
Abstract
Purpose:
Adolescents and young adults (AYAs) with cancer need self-management strategies to cope with multiple symptoms. Self-efficacy, self-regulation, and negotiated collaboration are key theoretical components of the self-management process and have not been fully explored with AYAs with cancer. This study examined the effects of a heuristic symptom assessment tool on AYAs' self-efficacy for symptom management, AYAs' self-regulation abilities related to their symptoms, and communication with their providers about symptoms.
Methods:
AYAs (15–29 years of age) receiving chemotherapy used the Computerized Symptom Capture Assessment Tool (C-SCAT) to illustrate their symptom experience and discuss their symptoms with providers during two clinic visits. Participants completed the PROMIS Self-efficacy for Managing Symptoms Scale, a measure of satisfaction with provider communication, and a short interview about self-regulation and communication behaviors at baseline and after each provider visit.
Results:
Eighty-five AYAs who used the C-SCAT showed improved self-efficacy for managing symptoms. Qualitative data suggest that the C-SCAT was useful for enhancing a number of AYAs' self-regulation abilities related to symptom management, such as awareness and recall of symptoms, how symptoms were related, and how they planned to talk about their symptoms to providers. AYAs reported C-SCAT facilitated communication with providers about symptoms and symptom management because it was a visual prompt showing priority and related symptoms.
Conclusions:
Because AYAs continue to experience multiple distressing symptoms, symptom self-management remains an important area for practice and research. Use of heuristic tools, such as the C-SCAT, may help AYAs more effectively self-manage their symptoms for better health outcomes.
Introduction
I
Several frameworks have been developed to advance the science of self-management in individuals with chronic illness, including cancer.4,5 Although the frameworks vary in specific components, most view self-management as a process with outcomes related to health behaviors, health status, and costs. While individual, family, and environmental factors influence the process, mechanisms that drive desired self-management behaviors include self-efficacy (confidence to carry out a behavior), self-regulation (activities related to self-monitoring, goal-setting, and decision-making), motivation, and/or patient activation (being engaged in managing one's health).4,6
Few studies have explored the self-management process in AYAs with cancer. A systematic review examined self-efficacy for disease management in AYA cancer survivors and concluded that higher self-efficacy was associated with greater social support, AYAs' ability to talk about cancer, and positive health beliefs. Higher self-efficacy in AYAs predicted positive health behaviors and engagement in treatment, while lower self-efficacy was associated with a poorer health status. 7 Linder et al. identified multiple self-management strategies used by AYAs to manage chemotherapy-related symptoms, including medication management, sleep and rest, physical activity strategies, eating strategies, and psychosocial/relational strategies. 8 In a study of facilitators and barriers to self-management following stem cell transplant, social support and communication with the healthcare team were identified as facilitators to improve AYAs' self-management behaviors. 9 “Connectedness” with providers and a strong patient-provider alliance have been associated with AYAs' treatment adherence and psychosocial adjustments.10–13
This study was guided by the Individual and Family Self-Management Theory (IFSMT), which includes three dimensions: context, process, and outcomes (Fig. 1).14–17 The contextual dimension consists of characteristics specific to the individual, family, and environment, which can be risk or protective factors that influence self-management. The process dimension refers to knowledge, beliefs, self-efficacy, self-regulation skills and abilities, and social facilitation (e.g., social influences, support, and negotiated collaboration). Proximal and distal outcomes include self-management behaviors, cost, quality of life, and health status. A key assumption of the IFSMT is that the primary responsibility for self-management lies with the individual and family. 5
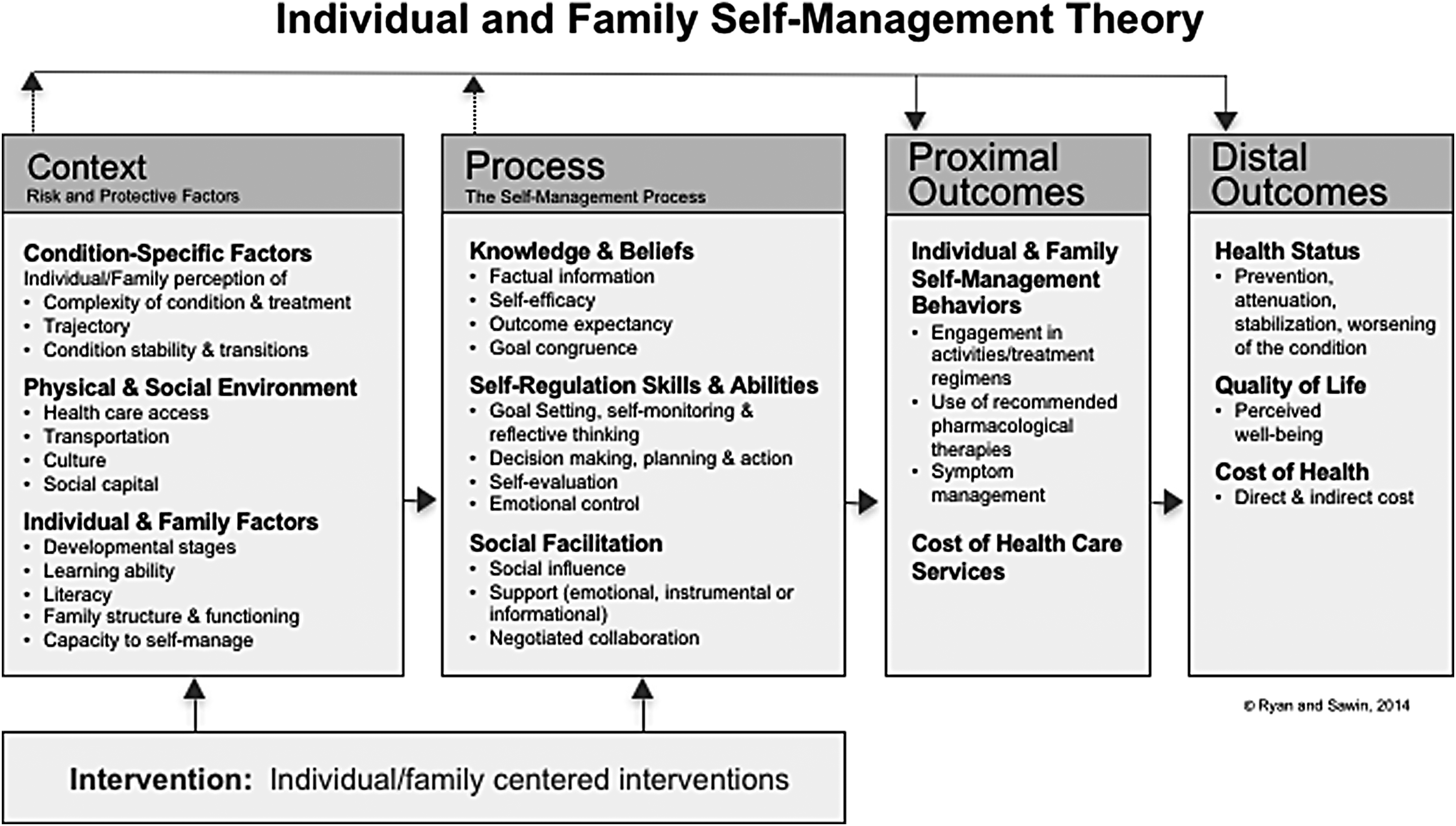
The Individual and Family Self-Management Theory. Used with permission from Ryan and Sawin, 2014. 17
This study sought to generate evidence about constructs integral to the process of self-management in AYAs related to cancer symptom management. The purpose of the study was to examine the effects of a heuristic symptom assessment tool, the Computerized Symptom Capture Assessment Tool (C-SCAT), on AYAs' self-efficacy for symptom management, their self-regulation abilities related to symptoms, and negotiated collaboration, as operationalized by AYAs' perceptions of communication with their providers about symptoms.
Methods
Study design
The study used a single-group longitudinal mixed methods design with data collection at the time of enrollment (baseline) followed by the use of C-SCAT and data collection during each of two post-baseline visits (visit 1 and 2) associated with chemotherapy administration. The time interval between most visits ranged from 1 to 4 weeks.
Setting and sample
Eligible participants were AYAs 15–29 years of age receiving myelosuppressive chemotherapy for any diagnosis of cancer at five academic medical centers in the USA. Narrower than that proposed by NCI, this age range captures adolescents and “emerging adults” who are more homogeneous in qualities of character.18,19 All sites treated AYAs with cancer and represented the Southwest, Intermountain West, Midwest, and Southeast. Inclusion criteria were as follows: (1) completion of at least 1 month of chemotherapy with at least two additional treatments anticipated, (2) physical and cognitive capacity to complete study procedures, and (3) ability to speak and read English.
Procedures
Following institutional review board approvals, the research team at each site screened for eligible patients. Written parental permission followed by written patient assent was obtained for those 15–17 years of age, and written informed consent was obtained for AYAs 18 years of age and older. Baseline measures of self-efficacy for symptom management and patient-provider communication were collected at the time of enrollment. At the next two scheduled visits for chemotherapy (visits 1 and 2) and before meeting with their provider, AYAs completed the C-SCAT and received a copy of the graphical image they created to use during the visit to discuss their symptom experience with their provider. Immediately after each provider visit, AYAs completed measures of self-efficacy and patient-provider communication and a brief in-person interview. All participants received a gift card at the completion of each provider visit. Intervention fidelity across sites was addressed by establishing standard operating procedures (SOP), training research team members to the SOP, and holding regular meetings to discuss any deviations across study sites.
Instruments
Participants self-reported their age, gender, race/ethnicity, and family/household structure. The medical record was reviewed for details about their cancer diagnosis, treatment protocol, and any co-morbid conditions.
(1) The Computerized Symptom Capture Tool (C-SCAT) is an investigator-developed application based on symptom cluster heuristics delivered using an iPad. 20 The C-SCAT guides the user to create a graphical image of his/her symptom experience. AYAs identify symptoms experienced during the past 24 hours from a menu, and then identify temporal and causal relationships between symptoms and groups of symptoms that occur together (symptom clusters). Finally, they name their symptom clusters and identify priority symptoms and a priority symptom cluster. Data generated from the C-SCAT are encrypted and transmitted to an HIPAA-compliant, password-protected Amazon Simple Storage Service account. The final image can be downloaded for review with a healthcare provider. The C-SCAT demonstrated initial feasibility and acceptability in AYAs with cancer. 21
(2) The PROMIS Self Efficacy for Managing Symptoms Scale (PROMIS S-E) is a 28-item scale for use with individuals with chronic conditions. Items assess the person's level of confidence to manage symptoms, including managing symptoms in different settings and keeping symptoms from interfering with daily activities. 22 Response options on a 5-point Likert scale range from “I am not confident at all” to “I am very confident.” Scores are summed across items, and higher scores indicate greater self-efficacy. Although the scale was validated in adults, the items are relevant for adolescents 15 years of age and older. 23 The Cronbach's alpha for the scale at baseline was 0.94.
(3) The Patient-Provider Communication Scale (PPCS) includes four investigator-developed items addressing the AYAs' perceptions of the quality of patient-provider communication about his/her symptom experience. Items address providers' openness, sensitivity, and care. Responses are measured on a 5-point Likert scale and range from “not at all” to “very much.” These items were derived from research addressing “connectedness” between AYAs with cancer and their providers. 10 The Cronbach's alpha for the new scale at baseline was 0.78.
(4) During a semistructured interview, AYAs responded to three questions that assessed how using the C-SCAT impacted self-regulation behaviors, such as self-monitoring, reflective thinking, and decision-making, as well as communication with providers.14,24–26 Questions addressed how using the C-SCAT helped the AYA (1) make sense of his/her symptoms; (2) manage his/her symptoms; and (3) discuss his/her symptoms with providers.
Data analysis
Descriptive statistics were computed for the demographic and cancer-specific variables. The PROMIS S-E and PPCS were scored, and a mean imputation was used for missing data. Less than 5% of participant responses were missing 1 or more items. All data were examined graphically to determine distributional properties. The C-SCAT images and associated text files were reviewed to summarize symptoms and priority symptoms reported by the AYAs.
Mixed-effects models examined the effects of the C-SCAT on perceived self-efficacy (PROMIS S-E) and PPCS over time. Using a backward elimination model-building approach, a mixed-effects linear model was fit to determine the best subset of predictors for the PROMIS S-E and PPCS, beginning with a base model that represented the design of data collection. Fixed effects included site, visit (baseline, visit 1 and visit 2), and site by visit interaction, and a random effect for study participant. Next, potential cofactors of interest (age, gender, and months since diagnosis) were added to the base model, and cofactors with a p-value >0.2 were then sequentially eliminated from the model. All models were checked for multicollinearity. Due to the pilot nature of the study, no adjustment for multiplicity was used, with the type 1 error set at 0.05.
Data from the interviews were analyzed using qualitative content analysis procedures to identify categories related to self-regulation abilities and patient-provider communication. 27 Audio files were transcribed and organized by question and by visit. Participants' answers were subdivided to reflect separate meanings. Two researchers worked together to create categories and subcategories of recurring meanings that reflected how the C-SCAT affected the AYAs' self-regulation of symptoms and communication with providers. The research team addressed discrepancies and confirmed the final analysis.
Results
Eighty-eight AYAs enrolled in the study and completed baseline data, and 85 AYAs had post-baseline data (visit 1 or visit 2 or both). Two AYAs withdrew after completing baseline data, and another did not report symptoms at either visit 1 or 2. Eighty-one completed surveys at visit 1 and 79 at visit 2. The majority of AYAs were male (54%) and white (72%). The mean age was 20.9 years (SD = 4.92). Table 1 lists participant characteristics by site.
PCH, Primary Children's Hospital, Salt Lake City, UT; CHLA, Children's Hospital of Los Angeles, Los Angeles, CA; Children's Mercy Hospital, Kansas City, KA; FH, Froedtert Hospital, Milwaukee, WI; VCUHS, Virginia Commonwealth University Health System, Richmond, VA; CML, chronic myeloid leukemia; ALL, acute lymphoblastic leukemia; APL, acute promyclocytic leukemia; AML, acute myelogenous leukemia.
Eighty-five participants reported symptoms using the C-SCAT. Eighty-three participants reported a mean of 5.6 symptoms at visit 1 (median = 5; range 1–15). Seventy-nine participants reported a mean of 4.8 symptoms at visit 2 (median = 4; range 1–18). All 32 symptoms included on the C-SCAT menu were reported at least once. Table 2 reports the five most frequent symptoms at each visit.
Interview responses were available from 83 participants. Qualitative data analysis identified seven categories related to the CSCAT's impact on AYAs' self-regulation behaviors and one category about communication with providers. Multiple subcategories were further identified under each category.
Self-efficacy for symptom management
Using a mixed linear model, none of the potential covariates (age, gender, and months since diagnosis) contributed to the model for self-efficacy; thus, the final model included effects for site, visit, and site by visit interaction with a random effect for participants. The final model identified a statistically significant effect for visit, showing that self-efficacy improved significantly over time (p = 0.034) (Tables 3 and 4).
PROMIS S-E, 28-item Patient-Reported Outcomes Information System (PROMIS) Self-Efficacy Scale (range, 28–140; higher scores indicate greater self-efficacy); PPCS, four-item Patient-Provider Communication Scale (range 0–4; higher scores indicate better communication)
p < 0.05
PROMIS S-E, 28-item Patient-Reported Outcomes Information System (PROMIS) Self-Efficacy Scale (range, 28–140; higher scores indicate greater self-efficacy); PPCS, four-item Patient-Provider Communication Scale (range 0–4; higher scores indicate better communication)
Patient-provider communication
Similar to the model for PROMIS S-E, none of the potential covariates contributed to the model, and the final model included site, visit, site by visit interaction, and a random effect for participants. The mixed linear model for the PPCS did not find any significant effect (Tables 3 and 4).
In the qualitative data under the category of communication with providers, eight subcategories reflected multiple ways the C-SCAT facilitated AYAs' discussions about symptoms with providers. (Table 5) AYAs commented that because the C-SCAT was a visual tool with standard language, talking about their symptoms was easier and faster, including their priority symptoms and symptoms that were embarrassing or sensitive. Participants indicated that the C-SCAT helped them explain their personal symptom experiences and facilitated conversations with providers about how to manage symptoms.
Subject IDs have been recoded to ensure confidentiality.
CUP, carcinoma of unknown primary; HL, Hodgkin lymphoma.
Self-regulation abilities
Analysis of qualitative interview data into categories revealed several distinct abilities related to AYAs' self-regulation of their symptoms. (Table 6). AYAs reported that the C-SCAT helped them identify and recall their symptoms, especially if memory loss was a problem, and AYAs found that the C-SCAT helped to organize their symptoms and realize how symptoms were related. Using the C-SCAT promoted reflective thinking about the severity and timing of symptoms as well as the causes and effects of symptoms and how to manage them, especially related symptoms. Finally, the C-SCAT helped AYAs prepare for what they wanted to communicate about their symptoms to providers.
Subject IDs have been recoded to ensure confidentiality.
APML, acute promyelocytic leukemia; NHL, non-Hodgkin lymphoma.
Discussion
This study explored how the C-SCAT, a heuristic symptom assessment tool, affected the process of symptom self-management among AYAs receiving chemotherapy. According to the IFSMT, AYAs will be more likely to engage in effective symptom self-management behaviors if they have knowledge and beliefs that improve their self-efficacy to manage symptoms, if they develop self-regulation abilities around their symptoms, and if they benefit from effective communication about symptom management with their providers.
Data were collected at a visit when chemotherapy was due, a time when AYAs might be expected to have fewer symptoms. AYAs in this study, however, commonly reported up to five symptoms, with some reporting 15 symptoms or more, indicating high symptom burden. The most common symptoms were those previously known to be prevalent and persistent, such as fatigue, nausea, and sleep-wake disturbances. 28 A focus on AYAs' symptom self-management strategies, therefore, remains an important area for practice and research.
AYAs who used the C-SCAT showed improved self-efficacy for managing symptoms from baseline across two visits. Self-efficacy, first introduced by Bandura in 1977, refers to the confidence a person has in their abilities to successfully engage in a behavior and is critical in self-management. 4 Self-efficacy can be measured in general, as in chronic disease management, or in relation to a specific behavior, such as symptom management. Using the PROMIS S-E tool, this study showed opportunity to improve AYAs' self-efficacy to manage symptoms. As with AYA cancer survivors 7 and adults with cancer, 29 improved self-efficacy may translate into improved symptom outcomes, which were not examined in this study, but are important variables for future symptom self-management studies.
Qualitative data suggested that the C-SCAT was useful for enhancing multiple self-regulation abilities related to symptom management, starting with awareness, identification, and recall. The C-SCAT facilitated AYAs' understanding of how their symptoms were related to each other and how symptoms affected each other. The C-SCAT promoted a greater understanding of their personal symptom experience and their priority symptoms, as well as the totality of their symptom experience. Finally, the C-SCAT stimulated thoughts about how AYAs could communicate with their providers and improve their own self-management of symptoms. These basic cognitive processes and reflective thinking about symptoms are foundational to self-regulation. 14 Enhancing these abilities may be especially important for AYAs as they may not have had prior experience with identifying, describing, and monitoring ongoing symptoms related to illness.
The PPCS did not show significant improvement in AYAs feeling connected with their providers regarding discussions about symptoms. Scale items may not have accurately captured the impact of the C-SCAT on these discussions. In addition, PPCS scores were high at baseline and may have been less sensitive to change. Interview responses, however, revealed how the C-SCAT facilitated AYAs' communication with their providers about their symptoms. AYAs found the C-SCAT, as a visual tool with standard language, was helpful to explain their symptoms to providers, including their priority symptoms and sensitive and embarrassing symptoms. AYAs have acknowledged challenges related to talking with providers, especially about mental health symptoms and sensitive topics, such as sexual function.30,31 Resources such as the C-SCAT may help AYAs overcome communication barriers with providers and promote the experience of “being known” by the healthcare team as a unique individual, which is highly valued by AYAs with cancer and helps them feel “connected” to their providers.31,32
Communication between AYAs and their providers about symptoms may lead to the mutual development of symptom management plans through negotiated collaboration. Negotiated collaboration is a process that includes open communication, mutual respect and trust, mutual goals, and shared power and decision-making.33–35 According to the IFSMT, “…negotiated collaboration occurs when “your, mine, and our” perspectives are respected and influential.”14, p. 225.e5 Comments from AYAs in the study, such as, “We discussed it and came up with a plan.” and “…ways that we can stop one symptom leading to another symptom…,” are examples of negotiated collaboration between the AYA and provider. Collaborative treatment decision-making is recommended by the National Comprehensive Cancer Network (NCCN) as a strategy to promote adherence in AYAs with cancer. 36
Limitations of this study include the single-group, nonrandomized design as well as a heterogeneous sample of AYAs, some of whom were diagnosed with cancer years earlier. Without a control group, it is not possible to determine whether AYAs' self-efficacy for symptom management and self-regulation improved naturally over time without the use of C-SCAT. How and whether every AYA in the study discussed the C-SCAT image with their provider are not known. As noted above, the PPCS was developed for this study.
Despite these limitations, this study examined how a heuristic symptom assessment tool affected several processes of self-management of symptoms in AYAs with cancer. Because AYAs may be novices in taking responsibility for their healthcare, AYAs may especially benefit from resources to promote their self-efficacy, self-regulation abilities, and communication with providers around symptom management. Electronic resources, such as the C-SCAT, are particularly appealing and feasible with this tech-savvy group of young patients, as demonstrated by AYAs in this study who easily mastered the C-SCAT. AYA providers are encouraged to develop and use age-appropriate symptom assessment tools, interventions, and resources to meet the needs of AYAs across the cancer trajectory. 37 A structured and systematic approach by providers to assess and discuss symptoms with AYAs may be helpful.
The C-SCAT demonstrated feasibility and acceptability with AYAs in a previous study. 19 This study indicated that use of C-SCAT may be an intervention to promote symptom self-management by affecting both internal (e.g., self-efficacy) and external (e.g., communication) processes. A larger, randomized controlled trial that includes a comparison group of AYAs who do not use the C-SCAT is needed to detect group differences in the self-management process, and a closer examination of AYAs' communication with providers, while using the C-SCAT, is needed. Future theory-based studies focused on AYAs' self-management behaviors will help to understand the relationships between the components of self-management. Instrument development is needed to accurately measure concepts critical to self-management. Intervention studies to improve symptom self-management must examine both short- and long-term outcomes, with the goals of relieving symptom burden and improving quality of life for AYAs with cancer.
Footnotes
Acknowledgments
The authors acknowledge the following sources of research support:
Advancing a Healthier Wisconsin Foundation Clinical and Translational Science Institute of Southeast Wisconsin St. Baldrick's Foundation University of Utah Virginia Commonwealth University School of Nursing
Disclaimer
Some of these data were presented in June 2018 at the annual conference of the Multinational Association of Supportive Care in Cancer (MASCC) in Vienna, Austria.
Author Disclosure Statement
No competing financial interests exist.