
Abstract
Purpose:
The aim was to study follow-up care attendance in adolescent and young adult (AYA) cancer survivors to investigate: (1) correlates of the intention to attend follow-up care and (2) whether the intention is associated with the actual attendance, applying the theory of planned behavior (TPB).
Methods:
We conducted a questionnaire survey in AYA cancer survivors diagnosed 1990–2005 at age 16–25 years, registered in the Cancer Registry Zurich and Zug, Switzerland, who had survived at least 5 years. Structural equation modeling was applied to investigate TPB-related correlates (attitudes, subjective norms, and perceived behavioral control) of intention to attend follow-up care. Logistic regression analysis was used to study the association between intention and actual attendance.
Results:
We included 160 AYA cancer survivors in the study (mean age at study: 34.0 years, mean age at diagnosis: 21.6 years, 98 [61.3%] male). Positive attitudes toward follow-up care (coefficient = 0.32, 95% confidence interval [CI]: 0.05 to 0.60) and supportive subjective norms (coefficient = 0.59, 95% CI: 0.41 to 0.78) were associated with higher intention to attend follow-up care. Perceived behavioral control was not associated with intention to attend (coefficient = −0.13, 95% CI: −0.36 to 0.10), but with actual attendance (odds ratio [OR] = 4.55, 95% CI: 1.83 to 11.31). Higher intention was associated with actual follow-up care attendance (OR = 14.29, 95% CI: 5.80 to 35.21).
Conclusion:
Positive attitudes and supportive social norms were associated with higher intention to attend follow-up care, and higher intention was associated with actual follow-up care attendance. Increasing awareness of the importance and benefits of follow-up care not only among survivors but also family, friends and healthcare professionals may help increase follow-up care attendance among AYA cancer survivors.
Introduction
F
Research showed that female and older survivors were more likely to attend recommended follow-up care,4,10 and attendance rates decreased with more time after diagnosis.11–14 More than 5 years after diagnosis, 40% of survivors reported not having attended a routine medical visit during the last year. 14 Furthermore, lower quality of life and more health problems were associated with more medical out-patient visits in long-term survivors, 10 indicating that there might also be a link to follow-up care attendance.
Perceived barriers to attend medical care included lack of insurance, high costs,13,14 no guidance from the oncologist, no perceived need for follow-up care,13,15 not enough information regarding follow-up care, conflict with other responsibilities such as family and work, fear of new cancer, and avoidance of care related to the former cancer disease. 15
Knowledge on cognitive correlates of follow-up attendance is still lacking. To address this gap, we applied the theory of planned behavior (TPB 16 ; Supplementary Figure S1 in Supplementary Data; Supplementary Data are available online at www.liebertpub.com/jayao) to investigate cognitive correlates of follow-up care attendance in a population-based sample of AYA cancer survivors in Switzerland. The TPB suggests that the intention to perform a behavior predicts the actual behavior. The intention itself is predicted by three constructs: attitudes toward the behavior (referred to as attitude), subjective norm (norm), and perceived behavioral control (control). In addition to the intention, the actual behavior is predicted by control. Attitude refers to a person's favorable or unfavorable opinions about the behavior of interest, norm refers to perceived expectations among the social environment to perform the behavior, and control refers to the perceived easiness or difficulty to perform the behavior. Generally, more positive attitudes and norms, and greater control are expected to be associated with a higher intention to perform the behavior, and a higher likelihood that the behavior is actually performed. 16 Survivors' positive attitudes toward follow-up care, the perception that family, friends, and health professionals support or expect their attendance, and the perceived easiness to attend care are thus expected to increase the intention of survivors to attend follow-up care.
The aim of our study was to investigate whether the TPB helps predicting follow-up care attendance in Swiss AYA cancer survivors. Specifically, we aimed at investigating: (1) TPB-related correlates of the intention to attend follow-up care, and (2) whether the intention is associated with the actual attendance.
Methods
Study participants
Eligible survivors had been diagnosed with cancer in the Canton of Zurich, Switzerland, between 1990 and 2005, aged 16–25 years at diagnosis, registered in the Cancer Registry Zurich and Zug, Switzerland, and survived ≥5 years after diagnosis. Cancer diagnoses were restricted to leukemia, germ cell tumor, lymphoma, central nervous system (CNS) tumor, neuroblastoma, renal, hepatic and bone tumor, and soft tissue sarcoma to enable comparison with a cohort of Swiss childhood cancer survivors.17,18
Procedure
A mailed questionnaire survey was conducted between August 2010 and January 2012. Addresses of eligible survivors were available from the registry. After 4 weeks, a reminder letter was sent to nonresponders. The study was approved by the Cantonal Ethics Committee of Zurich, and informed consent was obtained from all participants.
Assessment of correlates, intention, and attendance
Correlates (attitude, norm, and control) and intention were measured by indicator variables, which were assessed using 7-point Likert scales (Supplementary Table S1 in Supplementary Data). Questions were developed according to the TPB manual by Francis et al. 19 Attitude was measured by asking for the agreement with five items: “I find regular follow-up unnecessary–meaningful; bad–good; unpleasant–pleasant; boring–interesting,” and “To me, detecting and treating possible late effects of my cancer is unimportant–important.” Norm was assessed asking for the degree of agreement with the following items: “Most people that are important to me think I should attend to follow-up care.”; “It is expected from me that I attend to follow-up care regularly.” Control was measured using three items: “For me, attending regular follow-up is complicated–easy; stressful–not at all stressful,” and the degree of agreement with “It is foremost in my hands whether I regularly attend follow-up or not.” Finally, intention was assessed by asking for the degree of agreement with two items: “I intend to attend follow-up next year.” and “It is likely that I will attend follow-up within the next year.” To assess follow-up care attendance, survivors were asked whether they still attended follow-up care. We coded those who attended regular or irregular follow-up as attenders and those who rarely or never visited their former treating doctor as nonattenders 11 (Supplementary Table S1 in Supplementary Data).
Covariates
Sociodemographic characteristics
Sex was assessed in the questionnaire and obtained from the registry for nonparticipants. Age at study, educational achievement, employment status, partnership, and migration background were assessed in the questionnaire. Educational achievement of survivors was coded as compulsory schooling, vocational training, upper secondary education, and university degree. 20 Survivors were classified as having a migration background if they were not Swiss citizen, had moved to Switzerland after birth, or if they were not Swiss citizen since birth.
Clinical characteristics
Late effects, cancer relapse, and second malignancies were assessed in the questionnaire (yes/no). Furthermore, survivors were asked if they were afraid that late effects are detected when attending follow-up care (7-point Likert scale).
Clinical information from the registry
Information on diagnosis (classified according to the International Classification of Childhood Cancer, Third Edition—ICCC-3 21 ), age at diagnosis, treatment, and time since diagnosis were extracted from the registry. Treatment was hierarchically coded as surgery only, chemotherapy (may have had surgery), and radiotherapy (may have had surgery and/or chemotherapy).
Statistical analysis
Descriptive statistics, chi-square tests, and t-tests were used to compare participants and nonparticipants.
Aim 1: Structural equation modeling
We used structural equation modeling (SEM) to investigate correlates of the intention to attend follow-up care. SEM allows investigating associations between latent (unmeasured) factors based on measured indicator variables. A two-step approach to SEM was used. 22 First, an adequate measurement model was built; then the TPB-based structural model was added. The final SEM consisted of two parts: a measurement model depicting the relationships between indicators (indicator variables from the questionnaire) and latent factors (correlates and intention) and a structural model representing the paths between latent factors (Fig. 1).
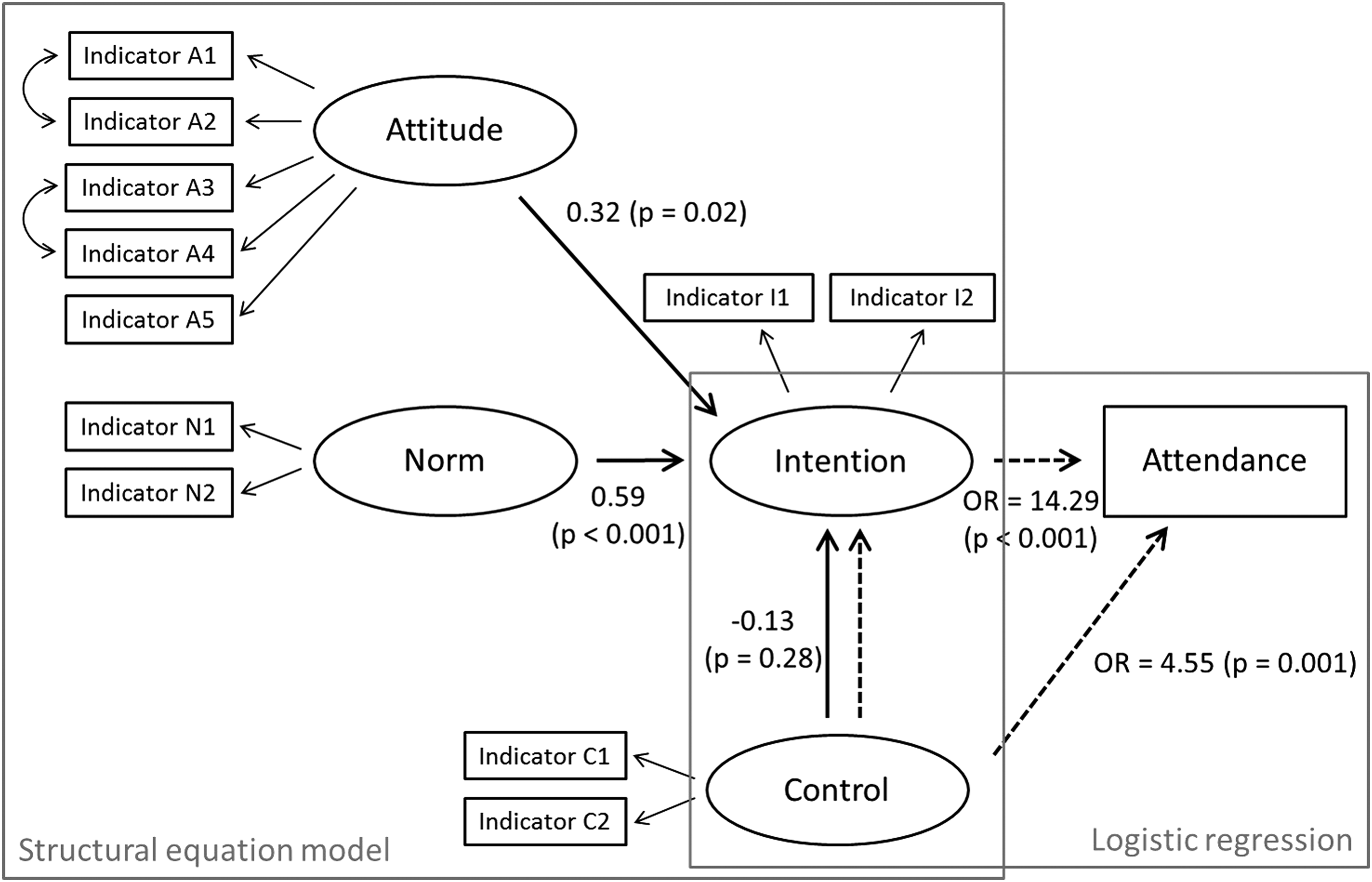
Predictors of intention to attend follow-up care (structural equation model) and actual follow-up care attendance (logistic regression analysis) in Swiss adolescent and young adult cancer survivors according to the theory of planned behavior. Ovals indicate latent factors (three predictors and intention), rectangles indicate measured variables (indicators and actual attendance), straight arrows indicate paths included in the structural equation model, curved arrows indicate freed covariances between indicators included in the structural equation model, and dashed lines depict the logistic regression analysis. OR, odds ratio.
The measurement model consisted of four parts representing the four latent factors attitude, norm, control, and intention measured by indicators. Higher scores indicate more positive attitude, more supportive norm, higher control, and higher intention. Cronbach's alpha measuring internal consistency was calculated for the four latent factors. Principal component factor analysis (PCFA) was applied for each factor separately to test whether the indicators loaded on one factor each. A confirmatory factor analysis (CFA) was conducted for the four factors together. Modification indices (MI) based on CFA and theoretical justification were used to modify the measurement model. The structural model consisted of three paths pointing from the correlates to intention (Fig. 1).
Maximum likelihood estimation taking into account all available information in the data in the presence of missing values was applied. Thus, no imputation of missing values was necessary to run the SEM. To estimate the precision of the model parameters, the robust Huber/White/sandwich estimator was used.
To assess goodness of fit, the following measures were used: chi-squared test statistic, root-mean-square error of approximation with corresponding 90% confidence interval (CI), and the standardized root-mean-square residual for overall model fit, and Comparative Fit Index and Tucker–Lewis Index for the comparison with baseline models. 23 For programming reasons, the goodness of fit measures had to be obtained without applying the robust standard error estimation.
Aim 2: Logistic regression analysis
We applied multivariable logistic regression analysis to investigate the association between intention and actual attendance to follow-up care (Fig. 1). Control and intention were included in the analysis as factor scores derived from the measured indicators. For the calculation of the factor scores, missing values in indicators were imputed with the mean of the available indicators of control or intention, respectively.
Covariates
Sociodemographic and clinical covariates were included in the SEM and multivariable logistic regression analyses if they were associated with intention or attendance in univariate regression analyses at p < 0.05 level. Consequently, both analyses were adjusted for age at study, time since diagnosis, late effects, relapse, new cancer, and fear of detecting late effects during follow-up care (Supplementary Table S2 in Supplementary Data). In addition, they were adjusted for sex. Age at study and time since diagnosis were included as continuous variables.
Statistical analyses were carried out using Stata version 14.2 (StataCorp LP, College Station, TX).
Results
Study participants
Among 469 cancer survivors eligible for the study, 389 (82.9%) could be contacted. Of those, 160 (41.1%) returned the questionnaire and were included in the analysis.
The mean age of the participants was 34.0 years, and 98 (61.3%) were males. Their mean age at diagnosis was 21.6 years. The most common diagnosis among the participants was lymphoma (60, 37.5%), followed by germ cell tumors (46, 28.7%), CNS tumors (15, 9.4%), and soft tissue sarcomas (15, 9.4%). One-third of the participating survivors was treated with surgery only (57, 35.6%), 36 (22.5) with chemotherapy, and 41 (25.6%) with radiotherapy. About a quarter of AYA cancer survivors (44, 27.5%) reported to suffer from late effects.
Participants and nonparticipants were similar regarding sex, age at study, diagnosis, cancer treatment, age at diagnosis, and time since diagnosis (Table 1). More than half of the survivors (n = 92; 57.5%) reported to attend follow-up care.
Bone tumors, neuroblastoma, renal tumors, and soft tissue sarcomas were combined in a category called “other tumors” for the analyses.
Missing values; percentages are based on the total number of participants/nonparticipants.
p-Value calculated from t-test statistics (continuous variables) and chi-square test statistics (categorical variables) comparing participants and nonparticipants.
Information was not available for nonparticipants.
Vocational training reference category for the regression analyses.
AYA, adolescent and young adult; CNS, central nervous system; ICCC-3, International Classification of Childhood Cancer—Third Edition; n, number; n.a., not available; SD, standard deviation.
Structural equation modeling
Internal consistency measured by Cronbach's alpha was α = 0.80 for attitude, α = 0.88 for norm, α = 0.99 for intention, and α = 0.43 for control. According to the PCFA, the indicators for attitude, norm, and intention loaded on one factor each (Supplementary Table S3 in Supplementary Data). The indicators for control loaded on two factors, one for the indicators C1 and C2, and another one for indicator C3. Therefore, indicator C3 was excluded for further analyses. Internal consistency was α = 0.71 for indicators C1 and C2 of control.
The MI of the CFA proposed to free the covariances between two pairs of attitude indicators (indicators A1 and A2: MI = 35.5; indicators A3 and A4: MI = 29.3). Since these two indicators were also related from a theoretical point of view, the covariances were freed. The loadings of the indicators on the factors were strong and statistically significant (Supplementary Tables S4 and S5 in Supplementary Data).
The results were similar with and without robust standard error estimation with slightly larger confidence intervals without the robust estimation. The CFA showed acceptable to good model fit (23) (Supplementary Tables S4 and S5 in Supplementary Data).
Aim 1: Correlates of intention
Positive attitude toward follow-up care (coefficient = 0.32, 95% CI: 0.05 to 0.60) and higher supportive norm (coefficient = 0.59, 95% CI: 0.41 to 0.78) were associated with higher intention to attend follow-up care (Table 2, Fig. 1). Control was not associated with intention (coefficient = −0.13, 95% CI: −0.36 to 0.10). Having had a relapse was associated with higher intention. The model explained 73.8% of the variance in intention. The results were similar with and without robust standard error estimation. The model showed acceptable to good model fit. 23
p-Values <0.05 are indicated in bold.
Based on 133 observations, since SRMR can only be obtained without taking into account observations with missing values.
Criteria and goodness of fit according to Schermelleh-Engel et al. 23
Degrees of freedom = 85 for the structural equation model.
CFI, Comparative Fit Index; CI, confidence interval; df, degrees of freedom; RMSEA, root-mean-square error of approximation; SRMR, standardized root-mean-square residual; TLI, Tucker–Lewis Index.
Aim 2: Intention and actual attendance
Both, higher intention to attend follow-up care (odds ratio [OR] = 13.77, 95% CI: 5.58 to 33.95) and higher control (OR = 6.30, 95% CI: 2.26 to 17.53) were associated with actual attendance (Table 3, Fig. 1). Having late effects, having had a relapse, and higher fear of detecting late effects during follow-up care were associated with attendance to follow-up care (Table 3).
p-Values <0.05 are indicated in bold.
OR, odds ratio; CI, confidence interval.
Discussion
We found that positive attitudes towards follow-up care and the perception that the social environment expects the survivor to attend follow-up care (supportive norms) were associated with higher intention to attend follow-up care in Swiss AYA cancer survivors. Survivors with a higher intention to attend follow-up care and those who perceived it to be easier to attend (higher perceived control) were more likely to actually attend follow-up care.
Facilitating and promoting positive attitudes toward follow-up care might help to increase follow-up care attendance in AYA cancer survivors. With more time passed since diagnosis, attendance rates to follow-up care decrease 11–14 and also attitudes toward follow-up care worsen. 4 Thus, it might be especially important to sustain and promote positive attitudes among long-term survivors. Also, attitudes of healthcare professionals toward follow-up care might influence attitudes of survivors and thus follow-up care attendance: other studies found that reasons to not attend follow-up care were that survivors felt that healthcare professionals would not have enough time to provide care, 10 or that there was no guidance from their oncologist regarding follow-up care. 15 Thus, not only survivors but also healthcare professionals should be continuously informed about the importance of follow-up care.13,15 This might be achieved by implementing survivorship care plans, 24 as there seems to be a lack of age-appropriate information for AYA cancer survivors.4,25–32
Supportive social norms might also increase follow-up care attendance. Although AYAs are mature, parents play an important role during and also after the end of treatment. 33 We found that expressing the importance of follow-up and the expectation that survivors attend follow-up increased the intention to attend follow-up. This is in line with a reason for not attending medical out-patient visits found in another study: nonattending survivors perceived that healthcare professionals felt survivors would not need follow-up care. 13 Thus, families and friends of survivors and healthcare professionals should be advised about their role in supporting survivors to attend follow-up care what is expressing the importance and expectation of attendance.
We did not find perceived control being associated with the intention to attend follow-up but with actual attendance. Survivors generally reported finding it easy to attend follow-up care (Supplementary Table S1 in Supplementary Data). These results might mirror the fact that due to the small country size, well-maintained public transport system, and mandatory health insurance in Switzerland, it is straightforward to attend follow-up care if a survivor is willing to do so. Thus, logistics, healthcare system, or insurance-related barriers to attend medical care identified in other studies13–15 might not hold for Switzerland. Perceived control might still be increased by providing survivors with guidance regarding follow-up care by for instance implementing survivorship care plans. 24 Survivorship care plans might help empowering survivors to take responsibility for their health, for instance by attending regular follow-up care. Furthermore, high perceived control is only possible if follow-up care is available and ideally tailored to the needs of AYA cancer survivors. In other studies, survivors reported the need for age-appropriate follow-up care that is accessible, affordable, and flexible to be compatible with work and family.4,13,25,34 Regarding organization of follow-up, care led by an oncologist in an adult hospital was preferred,11,35 a multidisciplinary team involved was favored as well.11,30,33 Medical reasons for follow-up were rated higher than supportive reasons by both, survivors11,35 and healthcare professionals. 36 Thus, follow-up care should include the provision of diverse information, including former cancer disease and treatment,24,32 and monitoring for late effects. But follow-up care should also include psychosocial support services outside the clinical setting, and cover aspects such as insurance or employment issues.4,35
The presence of late effects, having had a relapse, and higher fear of detecting late effects during follow-up were associated with actual attendance in our study. Suffering from late effects and relapse of cancer make it necessary to seek medical care. A main aim of follow-up care is to detect late effects. The fear of detecting late effects might thus be due to this awareness. On the contrary, survivors attending care might be more anxious in general, and have a higher need for monitoring their health. Our findings are in line with a study in Canada reporting that most common reasons for medical care visits in AYA cancer survivors were secondary neoplasms and other health-related symptoms. 12 In contrast, a study in the United States found the fear of new cancer being a barrier to attend follow-up care. 15 This contrast might be due to a culturally influenced higher need for monitoring and higher perceived control to attend care in Switzerland compared with the United States.
A limitation of our study is its cross-sectional design. Therefore, we are not able to draw conclusions on the temporality of the investigated TPB-related correlates and intention and actual follow-up care attendance. Furthermore, follow-up attendance was self-reported and might not reflect actual attendance correctly. The response rate of 41.1% is relatively low, but in the same range as response rates in questionnaire studies among childhood cancer survivors. 37 Also, AYAs are a heterogeneous and mobile population 34 difficult to reach and include into studies.38,39
One of the strengths of our study is the use of the widely used TPB 40 to investigate correlates of intention and actual attendance in AYA cancer survivors. Another strength is the population-based sampling of AYA cancer survivors. Our study participants were comparable to nonparticipants suggesting that the study sample is representative for AYA cancer survivors in a large and diverse region of Switzerland. Furthermore, we observed similar results in a cohort of Swiss childhood cancer survivors, 17 which strengthens our findings.
In conclusion, we found positive attitudes and supportive social norms being associated with higher intention to attend follow-up care, and higher intention being associated with actual follow-up care attendance. Increasing awareness of the importance and benefits of follow-up care not only among survivors but also family, friends, and healthcare professionals may help increase follow-up care attendance among AYA cancer survivors.
Footnotes
Acknowledgments
The authors thank all survivors for participating in our survey, the Cancer Registry Zurich and Zug, Switzerland for its support, and the members of the study team (Philip Läuppi, Anna Hohn, Zina Heg-Bachar). This work was supported by the Swiss National Science Foundation (Ambizione fellowship PZ00P3_121682/1 and PZ00P3_141722 to G.M.; grant 100019_153268/1) and the Swiss Cancer League (KFS-02631-08-2010).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.