
Abstract
Purpose:
Current guidelines recommend screening at-risk childhood cancer survivors for ovarian dysfunction using follicle-stimulating hormone (FSH). However, FSH identifies diminished ovarian reserve (DOR), a component of ovarian dysfunction, in the later stages when fertility preservation is less likely to succeed. This analysis evaluates the utility of anti-Mullerian hormone (AMH) for the assessment of DOR in adolescent and young adult (AYA)-aged survivors of childhood cancer.
Methods:
A retrospective chart review of 13- to 21-year-old female survivors who received gonadotoxic therapy and were ≥2 years off therapy was performed. Gonadotoxic treatments were categorized as low, moderate, or high risk for future infertility. Patients with AMH below the assay's age-specific normal range were identified and stratified by FSH values (normal ≤12 mIU/mL). Prevalence of low AMH and AMH-FSH subgroups was calculated and risk factors were evaluated using logistic regression.
Results:
AMH was measured in 190 survivors who received gonadotoxic treatment; of them, 35.3% had low AMH. Among survivors who received <30 Gy cranial radiation and were not on hormone therapy (n = 141), 18.4% had normal FSH with low AMH. Stratified by future infertility risk, 10.6% of low-risk, 38.1% of moderate-risk, and 25.7% of high-risk survivors had normal FSH with low AMH (p < 0.01). Within the low-risk group, normal FSH with low AMH was significantly associated with older age at diagnosis (p = 0.02).
Conclusion:
Nearly 20% of AYA-aged at-risk survivors had low AMH and normal FSH. DOR in these patients would have been missed in standard recommended surveillance practices.
Introduction
Many childhood cancer survivors are at risk for ovarian dysfunction because of the cancer treatments they receive.1–6 One component of ovarian dysfunction is diminished ovarian reserve (DOR), a subclinical reduction in the primordial follicle pool that may eventually progress to primary ovarian insufficiency (POI). POI can manifest as pubertal delay, hypergonadotropic hypogonadism with estrogen deficiency, and infertility. 6 Cancer survivors report being concerned about their reproductive health and seek to be informed about potential infertility issues.7–11 Therefore, it is important that effective screening for DOR begins in the adolescent years.
The Children's Oncology Group Long-Term Follow-Up (COG LTFU) Guidelines v4.0 12 recommend screening female cancer survivors at risk for ovarian dysfunction with follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol beginning at age 13 years. However, FSH can be difficult to interpret in young survivors because it is low in prepubertal patients whose hypothalamic–pituitary–ovarian (HPO) axis is not yet activated13,14 and suppressed in patients who are on hormone replacement therapy (HRT) 15 or in those with central hypogonadism after high-dose cranial radiation.16,17 Furthermore, FSH is a late indicator of DOR and once elevated into the menopausal range, fertility preservation therapy is unlikely to be successful. 18
Given the limitations of FSH, adolescent and young adult (AYA)-aged survivors may benefit from the addition of anti-Mullerian hormone (AMH) to the current screening for DOR. Antral follicle count (AFC) measured by vaginal ultrasound is a standard measure of ovarian reserve. Studies show that serum AMH levels correlate well with the AFC determined by ultrasound or histology. 19 AMH is now commonly used by reproductive endocrinologists to evaluate adult women with infertility.20,21 Furthermore, studies involving adult survivors of childhood cancer suggest that low AMH levels identify DOR before elevated FSH levels are detected.22,23 However, AMH testing is not currently part of the evidence-based COG LTFU guidelines because of limited literature on its use as an ovarian reserve marker in AYA-aged survivors.
The purpose of this study was to assess ovarian reserve using AMH in a large cohort of AYA-aged survivors and to identify associated demographic and treatment risk factors for low AMH. We also identified survivors with normal FSH but low AMH levels because this subgroup would not have been detected as having DOR by current FSH-based screening guidelines.
Methods
A retrospective study of female survivors of childhood cancer, who were seen in the multidisciplinary Cancer Survivor Program at Children's Healthcare of Atlanta (CHOA) between January 1, 2014, and August 31, 2016, was conducted. The study included patients who were 13 to 21 years old at their clinic visit. Survivors had been diagnosed with cancer at <20 years and were ≥2 years off treatment, which is the time point at which LTFU in survivor clinic begins at this hospital. Patients with a history of central nervous system (CNS) tumors were not included in this study as they are followed in a different LTFU clinic at the hospital. This study was reviewed and approved by the CHOA institutional review board.
Demographics, current HRT use, cancer diagnoses, and treatment details (cumulative dose of alkylating and heavy metal chemotherapies, radiation with potential ovarian exposure using radiation fields defined by the COG LTFU guidelines, 12 history of oophorectomy, cranial radiation doses, and hematopoietic stem cell transplant [HSCT] history) were abstracted from the medical record. Those who underwent a bilateral oophorectomy were excluded. No patients underwent ovarian tissue removal for fertility preservation. Study data were collected and managed using the Research Electronic Data Capture (REDCap) application. 24
AMH and FSH concentrations
Patients at risk for ovarian dysfunction were screened with FSH, LH, and estradiol beginning at age 13. In 2013, based on recommendations from our institutional reproductive medicine service, our survivor program began to incorporate AMH into the surveillance for DOR in at-risk survivors. This practice was routine by January 2014. For each patient, the first available AMH and FSH measurements during the study period were abstracted. As the screening was carried out as part of routine clinical care, serum samples were sent to Quest Diagnostics™, LabCorp®, ARUP laboratories, or our institutional laboratory for analysis based on the preference of the health insurance provider. Each AMH result was interpreted using the assay's age-specific reference range at the time of the blood draw. 25 Patients were classified as having normal AMH or low AMH (below the assay's age-specific reference range). AMH levels below the detectable range were also noted.
Among patients with FSH and AMH levels measured simultaneously, FSH levels were categorized as normal (≤12 mIU/mL), intermediate (>12 mIU/mL and <40 mIU/mL), or menopausal (≥40 mIU/mL). Patients who were on HRT at the time of surveillance and/or received ≥30 Gy cranial radiation were excluded from the FSH analyses because these values would not be interpretable.
Statistical analysis
The proportion of survivors seen in clinic who received gonadotoxic treatments was determined. At-risk survivors screened with AMH were compared with those who were not screened using chi-square and t-tests. Age at diagnosis was dichotomized at 11 years. As patients were not screened until age 13, patients diagnosed at <11 years had to age into screening, whereas those diagnosed at ≥11 years could be screened as soon as they reached 2 years off therapy. Cyclophosphamide equivalent doses (CEDs) were calculated for patients who received alkylating agents using methods developed by Green et al. to allow comparisons between different alkylating agents. 26 CEDs were categorized as none, low dose (1–7.49 g/m 2 ), moderate dose (7.5–14.9 g/m 2 ), and high dose (≥15 g/m 2 ).
Patients were categorized into treatment groups based on their risk for future infertility. Risk groups were determined by expert consensus of the pediatric initiative network (PIN) of the Oncofertility Consortium in 2015 (unpublished; permission obtained). The PIN developed this risk stratification system to help identify survivors at high risk for future infertility who might benefit from experimental ovarian tissue cryopreservation as a means of fertility preservation. Patients in this study were assigned to the PIN risk groups based on their highest risk exposure. Patients were considered high risk if they received high CED, an HSCT with any CED, ovarian radiation exposure (>15 Gy prepubertal and >10 Gy pubertal), total body irradiation (TBI, any dose), and cranial radiation ≥30 Gy; moderate risk if they received moderate CED, ovarian radiation exposure (10–15 Gy prepubertal and 5–10 Gy pubertal); and low risk if they received low CED, heavy metal therapy (any dose), radiation with ovarian exposure (<10 Gy prepubertal and <5 Gy pubertal), and/or a unilateral oophorectomy.
To better understand the association of each type of exposure with low AMH, patients were also analyzed by the most gonadotoxic therapy received to show differences by treatment within these risk categories.
The proportion of patients with normal and low (low but detectable and undetectable) AMH was calculated. To determine whether demographic and treatment characteristics were associated with low AMH, those with low AMH were compared with those with normal AMH using univariate logistic regression and two multivariate logistic regressions, one with interaction between age at diagnosis and future infertility risk group and one with no interaction.
Cross-tabulation of AMH categories with FSH levels was performed. Multinomial logistic regression was performed to compare those with low AMH/normal FSH and low AMH/menopausal FSH with those with normal AMH/normal FSH by age at diagnosis and future infertility risk group controlling for race/ethnicity. Patients with intermediate FSH levels were not included in the multinomial logistic regression because of sample size (n = 3). All analyses were conducted using SAS® version 9.4 (SAS Institute, Cary, NC) with p < 0.05 considered statistically significant and odds ratios (OR) with 95% confidence intervals (CI) reported.
Results
The cohort comprised 263 cancer survivors with 89.7% (236/263) who received gonadotoxic treatment. Three survivors had bilateral oophorectomy and were excluded. There were 43 survivors who did not have their AMH measured during the study timeframe, leaving 190 (80.5%) of the at-risk survivors who were screened with AMH and included in this analysis. The majority of survivors who were screened were white/non-Hispanic (57.9%) with a mean age of diagnosis of 8.0 years (standard deviation [SD]: 5.0 years) and age at screening of 16.7 years (SD: 2.3 years). There were no differences in screening status by race/ethnicity, age at cancer diagnosis, age at clinic visit, or current HRT use. Survivors who were screened with AMH were more likely to be classified as having high future infertility risk (Table 1).
Demographic and Treatment Characteristics of AYA-Aged Female Survivors of Childhood Cancer Who Were at Risk for Ovarian Dysfunction
CED = cyclophosphamide equivalent dose (Low dose = 1–7.49 g/m 2 ; moderate dose = 7.5–14.9 g/m 2 ; high dose ≥15 g/m 2 ).
p-value comparing female survivors screened versus those who were not screened with AMH. p-values in bold are statistically significant.
Excluded from analysis.
Based on the consensus of the PIN–Oncofertility Consortium for risk for future infertility (unpublished).
AYA, adolescent and young adult; CED, cyclophosphamide equivalent dose; HRT, hormone replacement therapy; HSCT, hematopoietic stem cell transplant; PIN, pediatric initiative network; SD, standard deviation.
Overall, 35% of at-risk survivors had low AMH, of which, 50% had undetectable AMH levels (Table 2). The distribution of AMH categories did not vary by laboratory assay (data not given). Those who received moderate or high CED (the latter with or without ovarian radiation), ovarian radiation alone, or underwent an HSCT were all significantly more likely to have low AMH than those who only received low CED (p < 0.05). There was no difference in the proportion of patients with low AMH among those who received heavy metals only or low CED with ovarian radiation versus low CED. When controlling for age at diagnosis and race/ethnicity, survivors in the moderate and high future infertility risk groups were more likely to have low AMH than those in the low-risk group (OR: 5.4, 95% CI: 1.7–17.2; OR: 32.2, 95% CI: 12.3–86.2, respectively).
Low Versus Normal Anti-Mullerian Hormone in AYA-Aged Survivors of Childhood Cancer Who are at Risk for Ovarian Dysfunction
CED = cyclophosphamide equivalent dose (Low dose = 1–7.49 g/m 2 ; moderate dose = 7.5–14.9 g/m 2 ; high dose ≥15 g/m 2 ).
Grey shades represent variables that were not included in the regression analysis.
OR of low AMH compared with normal AMH. ORs in bold are statistically significant, p < 0.05.
May have also received heavy metal chemotherapy.
4/24 had unilateral oophorectomy.
5/6 had radiation dose <15 Gy.
5/9 had radiation dose <15 Gy.
8/9 had radiation dose ≥15 Gy.
Allogenic transplant n = 19, Autologous transplant n = 12.
Based on the consensus of the PIN–Oncofertility Consortium for risk for future infertility (unpublished).
aOR, adjusted odds ratio; CI, confidence interval.
Patients diagnosed at ≥11 years of age compared with those diagnosed at <11 years were older at screening [mean (SD): 18.4 (1.7) years vs. 15.9 (2.1) years; p < 0.001] and were more recently off therapy [3.6 (1.5) years vs. 9.0 (3.8) years; p < 0.001]. As there was also a significant association between age at diagnosis and future infertility risk group (p = 0.008), an interaction logistic model was used to determine the odds of low AMH controlling for race/ethnicity (Table 3). Within each age at diagnosis strata, the odds of low AMH in survivors with high future infertility risk were higher than those with low risk. Within the future infertility risk groups, there was only a significant difference in the odds of low AMH by age at diagnosis among those with low future infertility risk. Within this group, survivors who were diagnosed with cancer at ≥11 years were 5.4 (95% CI: 1.5–18.5) times as likely to have low AMH compared with those diagnosed at <11 years.
Interaction of Future Infertility Risk Group and Age at Diagnosis on Low Anti-Mullerian Hormone in AYA-Aged Survivors of Childhood Cancer
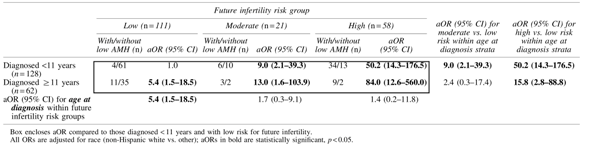
Box encloses aOR compared to those diagnosed < 11 years and with low risk for future infertility.
All ORs are adjusted for race (non-Hispanic white vs. other); aORs in bold are statistically significant, p < 0.05.
Among those with simultaneous FSH and AMH levels who received <30 Gy cranial radiation and were not on HRT at their clinic visit (n = 144), there were three survivors (2.1%) with intermediate FSH levels (19.7, 37.9, and 27.8 mIU/mL) and low AMH. In the remaining 141 survivors, 94 (66.7%) had normal AMH and FSH, 26 (18.4%) had low AMH with normal FSH, and 21 (14.9%) had low AMH with menopausal FSH (Fig. 1A). Only survivors with high risk for future infertility were significantly more likely to have low AMH with menopausal FSH than those with low risk (51.4% vs. 2.4% p < 0.001, controlling for race/ethnicity). However, both those with moderate and high future infertility risk were significantly more likely than the survivors with low risk to have low AMH with normal FSH (38.1% and 25.7%, respectively, vs. 10.6%; p < 0.01, controlling for race/ethnicity). When the future infertility risk groups were stratified by age at diagnosis, there was a significant difference in the proportion of survivors who had low AMH with normal FSH by age at diagnosis in those with low risk (p = 0.02). This association with age at diagnosis was not observed in the other risk groups (Fig. 1B).
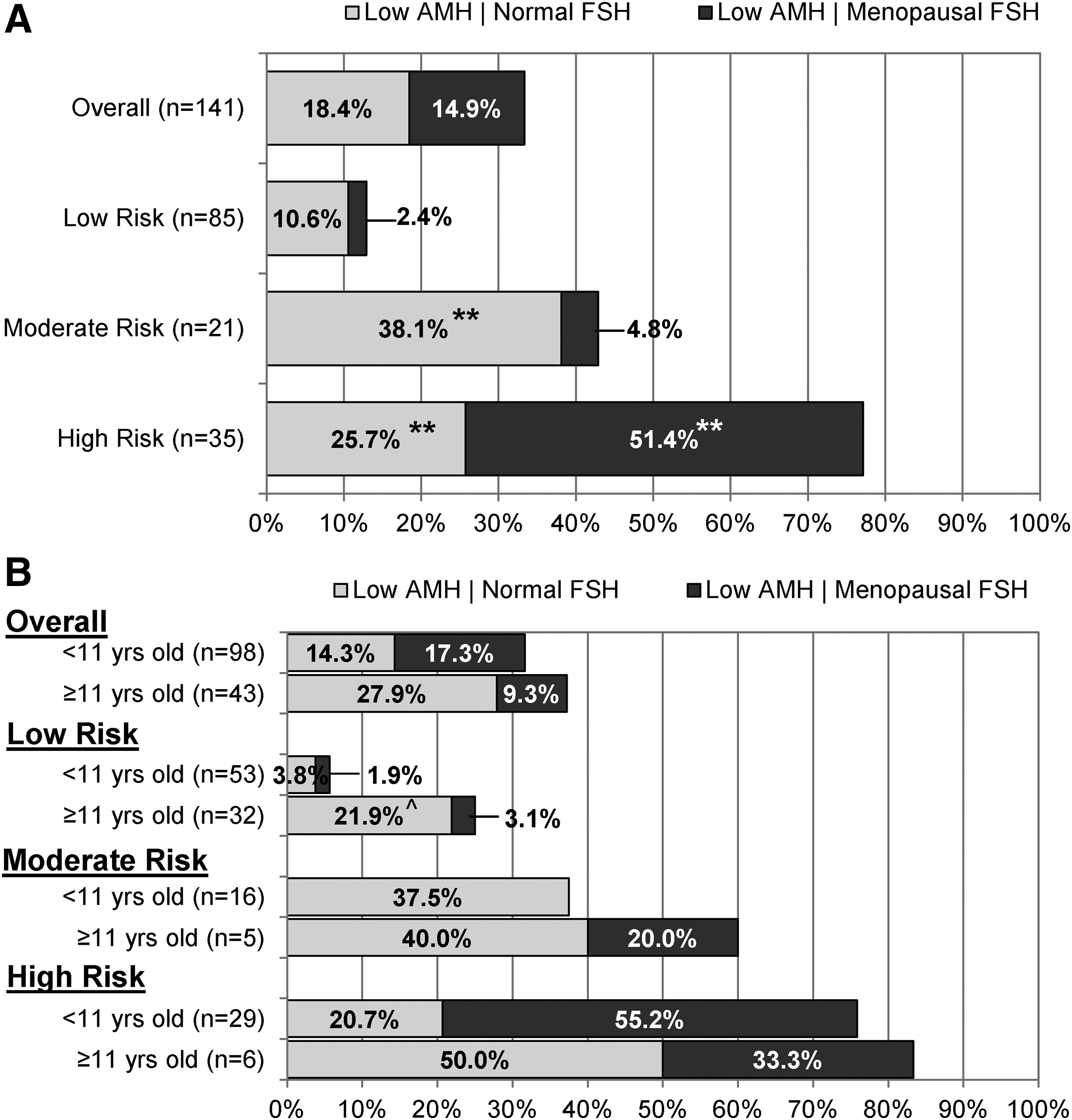
Distribution of low AMH with normal FSH versus low AMH with menopausal FSH stratified by
Discussion
This study showed that the majority of AYA-aged survivors of childhood cancer followed in a multidisciplinary survivor clinic received treatment that places them at risk for DOR; however, current FSH-based screening guidelines for ovarian dysfunction after cancer treatment would not have detected DOR in approximately one-fifth of the survivors. When stratified by future infertility risk categories, 11% of low-risk, 38% of moderate-risk, and 26% of high-risk survivors had DOR that would have been missed by screening only with FSH. This unique population may have normal menses and fertility at the time of screening but should be informed about the possibility of a shorter reproductive window. When appropriate, infertility counseling and fertility preservation should be offered to these patients.
In adult women, FSH alone is a poor screening tool for early DOR because of its abrupt change from normal to menopausal levels.27,28 In our study, we considered FSH levels ≤12 mIU/mL to be normal and ≥40 mIU/mL to be menopausal. Only three (2%) survivors at risk for ovarian dysfunction had intermediate FSH values, supporting its lack of utility as a signal of impending POI. In addition, FSH is uninformative in female survivors who are prepubertal, on HRT, or who have hypothalamic/pituitary damage.13,14,16,17,29 Of our study participants with simultaneous AMH and FSH levels, nearly one-quarter were excluded from FSH analysis because of HRT use, unknown HRT status, or previous cranial radiation exposure. Furthermore, FSH should be measured on days 2 to 4 of the menstrual cycle as its production fluctuates throughout the cycle. 21 Typically, in survivor care, labs are drawn at the time of the clinic appointment. It would be impractical to schedule clinics on a specific day of the menstrual cycle. For these reasons, the utility of FSH as a marker of ovarian reserve is limited in the AYA-aged cancer survivor population.
AMH may be a more useful biomarker of ovarian reserve in female childhood cancer survivors. AMH levels are not dependent on hypothalamus/pituitary function and are thus unaffected by cranial radiation or CNS surgery. Unlike FSH levels that change abruptly at menopause, the trajectory of AMH levels fluctuates from birth to 12 years of age but then increases steadily to a peak at 25 years with a subsequent gradual decline until menopause. 30 This emphasizes the importance of interpreting AMH using age-stratified normal ranges as was performed in this study. Although some studies detected variation in AMH levels throughout the menstrual cycle,31–33 others did not.34–36 In addition, the reported AMH fluctuations are less than those seen in FSH levels, suggesting that AMH can be interpreted on random days of the menstrual cycle. 37
There are conflicting reports on the effect of exogenous hormones on AMH levels. In one study of 123 healthy AYA women followed for a median of 2 years, AMH levels were 55% lower in those taking combined hormonal contraceptives than those who were not. 38 Conversely, several studies have found no relationship between exogenous hormone use and AMH levels.29,39,40 Regardless, AMH is not completely suppressed by exogenous hormone use, making it a more valid marker of ovarian reserve than FSH in AYA-aged survivors on hormone therapy.
Previous studies of smaller cohorts of AYA-aged survivors have supported AMH as a possible earlier indicator of ovarian dysfunction compared with FSH. In a study by Krawczuk-Rybak et al., 52% of 83 AYA-aged survivors who received gonadotoxic therapy were shown to have low AMH but normal FSH levels. 41 Lunsford et al. found that 28% of 53 pediatric cancer survivors aged 9 to 25 years had low AMH (defined by a fixed, non-age-based AMH level <1 ng/mL) with a normal FSH. 42 In a study of 49 adolescent cancer survivors by Elchuri et al., 18% had low AMH with nonmenopausal FSH. In the Elchuri study, AMH levels less than the fifth percentile for age were considered to be low. 43 We used the age-specific normal reference ranges of the assays to define normal and low AMH levels. In our large cohort of 141 young, at-risk survivors, almost 20% had normal FSH but low AMH.
Interestingly 50% of our survivors with low AMH actually had undetectable levels. This subgroup is of clinical importance because counseling about potential future infertility may be different when AMH levels are so low.
In the evaluation of adult women with infertility, low AMH levels are considered to be indicative of DOR and predictive of suboptimal response to ovarian stimulation for oocyte harvest.44,45 Low AMH levels have also been associated with earlier onset of menopause.46–48 Although studies of healthy adult women49–51 and adult female cancer survivors52,53 who are actively trying to conceive naturally have shown low AMH levels alone do not predict infertility, there have been no long-term studies to determine the relationship between low AMH during adolescence with future infertility as an adult.
Although this study evaluated a large population of AYA-aged cancer survivors, it is not without limitations. Although >75% of eligible childhood cancer survivors are followed in the survivor program, data on survivors who failed to enter the program are not available. Thus our study population may not be representative of the general childhood cancer survivor population. In addition, per current guidelines, only at-risk survivors are screened for ovarian dysfunction. As a result, there was no comparison group of survivors who did not receive gonadotoxic treatment. Furthermore, as AMH and FSH levels were not checked before cancer treatment, we do not know the baseline ovarian reserve of these cancer survivors, although we assume it would be similar to the general population. There may be cancer survivors with delayed puberty who have normal FSH levels during the study period but who may develop menopausal FSH levels with activation of their HPO axis in the future. It is therefore possible that we underestimated the prevalence of menopausal FSH in our study population. Finally, subgroups of patients with low AMH stratified by demographic and treatment characteristics were small, thereby limiting the power to detect statistically meaningful differences between the subgroups.
In conclusion, this study was a critical first step in demonstrating the utility of combined AMH and FSH screening over FSH-only screening for the detection of DOR in AYA-aged survivors of childhood cancer. Consideration should be given to include AMH in surveillance guidelines. Longitudinal studies are needed to assess the rate of decline of ovarian reserve after cancer treatment and whether low AMH levels in adolescence predict fertility rates, pregnancy outcomes, and age of menopause in adult-aged survivors of childhood cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.