
Abstract
Purpose:
To estimate the risk for hospitalizations among survivors of Hodgkin lymphoma diagnosed in adolescence or young adulthood according to exposure to treatment with radiation therapy.
Methods:
Through the files of the Danish Cancer Registry, we identified 1684 five-year survivors of Hodgkin lymphoma, diagnosed at age 15–39 years during the period 1943–2004, and for whom information on radiation therapy was available in the Cancer Registry. Population-based comparisons were identified through the Danish Civil Registration System and matched to the survivors on year of birth and sex. Survivors of Hodgkin lymphoma and comparisons were linked to the Danish National Patient Register for information on hospitalizations. Standardized hospitalization rate ratios (RR) and absolute excess rates (AERs) were estimated for total number of hospitalizations and for hospitalizations for cardiovascular disease, cancer and several other disease groups.
Results:
Overall, survivors of Hodgkin lymphoma who received radiation therapy had higher risk (RR 2.0) and AER (AER 588) of hospitalization than survivors not treated with radiation therapy (RR 1.8; AER 399). Especially, the risk for cardiovascular disease and cancer was high among survivors who received radiation therapy (RR 2.8 and 3.6) compared with survivors who did not receive this type of treatment (RR 2.2 and 2.3).
Conclusion:
Survivors of adolescent and young adult Hodgkin lymphoma treated with radiation therapy had a higher risk of diseases requiring hospitalization than survivors not treated with radiation therapy. Irrespective of the type of treatment received, initiatives that prevent and minimize hospital-requiring late effects in survivors of Hodgkin lymphoma are needed.
Introduction
Radiation therapy has been used as treatment for Hodgkin lymphoma since the 1960s 1 ; fortunately, radiation therapy nowadays is given to the involved fields only whereas the extended fields used in the past caused radiation exposure to larger areas of healthy tissue. 2 Several recent studies have shown increased risk for cardiovascular disease among survivors of Hodgkin lymphoma.3–6 One of these studies was from the Netherlands and included 2524 survivors of Hodgkin lymphoma diagnosed before the age of 51 years. 6 The study showed that treatment with mediastinal radiation caused significantly increased risks for coronary heart disease, valvular heart disease, and congestive heart failure when compared with the general population. 6 Also, the risk for second cancer is known to be increased among survivors of Hodgkin lymphoma.7–9 A recent study from the Netherlands included 3905 survivors of Hodgkin lymphoma diagnosed at age 15–50 years. 8 After 19.1 years of follow-up, 1055 cancers were diagnosed in 908 survivors, which resulted in a significantly increased standardized incidence ratio of 4.6, when compared with the general population. 8 The authors conclude that a reduction in the radiation exposure of healthy organs and tissues would reduce the number of survivors who develop second cancer. 8
In the present study, we estimate the risks for a range of disease groups among survivors of Hodgkin lymphoma who were diagnosed in adolescence or young adulthood, focusing on the risk for cardiovascular disease and cancer and on the differences in risks between survivors who were treated with radiation therapy and survivors who did not receive radiation therapy.
Methods
From the records of the Danish Cancer Registry, 10 we identified 1768 five-year survivors of Hodgkin lymphoma diagnosed in adolescence or young adulthood (15–39 years of age at diagnosis) in the period 1943–2004. A comparison cohort consisting of 228,447 age- and sex-matched comparison subjects were identified from the Danish Civil Registration System. 11 The Hodgkin lymphoma cohort and the comparison cohort were linked to the records of the Danish Patient Register 12 for identification of hospitalizations for 145 defined disease categories, which was grouped in 14 main diagnostic groups. Details of the cohort and the full list of disease categories have been published previously. 13 Follow-up started 5 years after Hodgkin lymphoma diagnosis, or on a corresponding date for comparison subjects, or on January 1, 1977 at the earliest (start of the Danish Patient Register). Follow-up ended on the first date of the following: date of death, date of emigration, or end of study on December 31, 2010. Standardized hospitalization rate ratios (RR) were calculated as the observed hospitalization rate in the survivor cohort compared with the expected hospitalization rate (based on the number of hospitalizations in the comparison cohort). Absolute excess rates (AERs) were calculated as the hospitalization rate per 10,000 person-years in the survivor cohort minus the hospitalization rate in the comparison cohort.
Information on treatment with radiation therapy was available in the Danish Cancer Registry on a Yes/No level. In the cohort of 1768 Hodgkin lymphoma survivors, 879 (49.7%) were treated with radiation therapy and 805 (45.5%) were not treated with radiation therapy; we assume that this group of survivors were treated with chemotherapy only. Information on treatment with radiation therapy was missing for 84 survivors (4.8%) leaving 1684 survivors for inclusion in this study. Valid information on treatment with chemotherapy was not available in the Danish Cancer Register.
Results
We included 1684 five-year survivors of Hodgkin lymphoma diagnosed in adolescence or young adulthood (15–39 years of age) of whom 879 were treated with radiation therapy and 805 were not treated with radiation therapy. The mean follow-up period for survivors who received radiation therapy was 18.6 years (median 19.2 years, range 0–34 years), whereas survivors who did not received radiation therapy had a mean follow-up period of 13.0 years (median 11.8 years, range 0–34 years). We saw a difference in the overall standardized hospitalization RR for a first category-specific hospitalization between the survivors of Hodgkin lymphoma who were treated with radiation therapy (RR 2.0) and survivors who were not treated with radiotherapy (RR 1.8) (Table 1). As can be seen from Table 1, men had higher risk for hospitalizations than women; both in the “radiation” group and in the “no radiation” group. Considering age at cancer diagnosis, survivors diagnosed at age 15–29 years and treated with radiation therapy had higher risks for hospitalization (RR range 1.9–2.2) than those who did not received radiation therapy (RR range 1.4–1.9). For survivors who were older at their Hodgkin lymphoma diagnosis (30–39 years), the risk for hospitalization was comparable between the “radiation” group and the “no radiation” group (Table 1). For survivors diagnosed in the calendar period 1943–1989, we saw a higher risk for hospitalizations in the “radiation” group when compared with the “no radiation” group. For the most recent period (1990–2004) the “radiation” group had a slightly lower risk of hospitalizations than the “no radiation” group (Table 1).
Standardized Hospitalization Rate Ratio with 95% Confidence Intervals of Hospitalization Among 1684 Five-Year Survivors of Hodgkin Lymphoma According to Selected Characteristics
CI, confidence interval; HL, Hodgkin lymphoma; RR, rate ratios.
For attained ages 30–39 and 50–69 years, the “radiation” group had higher risks for hospitalization compared with the “no radiation” group, whereas for other attained ages survivors in the “no radiation” group had a higher risk than survivors in the “radiation” group; however, confidence intervals (CI) were overlapping (Table 1).
The overall higher risk estimates observed in survivors treated with radiotherapy were mainly due to higher RRs for hospitalization for cancer (3.6 in irradiated and 2.3 in nonirradiated survivors) and cardiovascular diseases (2.8 vs. 2.2) (Fig. 1). Table 2 gives the estimates for a selected set of cardiovascular diseases and cancers for which the RR was ≥4.0 in either the group treated with radiation therapy or that not treated with radiation therapy.
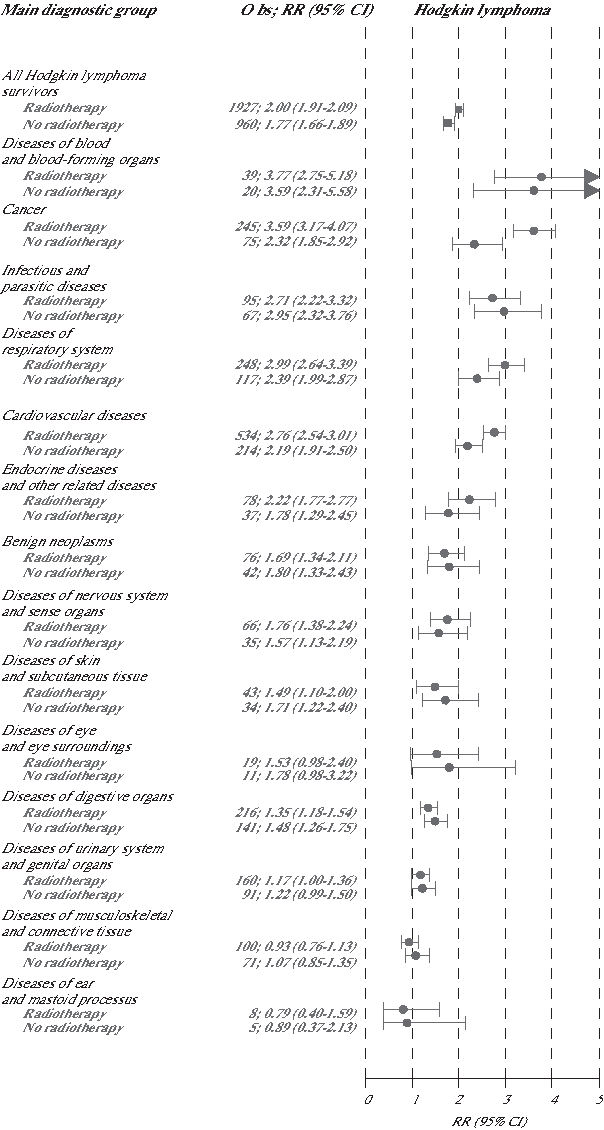
Forest plot showing the standardized hospitalization RRs with corresponding 95% CIs for each of the 14 main diagnostic groups. Risk estimates are given for survivors treated with radiotherapy and survivors not treated with radiotherapy. CIs, confidence intervals; Obs, observed number of hospitalizations; RR, rate ratio.
Standardized Hospitalization Rate Ratios and Absolute Excess Rates with 95% Confidence Intervals for Disease-Specific Hospitalizations Among 1684 Five-Year Survivors of Adolescent and Young Adult Hodgkin Lymphoma
Risk estimates are shown for all causes of hospitalization combined (Total), for all cardiovascular diseases combined, for all cancers combined, and for a selected set of cardiovascular diseases and cancers for which the relative risk was ≥4.0 in the “Radiation” group or in the “No radiation” group of survivors.
AER per 10,000 person-years.
Diseases of other endocrine glands: ICD-8: 251–255, 258; ICD-10: E15–E27, E30–E35.
AER, absolute excess rate.
Cardiovascular disease
The subgroup of Hodgkin lymphoma survivors who received radiation therapy had extraordinarily high RRs for hospitalization for aortic and mitral valve disorders, endocarditis, acute and chronic diseases of the pericardium, and heart failure, resulting in 135 hospitalizations, accounting for 25% of all 534 category-specific first hospitalizations for cardiovascular diseases (Table 2). The diseases were diagnosed mainly in subjects aged 40–69 years, with most excess cases seen in survivors in their 50s. Table 3 shows the risk estimates for cardiovascular diseases by age at diagnosis, calendar period and attained age. For the period 1943–1989 the “radiation” group had higher risk for hospitalization than the “no radiation” group. In the most recent period (1990–2004) the “no radiation” group had the highest risk. None of these risk estimates were significantly different between the “radiation” group and the “no radiation” group (Table 3).
Standardized Hospitalization Rate Ratios with 95% Confidence Intervals for Cardiovascular Disease and Cancer by Age at Hodgkin Lymphoma Diagnosis, Calendar Period of Diagnosis and Attained Age
HL, Hodgkin lymphoma.
Cancers
Cancers for which there was a high risk in the “radiation” group tended to be located within or close to the irradiated field, for example, the highest AER in this group of survivors was observed for cancer of the lung, bronchus, and trachea (AER, 20 per 10,000 person-years). For comparison the corresponding AER in the group of survivors who did not received radiation therapy was 4 per 10,000 person-years (Table 2). Table 3 shows the risk estimates for cancer by age at diagnosis, calendar period, and attained age. For survivors diagnosed in the period 1960–1974, we saw a significantly higher risk of hospitalizations for cancer in survivors who received radiation therapy compared with those who did not received radiation therapy. Also in the period 1975–2004 the risk for hospitalization for cancer was higher in survivors who were treated with radiation therapy, however, these differences were not significant (Table 3).
Five survivors of Hodgkin lymphoma were diagnosed with mesothelioma during follow-up. All five survivors were treated with radiation therapy and all mesotheliomas were located in the pleura, with a lag between the dates of diagnoses of Hodgkin lymphoma and mesothelioma of 15–35 years. Among survivors who were treated with radiation therapy the RR for mesothelioma was 21.4 (95% CI 8.6–53.3) and the AER was 2.9 (95% CI 0.2–5.6) per 10,000 person-years (Table 2).
The risk for leukemia was particularly high in the group not treated with radiation therapy (RR 9.5, 95% CI 4.7–19.1).
Discussion
In this study, we include information on treatment with radiation therapy among 1684 five-year survivors of Hodgkin lymphoma. When evaluating the overall risk estimates, survivors who received radiation therapy for treatment of Hodgkin lymphoma had higher risk for hospitalizations than survivors who did not received radiation therapy. We had no information on treatment with chemotherapy, but the slightly higher risk of hospitalizations among survivors who had no radiation therapy and who were treated in the most recent period (1990–2004) could be an indication of the late effects caused by treatment with chemotherapy. Our finding of high risk for leukemia in survivors of Hodgkin lymphoma not treated with radiation therapy might also be an indication of the toxic effects of chemotherapy.
Cardiovascular disease
In the group of survivors who received radiation therapy as part of their treatment, both the prevalence of and the relative risks for admission to hospital for cardiovascular diseases were particularly high, especially for acute and subacute endocarditis, valve disorders, and heart failure.
In a recent study in the Netherlands, 6 the risk for cardiovascular disease was studied in a cohort of 2524 five-year survivors of Hodgkin lymphoma diagnosed at age 51 years or younger, during the period 1965–1995. The analysis of outcome data, which were collected from medical records and general practitioners, showed four- to six-fold increases in the risks for coronary heart disease and heart failure in comparison with the general population. Hazard ratios for valvular heart disease and heart failure were 6.6 and 2.7, respectively, among survivors who had received radiotherapy as compared with those who had not. 6 This risk pattern is compatible with that seen in the present study, which shows a significantly increased risk for all but a few diagnostic categories of cardiovascular disease. This also corresponds to the results of a cross-sectional European multicenter study of 6039 survivors of Hodgkin lymphoma (median age at diagnosis, 30 years; median length of follow-up, 9 years), with registered information on primary treatment, who responded to a questionnaire during 2009–2010. 5 In this study, the mean radiation dose to the heart and the dose of anthracyclines were significant predictors of cardiovascular disease. 5
Cancer
The findings of an increased risk for cancer of the lung in survivors of Hodgkin lymphoma who received radiation therapy are in accordance with that of a recent study, which included 604 survivors of Hodgkin lymphoma. This study reports an increased risk for lung cancer among survivors of Hodgkin lymphoma who received radiation therapy doses higher than 42 Gy (hazard ratio 4.0; 95% CI, 1.1–11.6). 14
Mesothelioma
The association between asbestos minerals and malignant mesothelioma was first acknowledged in 1960 15 ; since then other exposures, for example, to certain metals and ionizing radiation have been associated to an increased risk for mesothelioma.16,17 In ∼80%–85% of cases of malignant mesothelioma an exposure to asbestos mineral fibers have been established, 18 which implies that a causal explanation is missing in the remaining 15%–20% of cases. These cases are likely caused by radiation; mainly radiation given for treatment of cancer but also exposure to radiation from thorium dioxide in the form of Thorotrast; a diagnostic X-ray contrast medium.
In this study, five cases of pleural mesothelioma occurred among survivors who had been treated with radiation therapy and the relative risk of mesothelioma in this cohort of Hodgkin lymphoma diagnosed in adolescence or young adulthood was 21.4. Among survivors who were not treated with radiation therapy, no cases of mesothelioma were observed. This observation indicates that treatment with radiation therapy cause a highly increased risk for mesothelioma, although the AER was rather small: 2.9 per 10,000 person-years.
In 2009, a long-term follow-up study of 2567 five-year survivors of Hodgkin lymphoma in the Netherlands revealed 13 cases of malignant mesothelioma of the pleura in the subgroup treated with radiotherapy, resulting in an RR of 29.5. 19 This finding and ours indicate that the occurrence of mesothelioma after radiation therapy to the chest is as common as cancers at other sites in the respiratory and gastrointestinal tracts.
Limitations
In this study, we have no information on the occurrence of relapse. This means that the increased risk for late effects observed in this study can be due to the treatment given for the first occurrence of Hodgkin lymphoma, but also potentially due to the often more intense treatment given for relapse. Also, it should be kept in mind that patient characteristics and severity of disease at diagnosis are determinants for the choice of treatment. Thus, if patients with a more advanced disease at diagnosis were more often treated with radiation therapy, the consequences of having had an advanced disease might contribute to the increased risk of hospitalization, independent of type of treatment. Further, it must be emphasized that survivors who were treated with radiation therapy in this study might also have received chemotherapy. This study included survivors of Hodgkin lymphoma diagnosed during a long period in which there has been major changes in the treatment of Hodgkin lymphoma. In this study, we had no information on the details of treatment and we were not able to consider the positive effects of modern radiation therapy.
Strengths
In this nationwide cohort of survivors of Hodgkin lymphoma diagnosed in adolescence and young adulthood, we had access to all hospital admissions since 1977 and were hereby able to estimate the risks for hospitalization stratified by treatment with radiation therapy.
Conclusion
Survivors of Hodgkin lymphoma diagnosed in adolescence and young adulthood are at increased risk for hospitalization for a range of diseases. Survivors treated with radiation therapy had higher risks; especially the risk for cardiovascular disease and cancer was higher among survivors treated with radiation therapy. Survivors of Hodgkin lymphoma and health professionals should pay attention to symptoms that might indicate a disease. Hereby, timely treatment could prevent progression of the disease and hospitalization might be avoided.
Footnotes
Acknowledgments
We would like to thank Andrea Bautz, Danish Cancer Society Research Center, for her through work with the programming and the analyses of the data used in this article. We acknowledge Nick Martinussen, Danish Cancer Society Research Center, for his development of the program for creation of the forest plots. K.R. received a postdoctoral grant for the period January 1, 2014 to December 31, 2016, from The Danish Council for Independent Research in Medical Science. The funder had no involvement in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the article.
Authors' Contributions
K.R. and J.H.O. designed the study, collected the data, analyzed the data, and interpreted the results. K.R. drafted the article. K.R. is guarantor.
Ethical Approval
The study protocol was approved by the Danish Data Protection Agency.