
Abstract
Purpose:
Adolescent and young adult (AYA) cancer survivors experience fertility and childrearing challenges in adulthood, but there is limited evidence on awareness, beliefs, and concerns about oncofertility in this population, needs for supportive resources, and associations with quality of life (QoL).
Methods:
Participants were 69 AYAs aged 12–25 who were diagnosed with cancer at age 18 years or younger and ≥1 year cancer free, recruited from childhood cancer clinical records and support organizations. Participants completed self-report assessment of oncofertility knowledge and beliefs, information needs, and measures of QoL. Analyses examined associations between oncofertility-related variables and QoL.
Results:
Knowledge and beliefs about oncofertility options were considerably low in the sample, and participants reported unmet oncofertility resource needs. In multivariable analyses, QoL was associated with beliefs valuing the importance of fertility in childhood cancer (β = 0.87, p = 0.01) and lower information needs (β = −1.19, p = 0.022).
Conclusions:
Infertility is a well-documented effect of childhood cancer treatment. Our findings indicate that clinical providers are a preferred source of information for AYA patients, and there is a need to address oncofertility concerns and challenges in this group. Research is needed to examine barriers to addressing fertility issues in childhood cancer treatment and ways to promote dialogue between providers and patients and their families.
Introduction
D
Fertility preservation methods such as embryo cryopreservation, gonad shielding and oophoropexy, and sperm collection before therapy are available8–11 ; however, they are not equally accessible to all patients due to prohibitive costs and limited availability at pediatric cancer treatment centers. 10 Other factors may also impede discussions providers have with young patients and their families about fertility risks at the time of cancer treatment, including patients' and providers' lack of awareness, resources, opportunity, or time with respect to treatment initiation.5,12–17 Organizations such as the American Society of Clinical Oncology have developed recommendations for clinicians to discuss infertility risks and preservation resources with patients and families, but evidence suggests fewer than half of oncologists follow such recommendations.17–19
Available data suggest that pediatric cancer patients and families who discuss fertility and preservation options with their providers at the time of diagnosis experience improved quality of life (QoL). Failing to do so is associated with poorer long-term QoL and psychological well-being.3,13 Unfortunately, many AYA survivors continue to report gaps in their understanding of oncofertility and preservation options,5,20 but evidence in this area remains limited. This study examined patient-reported knowledge and perceptions of oncofertility risks, oncofertility information needs, and associations with QoL in a sample of AYA survivors of pediatric cancer.
Methods
Sample and setting
Eligible participants were AYA cancer survivors aged 12–25 years who were diagnosed with cancer at age 18 years or younger, were at least one year post-treatment with no relapse at the time of screening, and able to read and speak English. The study took place at a pediatric hematology/oncology clinic located within an urban cancer research and treatment center in Washington, DC. The clinic provides inpatient and outpatient services, including follow-up care and late effects programs to a large, diverse patient population. The study also partnered with community-based organizations that serve AYA cancer survivors in the clinic's geographic catchment area to identify potentially eligible patients who may reside in the community and not treated at the clinic. The protocol was approved by the host institution's Institutional Review Board. Participants aged 18 years and older provided written informed consent; those younger than 18 years of age provided written assent with parental consent.
Recruitment and study procedures
Potentially eligible participants were identified through the clinic's medical records and by posting study recruitment advertisements in electronic communications of partnering community-based organizations (e.g., email newsletters, social media posts). Potential participants identified through clinic records were initially contacted with information about the study by postal mail. In response to the mailing, those interested in participating could contact study staff, and recruitment mailings included a card that could be returned by those who were not interested. Study staff conducted telephone follow-up among those who did not respond to initial mailings. Advertisements in communications from community-based organizations directed interested individuals to contact study staff directly. All recruitment materials invited potentially interested patients (and parents, where appropriate) to be part of a study about reproductive health issues and QoL related to cancer treatment. For all participants, eligibility was confirmed by telephone, and once participants were determined to be eligible, they were mailed a packet describing study procedures and containing age-appropriate informed consent/assent forms. Eligible, consenting participants completed a self-administered survey and returned it to study staff by mail.
Measures
Demographics and clinical characteristics
Demographics assessed included age, gender, and race/ethnicity. Educational attainment and household income were assessed among young adults and parents' of adolescents. Information on cancer diagnosis was abstracted directly from patient medical records where available. Telephone follow-up was conducted among participants with archived clinical records and those recruited through community-based organizations to ascertain information on cancer diagnosis.
Oncofertility knowledge and beliefs
Oncofertility knowledge was measured using a 14-item scale capturing self-assessed knowledge of reproductive health, infertility, and fertility preservation in the context of pediatric cancer (α = 0.91).21,22 Response options for each item ranged from “Nothing” (0) to “A lot” (3) and were summed to create a score indicating greater self-assessed knowledge (possible range 0–42). Beliefs indicating the importance of oncofertility risks and preservation were assessed using 10 items with response options ranging from “Not at all” (0) to “Very Much” (4). 23 Responses to the items were summed to create a score (possible range 0–40) indicating greater importance of oncofertility risks and preservation (α = 0.74). Perceived risk of infertility was assessed using a single valid item assessing perceived risk of infertility compared with similarly aged peers who were never diagnosed with cancer. 24 Response options ranged from “Much less” (1) to “Much more” (5).
Oncofertility information needs
Oncofertility information needs were measured using six face valid items adapted from previous research. 25 Items assessed participants' perceived need for information about oncofertility risks and preservation from oncologists, nurses, fertility specialists, other cancer patients, print materials, or internet-based resources. Response options ranged from “Not at all” (1) to “Extremely” (4). These items were descriptively examined individually and were summed to create a score (possible range 6–24) indicating greater perceived oncofertility resource needs (α = 0.82).
Emotional well-being
Emotional well-being was assessed by the Center for Epidemiologic Studies Depression (CES-D) scale, a valid measure used in population and epidemiological studies to measure depressive symptoms. 26 The scale includes 20 items with response options ranging from “None of the time” (0) to “Most of the time” (3). Responses were summed to create a score (possible range 0–60) with higher scores indicating poorer emotional well-being (α = 0.88).
Quality of life
Patient-reported QoL was assessed with the Pediatric Oncology Quality of Life Scale.27,28 This 21-item measure captures multiple QoL domains, including daily activity, emotional, social, and cognitive functioning. Responses to each item range from “Never” (1) to “Very frequently” (7) and were summed (possible range 21–147) to create a global score with higher values indicating poorer QoL (α = 0.90).
Statistical analysis
The statistical analysis occurred in several steps. Descriptive analyses were conducted for all variables measured, including item-level analyses of participants' reported oncofertility resource needs. Multiple linear regression was used to examine associations among oncofertility knowledge and perception variables, emotional well-being, and global patient-reported QoL. Age (adolescent/young adult) and gender (male/female) were also included as control variables in these analyses given previous research indicating varying oncofertility risks and outcomes by these characteristics. 29
Results
Descriptive statistics
In total, 148 potentially eligible, interested individuals responded to study mailings or recruitment communications. Of those, 69 (49%) met eligibility criteria, consented, and completed study procedures. Descriptive statistics for the sample (N = 69) are shown in Table 1. A majority of individuals in the sample were young adults (n = 46; 67%) with a mean age of 19.6 years (standard deviation [SD] = 3.9). Most were non-Hispanic white (72%) and previously diagnosed with leukemia or lymphoma (61%). Of those not diagnosed with leukemia or lymphoma, the most common diagnoses were central nervous system malignancies (n = 10, 14%). The mean knowledge score was relatively low overall (M = 13.1, SD = 8.5). The belief that oncofertility risks and preservation are important was moderate (M = 21.7, SD = 7.0). Individuals' perceived risk of infertility compared to their peers were about average (M = 3.8, SD = 1.0) and the need for information through various sources was moderately high (M = 13.8, SD = 4.5). Global QoL, where a lower score indicates positive QoL, was high in the sample (M = 48.8, SD = 20.2).
SD, standard deviation.
Figure 1 illustrates AYA survivors strongly preferred learning about possible effects of cancer treatment on reproductive health through a fertility specialist (61%) or oncologist (55%). Other trusted sources to address information needs were through a nurse (33%), peer-led supports such as other patients (32%), print (26%), or internet materials (25%).
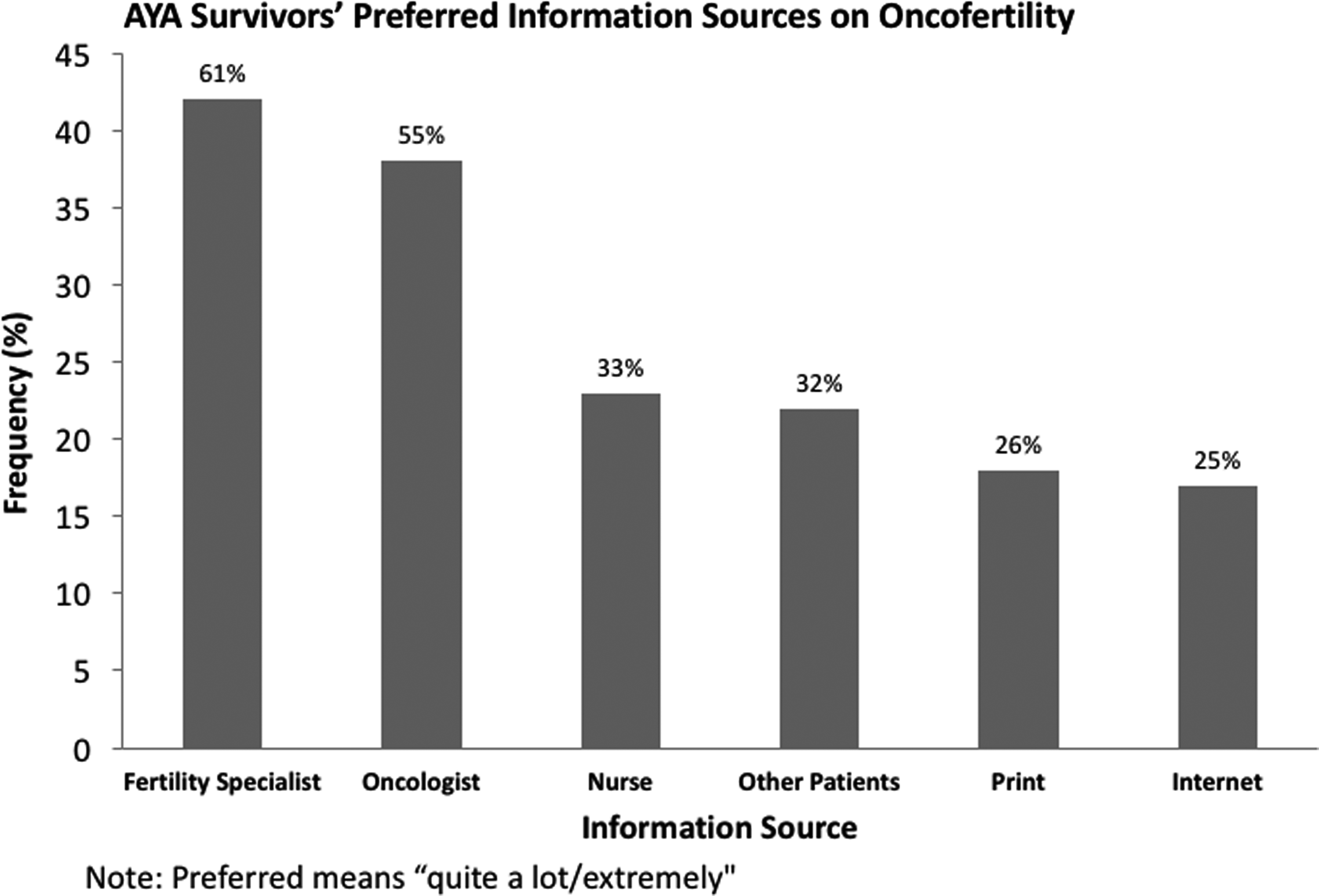
Adolescent and young adult survivors of pediatric cancer oncofertility information support needs.
Multivariable analysis
Multiple linear regression was run to examine individual level factors, which might be predictive of QoL. Results are reported in Table 2. Significant predictors associated with poorer QoL included an increased score of beliefs that infertility is important (β = 0.87, p = 0.01), lower information needs (β = −1.19, p = 0.022), and lower emotional well-being (β = 1.12, p = 0.001), controlling for all factors in the model. Other variables including age, gender, knowledge, and perceived infertility risk relative to peers were not significantly associated with QoL in the model. Overall, the model significantly explained 50% of the variance in reported QoL.
SE, standard error.
Discussion
Multiple patient-, provider-, and system-level barriers affect AYA cancer survivors' opportunities to discuss fertility preservation options with providers at the time of diagnosis or treatment. 30 This study provides new data on AYA survivors' perspectives surrounding reproductive health and demonstrates associations with overall QoL. Our findings indicate that AYA cancer survivors perceive that treatment-related infertility risks are important, and such beliefs are associated with poorer global QoL. Patients also indicated a need for more information about reproductive health and fertility preservation. Importantly, higher reported need for information was associated with poorer QoL. Our results build from another study demonstrating adolescent cancer patients express a high level of concern about infertility risks, 23 indicating an important unmet need for support resources for oncofertility among young cancer patients and survivors.
Although research on oncofertility issues and concerns in AYA survivors remains limited, evidence demonstrates fertility is a prominent concern among adult cancer patients and provides additional context for our findings.31–33 A recent systematic review of reproductive aged female cancer patients found subjective beliefs about infertility risks were most predictive of poor QoL, regardless of objective measures of infertility. 34 Another qualitative study among adult survivors of breast cancer showed that although some received information on fertility preservation, they were dissatisfied with the information or said that their provider seemed uncomfortable discussing the topic. 32 Another systematic review demonstrated that young women primarily sought fertility information from a fertility specialist or decision aid early in the treatment process. 31 Taken together with our results surrounding AYA survivors of pediatric cancer, this evidence further highlights the need to address infertility risks at the time of cancer diagnosis and treatment.
Potential approaches to address the unmet need for information on fertility risks and preservation among young cancer patients may include education for adolescents and parents,11,35–38 providers and fertility specialists,39–42 and other healthcare personnel.43,44 Investigating optimal ways to support providers to enhance discussions about fertility risks and preservation options also appears warranted. 45 Some recent efforts to support providers include enhancing referral practices to fertility specialists and fertility networks,46–48 guideline development,9,49,50 and decision guides and trees models18,19,51 to ensure that patients are informed of their preservation options. However, there is evidence that providers do not perceive that they have sufficient information to hold discussions with patients,12–15,39,52 indicating continued research into provider-facing strategies is needed.
The study findings should be interpreted in light of important limitations. The study was cross-sectional and involved a local convenience sample, limiting generalizability to other patients and settings. We do not have information to characterize nonresponders, and those who participated may have been more inclined to report on the topics of study. Aside from the clinical characteristics gathered, all data were based on participant self-report, and we did not study provider or parental perspectives. 35 It is possible that methodological factors, including the order of measures on the study assessment, affected participants' reporting. Although we used well-validated measures to capture constructs of interest, we were limited in the ability to parcel out some constructs (e.g., QoL) and examine results in subgroups of participants owing to the relatively small sample size. In the future, it will be important to investigate if the associations reported herein may vary for different domains of QoL (e.g., physical, functional, emotional) that comprise this construct.
Despite these limitations, our study provides new information on beliefs about fertility, information needs, and associations with QoL in AYA survivors of childhood cancer. Our findings reinforce that oncofertility concerns remain an unaddressed need in this patient population, with potential effects on overall patient QoL. In the future, it will be important to investigate if findings vary by clinically relevant factors such as cancer type and infertility risk stemming from diagnosis and treatment. Qualitative investigations will also help to better understand reasons why AYA patients' beliefs and information needs may affect QoL. Research examining strategies for improving oncofertility education for AYA patients and their families at the time of diagnosis and treatment and supporting providers discussing fertility risks and preservation options with patients and families could improve outcomes for this population.
Footnotes
Acknowledgments
This study was supported by a Hope Scholar Grant from the Hyundai Hope on Wheels Foundation. This work was also supported by the Georgetown Lombardi Comprehensive Cancer Center Support Grant under NIH grant no. P30CA051008. The study sponsors had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the study sponsors.
Author Disclosure Statement
No competing financial interests exist.