
Abstract
Purpose:
The diagnosis of cancer is often prolonged in teenagers and young adults (TYA). There may be lessons in improving this from international comparisons. However, international studies are complex and so we conducted a pilot study to examine the key barriers to large-scale research in this field.
Methods:
We provided translated questionnaires covering key aspects of presentation and clinical management within 60 days of a confirmed cancer diagnosis, to patients 13–29 years of age inclusive, to their primary care physicians and to the cancer specialists managing their cancer. We conducted descriptive analyses of the data and also the process of study implementation.
Results:
For our pilot, collecting triangulated data was feasible, but varying regulatory requirements and professional willingness to contribute data were key barriers. The time of data collection and the method for collecting symptom reports were important for timely and accurate data synthesis. Patients reported more symptoms than professionals recorded. We observed substantial variation in pathways to cancer diagnosis to explore definitively in future studies.
Conclusion:
Focused research upon the mechanisms underpinning complex cancer pathways, and focusing that research upon specific cancer types within TYA may be the next key areas of study.
Background
C
There is low awareness of cancer during adolescence and early adulthood, in the public and providers, and healthcare professionals may not immediately recognize TYA cancer symptoms.16–19 Therefore, when TYA develop cancer, they may experience a longer time until diagnosis and treatment than younger children or older adults.20–24 In general, cancers that are more advanced when commencing treatment have poorer outcomes whether due to requiring more treatment (causing greater late toxicity) or through lower treatment success rates, and studying and understanding the time to diagnosis is an important TYA cancer research goal.17,25 While some studies show a direct correlation, the relation between symptom interval and outcome is complex with clinical, biological, and human factors involved.16–19,20,23 Access to primary care maybe relevant and health insurance is sometimes relevant.19,21,26 In a large U.K. primary care cohort study, in the 3 months before diagnosis, 42.9% of TYA with cancer consulted primary care ≥4 times versus 11.5% in age-matched patients without a cancer diagnosis. 27 Almost twice as many TYA visited their general practitioner (GP) more than three times before diagnosis of cancer than is observed in older adults (38% vs. 20%). 28
Understanding international variation in time to diagnosis could assist us in improving outcomes, sharing of best practice, and adhering to consistent research definitions.29,30 Previous and ongoing TYA studies do not allow valid international comparisons or identify where long times to diagnosis may be occurring.17,31 The International Cancer Benchmarking Project (ICBP) module 4 examined the route from symptoms to cancer treatment in adults and their clinicians.31–33
Cooperation over large geographical areas and large datasets are required to reach robust research findings particularly given the relative rarity of TYA cancers. 34 This requires cooperation, infrastructure, and funding. International clinical networks and online data capture may overcome some of these barriers, but introduce others. Within the EU FP7 grant “European Network for Cancer in Children and Adolescents (ENCCA),” between 2011 and 2016, an international collaborative working group of clinicians, researchers, and patients in TYA cancer was initiated. As an initial step to developing formal research proposals, the group developed a pilot study as a test case for future large-scale collaborative research. This was undertaken without study management funding, but based upon the cooperation present within the network, to examine if this process could minimize the need for full funding for future studies.
Study objectives
(1) To pilot collaborative working and data collection within the European TYA cancer community.
(2) To identify and characterize timescales within the diagnostic pathway of cancer in the TYA population.
(3) To examine the consistency of report of waiting times, by the triangulation of the responses of patients with those of clinicians in different healthcare sectors.
Methods
Investigators were approached through the ENCCA network of TYA professionals.
Ethics and regulatory elements
Ethics approval was obtained for the use of shared data collection, security, and storage procedures, according to the various local and international regulations. The age range for inclusion in the whole project spanned 13–29 year olds, although differed in some locations, so two different consent forms were designed. Those under 16 years required both the consent of a parent/guardian and patient assent, whereas those over 16 years consented directly.
Eligibility criteria
Patients
Aged between 13 and 29 years on study entry
Diagnosed with leukemia, sarcomas of bone or soft tissue, lymphomas, central nervous system tumors, and germ cell tumors or carcinoma.
Was receiving or had received care in a contributing specialist center.
Less than 60 days from cancer diagnosis.
Able to complete the questionnaire, with the help from another person if necessary
Professionals
The oncology/hematology specialist involved in the care of the patient
The GP/community/primary care doctor who initially saw the patient and/or made the referral to specialist services.
These professionals were identified by the patient in their questionnaire.
Questionnaires
Questionnaires developed in the ICBP module 431,32 were adapted by experienced cancer clinicians and the research team to better fit the TYA population. The questionnaires contained items related to symptoms, clinical contact/interventions, and time periods. Three different versions were developed; for patients, oncology/hematology specialists, and GPs/primary care physicians.
Patient questionnaire
Each TYA participant was asked for limited demographic and clinical details, but no personally identifiable information was requested (Supplementary Appendix A1; Supplementary Data are available online at www.liebertpub.com/jayao).
When the participant identified their specific diagnosis, they then selected from a list of cancer symptoms compiled by experienced clinical study members, tailored to each cancer type, and including free space to add other symptoms they experienced before their diagnosis. This aimed to focus upon relevant specific symptoms. The patient was also asked about events leading to diagnosis and to estimate dates of key events in their pathway, including dates of first symptoms, referral, diagnosis, and treatment.
Primary care questionnaire
The primary care clinician's questionnaire documented the symptoms of their patient using free text to encourage wide reporting, as well as how many clinical assessments occurred in primary care. They were asked what investigations were ordered and when/how they referred the patient further. The research team wrote the information sheet to help GPs feel confident in participating, by explaining that this research was not designed to criticize them or to imply any mistakes or delays, but to understand processes and compare perspectives when measuring previous events (see GP information sheet in Supplementary Appendix A2).
Specialist questionnaire
The specialist questionnaire asked consultant oncologist/hematologists questions about how the patient was first referred to their service. They were also asked how the patient was diagnosed and the details of their diagnosis and treatment. Again, the information sheet emphasized there was no criticism or implication of delay.
Data collection
A bespoke online system was developed for the data collection in this project, with a unique and secure login system for each participating country that could link patients' data to their GPs and specialists.
The GPs and specialists had the same prefix as their patient, so that the data could be linked for example, GB0101P would be linked with GB0101G and GB0101C. To access the system, each participant was given a login card (Supplementary Appendix A3), for secure use on the survey website to input their patient ID, authentication code, and three grid references (e.g., A1, C5, H2). The grid references changed upon website access, enhancing data security.
Development of the website took 5 months, including piloting with two service users. The questionnaires were translated forward from English into the different languages appropriate and back-translated to ensure accuracy, coordinated by the lead national collaborator.
Each center could access our survey website to review local progress, and generate local login cards for their participants. A Center Management Report allowed the local investigator to see when a patient had completed the questionnaire and also to see the details they had provided for their GP and specialist, to invite those professionals to take part.
Statistical analysis
Descriptive statistics were used to assess the questionnaires completed. Where appropriate, this included reporting the number of missing responses for each question. Questionnaire responses were compared between pairs of responders (e.g., patient and GP) and agreement assessed by the Kappa statistic.
Time differences in the patient pathway between key events were calculated from the dates provided by the patients. We calculated the difference between (1) first symptoms and GP appointment, (2) first symptoms and appointment with a specialist, (3) first symptoms and cancer diagnosis, (4) GP appointment and appointment with specialists, and (5) GP appointment and cancer diagnosis. Patient pathway times were reported by median and interquartile range (IQR).
We compared responses by country for those with the highest number of responders (England, Italy vs. Others, including France, Denmark, and Hungary). Comparison of responses between subgroups (such as age group or tumor type) were not appropriate due to the pilot aims and small sample.
Results
Study approval
Initially seven U.K. departments expressed interest in the study from 4 treatment centers (Leeds x2, Sheffield x2, Birmingham x2, and London) and 13 EU Centers in five countries (Italy, France x5, Spain x5, Hungary, and Denmark). Swedish and German centers could not proceed without funding for ethics and an employee to deliver the project. The timeliness of study opening varied by over 12 months, and it was not always possible to open the study due to available resources (Fig. 1).
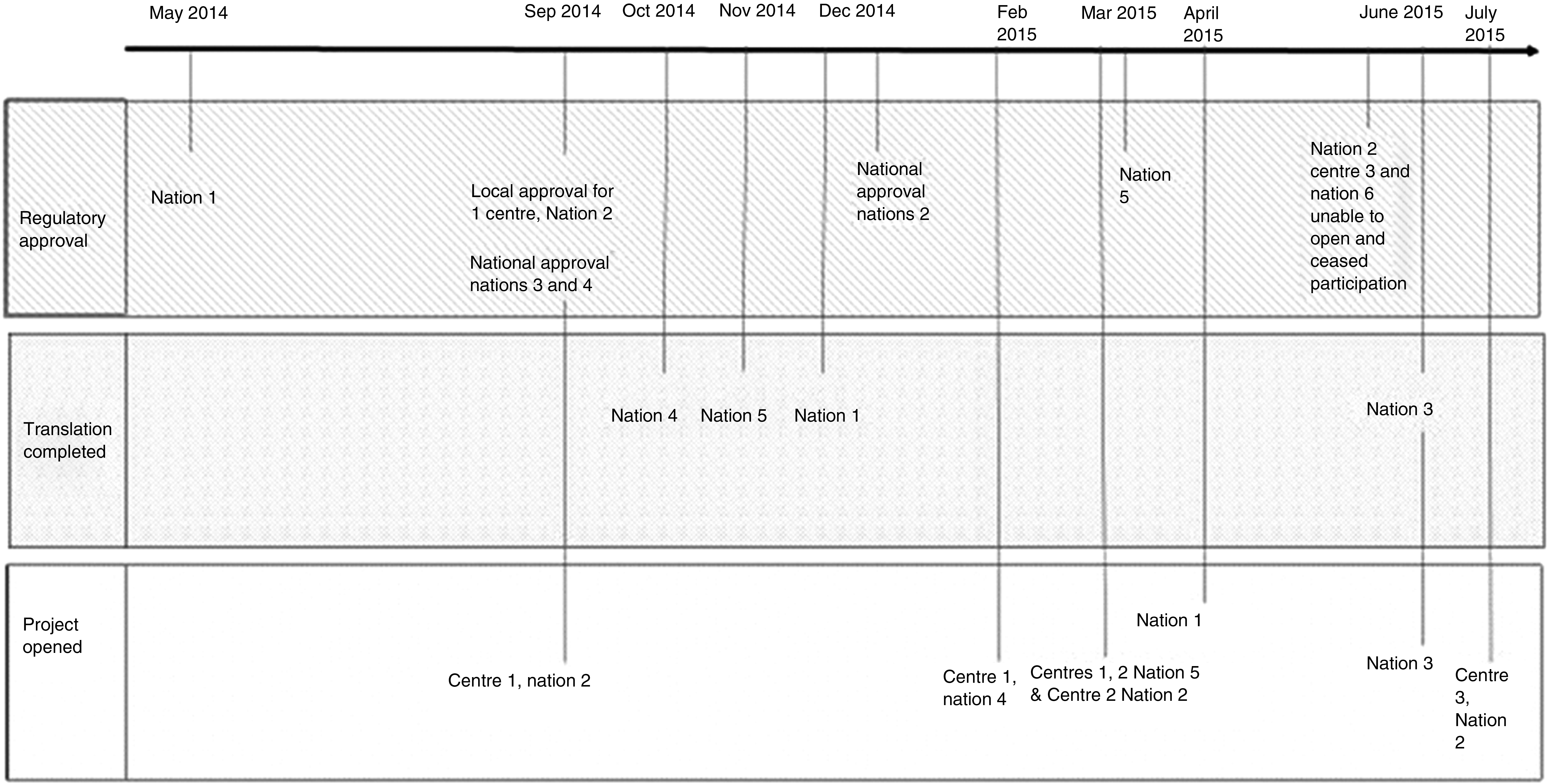
A timeline for the opening of the pilot study, in successful and other initially interested centers.
Data
A total of nine centers in five countries participated; responses for each are shown in Table 1. A total of 68 patients, 42 GPs, and 50 specialist centers completed their respective questionnaires. Responses for all three elements (patient, GP, and specialist center) were completed by 32. While the greatest number of patient responses were completed in England, the other countries, in particular Italy, were more successful in obtaining responses for all three responder types.
GP, general practitioner.
A wide range of symptoms were reported by patients and GPs, with more symptoms reported by patients (Table 2). The most commonly reported symptoms by the patients were: swelling or lump with no pain (31%), bone pain (31%), tiredness (26%), and swelling or lump with pain (18%). Swelling or lump with pain was the most commonly reported symptom by the GP (31%) followed by bone pain (24%).
Other included: drowsiness, enlarged lymph nodes, uncoordinated walking, loss of vision or double vision, high temperature, irregular periods, itching, bruising, enlarged spleen, fever, infection, diarrhea, difficulty swallowing, numbness, problems with writing or doing calculations, recurrent infections, seizures, broken bones, changes in personality and intellect, vomiting, weight gain.
Almost 50% of patients reported seeing their GP between 1 and 4 weeks from first symptoms, and 18% reported waiting more than 1 month with symptoms before contacting a GP. However, 47% of GPs reported that the patients waited more than 1 month with symptoms before contacting them (Table 3). Overall, 39% of patients reported visiting their GP twice or more before diagnosis (Table 4). This was different between countries; 47% in England, 34% in Italy, and 35% in the other countries combined, but not statistically significantly (p = 0.44). The use of emergency hospital services (accident and emergency departments) was low, and consistent between reporters. Referrals direct to cancer specialist teams were uncommon, being more often into a nonspecialist hospital doctor and then onward referral to oncology/hematology.
Thirty-five with both patient and GP-reported duration: Kappa agreement = 46% (moderate agreement).
Other includes Denmark, France, and Hungary.
Within the limitations of our pilot design, we observed shorter median times from symptom onset to specialist appointment and from symptoms to diagnosis in Italy than in the other nations studied and the longest in the United Kingdom (Supplementary Table S1).
Triangulating the data, there was inconsistency of reporting of the diagnostic process (Table 5). Two thirds of patients reported initially seeing a GP about symptoms and 21% reported attending emergency services. A third of GPs reported making an urgent referral for assessment of cancer, whereas only 14% of specialist centers reported receiving a referral from a GP.
Patient question: Which of the following best describes the events which led to your diagnosis of cancer?
GP question: If you made a referral to specialist services, which of the following best describes the nature of this referral?
Center question: How was the patient referred to the hospital/specialist services related to their cancer?
Patients reported a wide range of times between key points on the patient pathway (Fig. 2). The median time between patients reporting symptoms and seeing a specialist was 59 days (IQR 31–130 days). However, patients were then promptly diagnosed after seeing a specialist with the median time from symptoms to cancer diagnosis 63 days (IQR 35–153 days). Where data on time from symptoms to diagnosis were present from several sources (in 18 patients), the reported time differences were modest; mostly under 14 days and never over 30 days. For all time periods there were some patients with extended times on the diagnostic pathway.
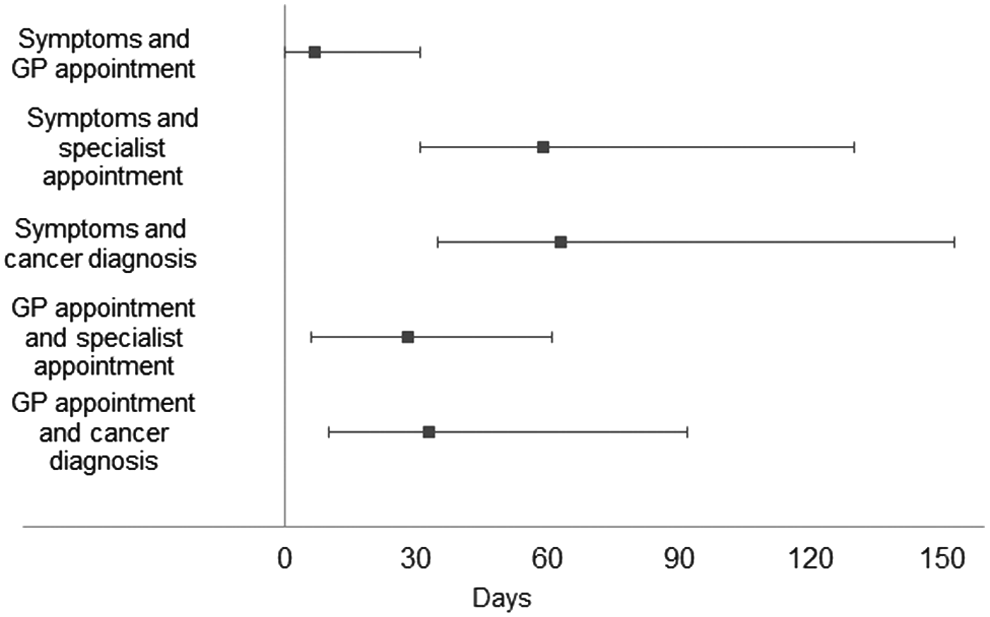
Patient-reported pathway times (median and IQR). IQR, interquartile range.
Discussion
In this feasibility pilot study, we have demonstrated that international multiprofessional research, including patients as direct data contributors in TYA with cancer, is feasible within our international collaborative network. Conducting such research without grant funding was difficult. Responses from primary care were the most difficult to obtain, but not impossible, and not uniformly obtained by country. The results observed for patient experience must be interpreted with caution given our pilot aims and sample size.
There were significant variations and barriers presented by regulatory aspects. Translation of study forms significantly delayed study implementation. Administrative burdens upon the study team and investigators varied across locations within Europe, despite local research teams being highly motivated to participate. Imbalances between available research resource and local governance requirements resulted in inequity in our ability to open the study in a timely manner, or to open it at all in some places. Explicit unified European positions on these issues for relatively low-risk questionnaire-based studies could substantially improve research productivity. We recommend that proportionate review systems for defined low-risk projects are considered internationally according to local systems. 35
Although our pilot study had limited sample size, the findings are broadly comparable with other studies. We found ∼40% of patients visited their GP at least twice before diagnosis. In comparison, a large U.K. primary care cohort study, in the 3 months before diagnosis, 42.9% of TYA with cancer consulted primary care ≥4 times versus 11.5% in age-matched patients without a cancer diagnosis. 27 Almost twice as many TYA visited their GP more than three times before diagnosis of cancer than is observed in older adults (38% vs. 20%). 28 We found that the median time from reporting symptoms to cancer diagnosis was 9 weeks. In comparison, a 2007 study 36 showed a median time from symptom onset to diagnosis of 9.5 weeks (range 2–191.5 weeks). We identified marked differences in the proportion of repeated visits reported by GPs and patients. A survey of 174 TYA patients in 2004 showed that 20% of patients waited several months before seeking help after experiencing symptoms and that 71% of TYAs also reported visiting their GP two to five times before being referred to a specialist. 37 Some of the reasons given for this delay included, being scared to seek help, ignoring symptoms, concerned or embarrassed about symptoms, not having time, concerns about not being taken seriously, and fear of bad news.36,37
Symptoms reported were distinct between primary care and patients, despite data collection being shortly after diagnosis. It is possible that primary care recorded only the most clinically worrying symptom. Pain was a common feature of primary care physicians' reported symptoms, although patients commonly reported painless lumps.
The range in times from onset of symptoms to diagnosis in our study is very wide, whereas the median times are reasonable clinically for the cancers being considered. This asymmetric and skewed distribution may indicate a sporadic not a systematic prolongation of the process. This is reflected in the recent “three-legged” approach to health service improvement in Denmark.38,39 The characteristics and risk factors associated with this could be examined in a larger study, focusing upon the cancers, where data most strongly indicate that a prolonged pathway is detrimental. 40 In the United Kingdom, campaigns designed to increase awareness of the signs and symptoms of TYA cancers have been implemented. 41
There are obvious limitations of this study; it was not intended as a comprehensively sampled inception cohort design, included recruitment only at selected centers with small sample size. Eligibility, only shortly after diagnosis, may have limited recruitment. The study clearly requires extension before firm conclusions can be reached. However, we met our main pilot study objectives; we demonstrated the feasibility of such studies, which cross traditional data-reporting approaches, including the collection of triangulated data. There are preliminary signals of possible differences in these patient pathways internationally, which merit confirmation as well as exploration of mechanisms in future work. The study also indicated some key methodological learning for more definitive future studies; patients reported a larger burden of symptoms than GPs. However, patient's symptoms were reported from a check list, whereas GPs reported symptoms through a free text field, and GP records may well only include key symptoms even when free text is available. The evolution in the perception of events over time is apparent, with patients reporting primary care consultations at the outset of their pathways, but their oncology specialists not identifying this from their records. Precise recording of the relation between the date of events and of data collection may be very important in conducting future larger-scale studies. The proportion reporting a shorter symptom duration was higher for patients than it was by GPs. This may be important when measuring this in future studies. Triangulating the responses from patients, primary care, and secondary care clinicians about how symptoms were investigated through health services through various emergency and elective providers, requires the development of a clear shared terminology.
The importance on international networking (as demonstrated by this study) is clear in driving and delivering such a study, and the ability of a network such as ENTYAC to increase our understanding and potentially reduce diagnostic delay is apparent. 42 Our group plan to take this learning forward in building multicenter European studies for TYA with cancer in this and other areas of enquiry.
It is interesting to note from the current literature the influence that the initial clinical impression or extent of “cancer suspicion” of the initially assessing GP has upon the subsequent pathway. This impression may be due to the presence of nonspecific symptoms (such as lump without pain) at that assessment. However, many cancers present without specific symptoms, particularly while of early stage, and this may be unduly influencing clinical behavior. 43 This is particularly relevant to TYA. As TYA have less experience of medical encounters and greater embarrassment when reporting symptoms, the proportion giving nonspecific descriptions may be increased.19,44 If this is coupled with a low clinical suspicion (driven by the epidemiology), long delays would then occur for cancers where nonspecific symptoms are reported.
In future, we propose to focus upon the experiences of TYA patients with very long times to diagnosis, specifically where time from symptoms to diagnosis appears to markedly influence clinical outcome, nonrhabdomyosarcoma soft tissue sarcoma, and advanced germ cell tumor. 41 Analyses by cancer type were not possible in our sample size, nor appropriate in a pilot design. Very long diagnostic pathways may be clinically important and costly to healthcare resources, but moreover are highly emotive for patients, carers, and clinicians, and may promote a clinical impression that all pathways are more prolonged than they generally are.
Footnotes
Acknowledgment
Information described in this article has received funding from the European Union's Seventh Framework Program (FP7/2007–2013) under the project ENCCA, grant agreement HEALTH-F2-2011-261474.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.