss of the mandate to cover young adults until 26 years on their parent's health insurance, we may see worse cancer outcomes in the AYA population. In the meantime, efforts should be made to improve access to care and survivorship in the AYA HNC population irrespective of health insurance status. This is probably the most important step in closing the health insurance-dependent survival disparity gap that currently exists in the AYA HNC population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.