
Abstract
Purpose:
Enrollment in Children's Oncology Group (COG) clinical trials has led to significant improvements in survival; however, disparities in survival persist, particularly among ethnic minorities, adolescents and young adults (AYAs), and the underinsured, partly due to inadequate access to cooperative group cancer clinical trials. In 2008, two COG sites University of Illinois at Chicago (UIC) and Rush University Medical Center, and a nonmember institution, John H Stroger Hospital, created a unified COG program utilizing one lead Institutional Review Board and research team. This study assesses the impact that the tri-institutional COG program had on clinical trial accrual for minority, AYA, and uninsured patients.
Methods:
Analysis and comparison of COG enrollment data from 2002 to 2008 (pre-merger) and 2008 to 2017 (post-merger) by age, ethnicity, insurance type, clinical trial type, oncologic diagnosis, and specialty of the enrolling physician were completed.
Results:
Following the merger, the total studies open to enrollment increased by 100%, enrollments increased by 446%, and, for each diagnoses, increased by more than 200%. Enrollment of ethnic minorities rose by 533%, most significantly for Hispanic patients by 925%. AYA enrollments increased by 822%. There was a 28-fold increase in enrollment of uninsured patients. Significantly more providers from various oncology specialties were engaged in enrolling patients and a consistent increase in the percentile standing of the program occurred after the merger.
Conclusions:
Creation of a tri-institutional COG research program was associated with significant increases in clinical trial enrollments, especially for underrepresented minorities, AYAs, and uninsured patients. The UIC/Rush/Stroger COG Program provides a novel and exemplary approach to address cancer health disparities for these vulnerable populations.
Introduction
Considerable attention has focused on the need to increase accrual of underrepresented minority patients and adolescent and young adults (AYAs) in cancer research in recent times.1,2 Disparities in cancer burden, access to clinical trials, and survival are much less researched in children and AYAs compared to adults. 3 Five-year survival rates for children from birth to 19 years with cancer have increased significantly overall from 63% (1975–1979) to 79% (1995–1999).Nevertheless, Hispanic and African-American children continue to have lower 5-year survival rates than their white counterparts (74% and 73% vs. 81%).4,5 These differences in survival have been seen across most cancer types, including acute lymphoblastic leukemia, acute myeloid leukemia (AML), Hodgkin lymphoma, rhabdomyosarcoma, central nervous system (CNS) tumors, and neuroblastoma.6–11 Survival rates for adolescents 15–19 years of age and young adults have been notably lower compared to younger patients for most cancers.12,13
It is likely that racial/ethnic and age-related differences in survival in children and AYAs with cancer are multifactorial. Disparities in survival in minority groups are influenced by socioeconomic, cultural, biological, and pharmacogenetic differences. Furthermore, timely diagnosis and access to quality health care, as well as compliance with treatment are linked to ethnicity, socioeconomic status, and survival.1,6,14
Children's Oncology group (COG) is a pediatric focused national Cancer institute (NCI)-funded cancer clinical trials program that includes greater than 200 institutions across the world. Survival and quality of life for pediatric cancer patients have significantly improved over the last half-century due, in large part, to COG and other clinical trials networks (CTN) successful enrollment of patients onto COG or comparative network's late phase clinical trials.15–17 Careful monitoring of these clinical trials allows for effective therapies to be retained and those that are unsuccessful or toxic to be abandoned, ultimately leading to better outcomes for patients. For most cancers, children treated on standardized protocols at COG and other centers with access to cooperative group clinical trials are reported to have a significant survival advantage compared with those not treated on standard protocols.18,19 Nevertheless, AYA and ethnic minority enrollment in cooperative group trials is a valid concern that could potentially result in disparities in survival.
A recent study showed that blacks and Hispanics were underrepresented in cooperative group trials from 2000 to 2003. 17 Few previous analysis of COG data as well as a single institutional analysis highlight the underrepresentation of Hispanic children and AYAs on cooperative group clinical trials.2,20,21 The majority (71%–94%) of United States cancer patients 0–14 years of age receive care at COG centers. It is reported that only half the 15–19-year-olds and one-sixth the 20–29-year-olds compared to children <15 years enroll onto NCI-funded clinical trials. 12 Thus, only 2%–4% of AYAs enroll into cooperative group clinical trials. It is also established that a strong correlation between enrollment into NCI clinical trials and improvement in 5-year survival rates has been established at least for some for AYA cancers, such as soft tissue and bone sarcomas and leukemia22,23 Furthermore, many AYAs with cancers have different outcomes when treated on pediatric versus adult United States NCI Cooperative group regimens and often do not have access to pediatric COG protocols at community hospitals or adult centers where they receive treatment.24,25
Commonly identified universal barriers to clinical trial participation for underserved communities include distrust of clinical research among patients and restrictive eligibility criteria. 26 Institutional barriers that may contribute to reduced enrollments include regulatory challenges, limited research resources, lack of a robust NCI-funded clinical trials program at safety-net institutions, limited philanthropic funds to supplement the NCI per case reimbursement for research personnel, and failure to refer to a NCI center with such a program.27,28,29 Additional local barriers for AYA enrollment at any institution may include lack of eligibility screening procedures, limited communication between medical and pediatric oncologists, limited knowledge and comfort with COG clinical trials, time, economic constraints, and finally, psychosocial barriers that influence both the oncologist's and the patient's decision to offer and agree, respectively, to a clinical trial.30,31
A novel tri-institutional NCI-sponsored COG clinical trial program with the goal of providing improved access to COG clinical trials to underrepresented ethnic minority, uninsured, and AYA patients was created at three neighboring major medical centers in Chicago. This research describes the impact of this program on clinical trial accrual.
Methods
Program description
University of Illinois at Chicago (UIC) is a major public academic state-wide institution with 70% publicly insured pediatric and AYA patients. The Pediatric oncology service at UIC intakes around 20 new oncology patients annually, encompassing a wide range of hematologic and solid tumors. There are two pediatric oncologists and two pediatric oncology nurse practitioners on the team. Rush is a major academic private institution with 50% publicly insured pediatric patients. It takes care of 25 new oncology patients annually presenting to the pediatric oncology team composed of three pediatric oncologists and one nurse practitioner. Rush is a major referral center for pediatric and AYA musculoskeletal tumors. Stroger is a public safety net hospital with >99% publicly insured or uninsured patients, including undocumented immigrants. It intakes around 10 new pediatric oncology patients annually with two pediatric oncologists on staff. UIC, Rush, and Stroger are independent institutions located one block apart in the Illinois Medical District on the west side of Chicago (Fig. 1).
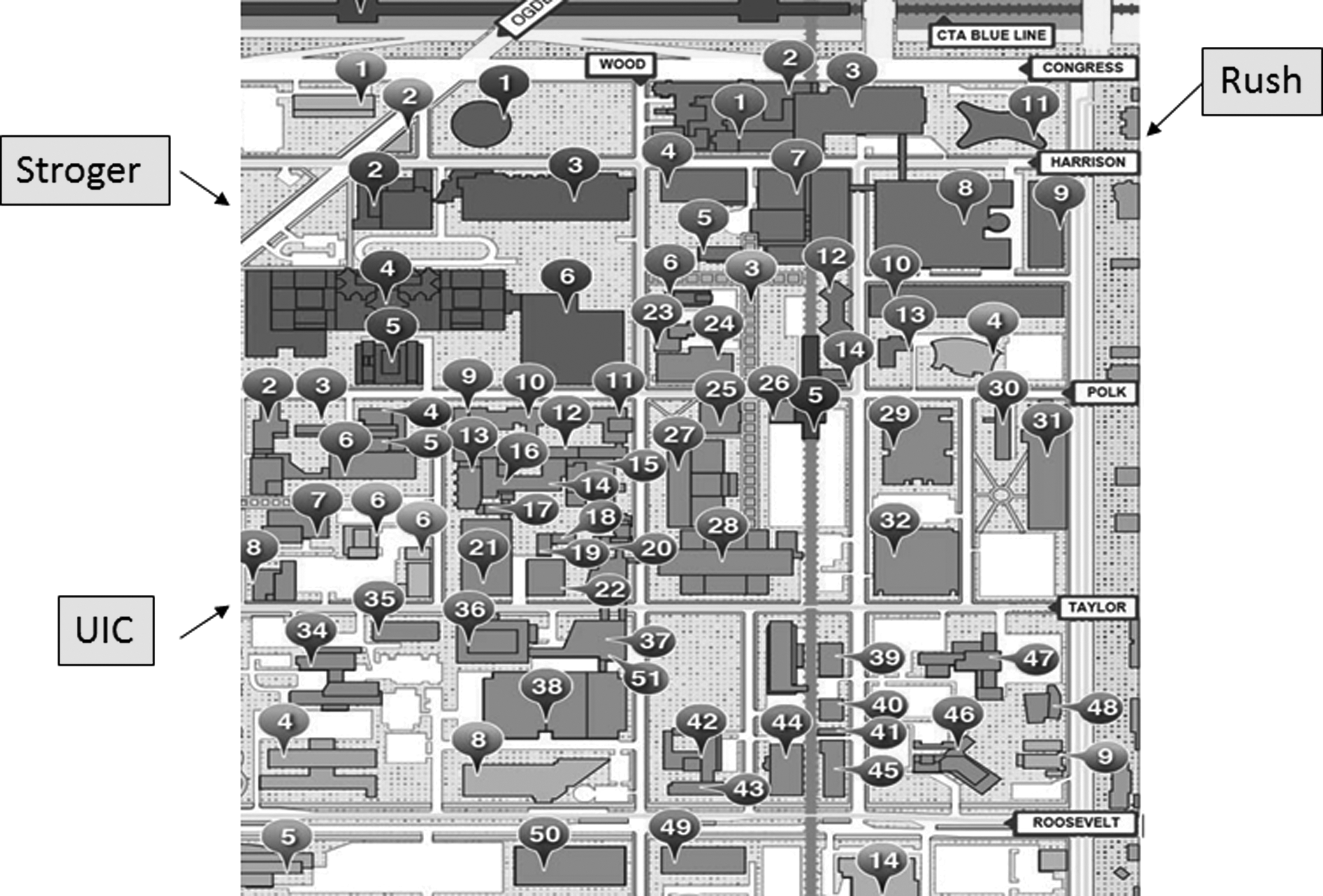
Map of the Illinois medical district depicting the three medical centers participating in the UIC-Rush-Stroger COG Program. COG, children's oncology group; UIC, University of Illinois at Chicago.
All three hospitals are full-service medical centers with medical and pediatric oncology services under the same roof. All three medical centers serve a very significant Hispanic and black population in South West Chicago. Philanthropic support and research resources to support COG cooperative group clinical trials program infrastructure are extremely limited at these institutions. Before 2008, UIC and Rush Pediatric Oncology teams ran separate, small-scale COG programs, while Stroger Pediatric Oncologists were not members of COG, and therefore, patients attending Stroger had no access to COG clinical trials. A unified UIC/Rush/Stroger COG new member application was submitted and approved in August, 2008, with a unified research team covering all aspects of COG research, including regulatory, patient enrollment, and data management. Multidisciplinary faculty from all three sites are COG members with full access to the COG resources.
Institutional Review Board oversight
The NCI-sponsored Pediatric Central Institutional Review Board (CIRB) is the Institutional Review Board (IRB) of record, with the UIC IRB serving as the lead local IRB, and inter-IRB agreements existing between UIC and Rush, and UIC and Stroger.
Study description
A retrospective comparative analysis was completed of COG enrollment data from 2002 to 2008 and 2008 to 2017 (pre-merger vs. post-merger) for all patients with cancer enrolled through the UIC/Rush/Stroger programs. The IRBs at UIC, Rush, and Stroger provided approval for this analysis of COG enrollment databases. Pre-merger and post-merger analysis were conducted for the number of COG clinical trials available, the enrollments by diagnosis, ethnicity, age, insurance type, and type of clinical trial (biology, registry, and therapeutic). Annual percentile standing of the UIC/Rush/Stroger program post-merger within COG was compared. The number of oncologists engaged in enrolling patients onto the COG clinical trials and their specialty type were also analyzed.
Results
Studies open to enrollment
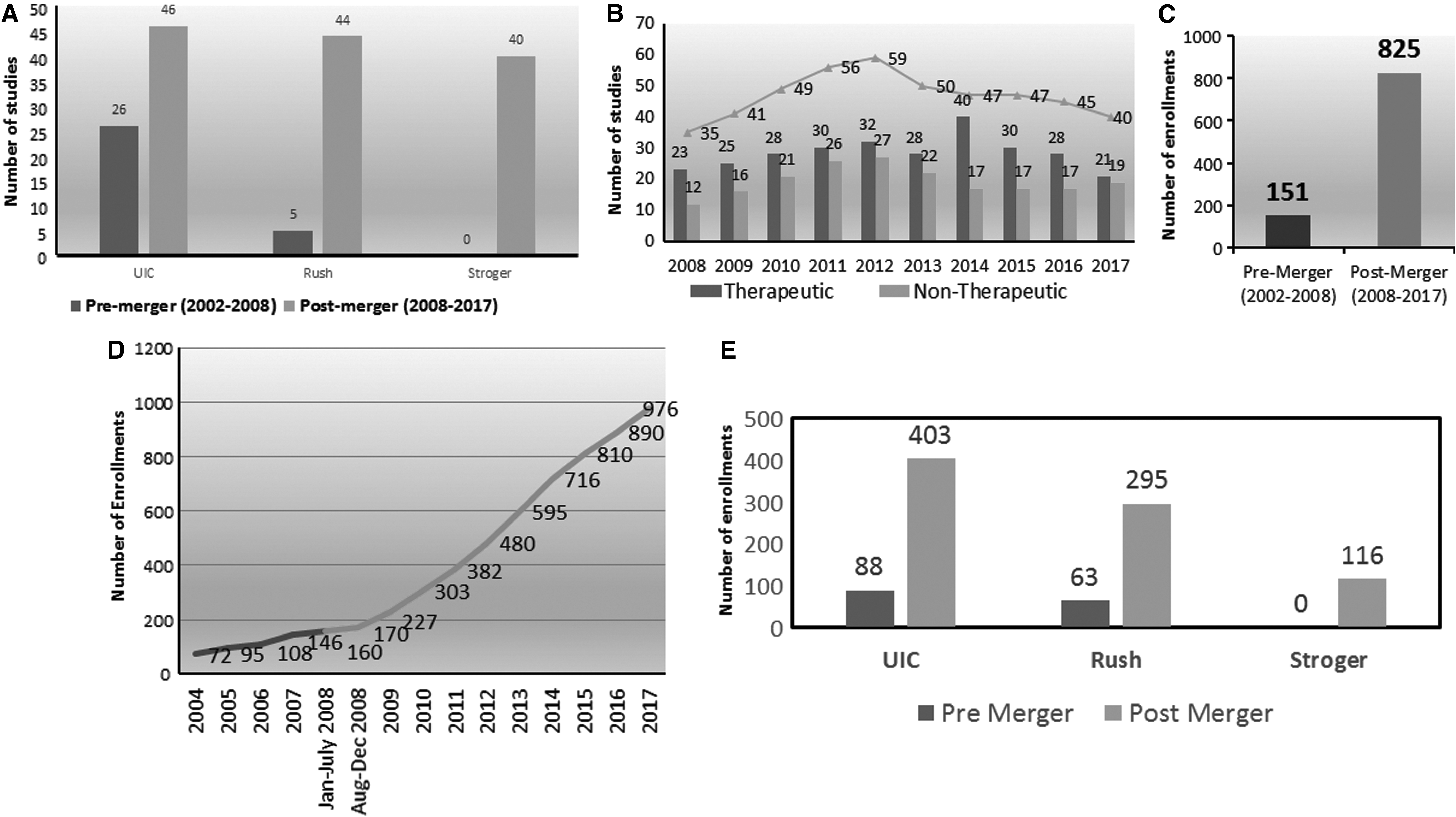
COG research protocols open for enrollment nearly doubled during the post-merger period compared to pre-merger (Fig. 2A), including therapeutic, biology, epidemiology, and registry trials across all cancer types (Fig. 2B). Some new studies included broader age eligibility, allowing AYAs to enroll in greater numbers post-merger.
Patients enrolled by disease and study type
Overall enrollments onto COG trials increased by 446% (2002–2008: n = 151, 2008–2017: n = 825) (Fig. 2C). A steady and consistent increase in enrollments were seen for the entire post-merger period, resulting in progressive growth of the UIC/Rush/Stroger COG program (Fig. 2D). Enrollments increased across all three institutions with a 357% increase at UIC and 368% increase at Rush. Stroger was not a member of COG before the merger, but had 116 enrollments in the post-merger period (Fig. 2E). Enrollments increased for all study types, including therapeutic, registry, biology, epidemiology, and cancer control, and supportive care studies (Fig. 3A). Total number of enrollments increased by at least threefold for all cancer diagnoses, the most gains in enrollments being for CNS tumors (20-fold), AML (46-fold), and non-Hodgkin lymphoma (31-fold). (Fig. 3B). The comparative percentile ranking of the UIC/Rush/Stroger COG Program rose from the 20th to the 77th percentile among all 250 COG sites (Fig. 3C). Three successful COG audits of the UIC/Rush/Stroger COG Programs have been conducted post-merger.

Engaged faculty
A greater number of treating oncologists were involved in enrolling their patients into COG trials post-merger. Successful engagement with medical oncology teams at Rush for sarcoma and neuro-oncology patients, at UIC for leukemia, gynecology, and neuro-oncology patients, and at Stroger for leukemia patients has provided improved access to COG resources for more patients, especially AYAs normally cared for outside of the Pediatric Oncology service lines. A total of 30 faculty were engaged in actively enrolling patients on COG clinical trials post-merger compared to six faculty pre-merger. No adult oncologists were engaged in enrolling patient's pre-merger compared to 21 engaged post-merger across all three institutions (Fig. 3D).
Enrollments for underrepresented minority patients
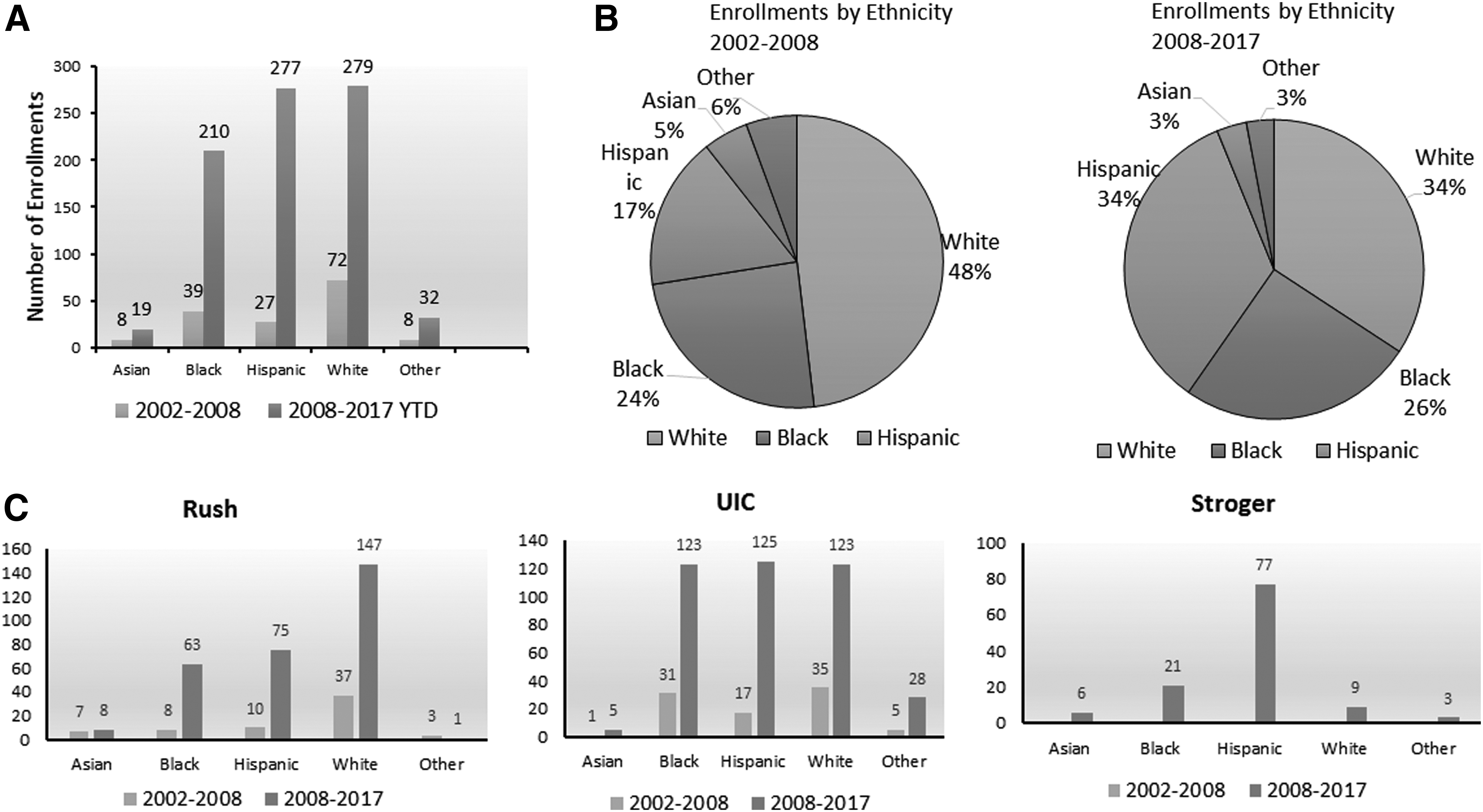
Enrollment of ethnic minority patients increased by 533% post-merger, whereas non-Hispanic white patients had a 262% increase in enrollment (Fig. 4A). Ethnic minority patients comprised 66% of enrollments post-merger compared with 52% pre-merger. Representation of Hispanic patients increased from 17% of pre-merger enrollments to 34% post-merger amounting to a 925% increase, while representation of African-American patients increased slightly from 24% of pre-merger to 26% of post-merger enrollments amounting to 438% increase (Fig. 4B). Increase in post-merger enrollments was seen for all ethnicities at all three sites; however, increases were much more robust for Hispanic patients at all three institutions (Fig. 4C).
A 296% increase was seen in enrollments for patients younger than 14 years compared to an 822% increase in total AYA enrollments observed following merger of the three institutions (Fig. 5A). AYAs constituted 49% of enrollments post-merger compared to 34% of the enrollments before merging (Fig. 5B). Of the post-merger AYA enrollments, 9.1% came off protocol therapy. Reasons for coming off protocol therapy were disease progression or death in 4.4%, noncompliance with protocol or lost to follow-up in 2.7%, toxicity to protocol therapy necessitating removal in 1.3% either by protocol requirement or physician recommendation, and other clinical change necessitating removal from protocol as per protocol requirements in 0.7%. There was also a >28-fold increase in uninsured and >7-fold increase in publically insured patients post-merger compared to rates pre-merger (Fig. 5C). Stroger patients accounted for the majority of the increase in uninsured patients as 40% of their enrollments were uninsured patients (Fig. 5D).

Thus, very significant improvements in enrollments for Hispanic and AYA patients as well as uninsured patients were a direct result of the merger.
Discussion
The dramatic improvement in survival for children with cancer is due, in large part, to the widespread adoption of recommendations made after completion of clinical trials, which become the new “standard of care” and generally guide cancer therapy for young patients across the world. 32 The proportion of children accrued to COG trials varies by access, availability of an appropriate trial and willingness of the oncologist to offer, and the patient/family to consent to trial participation. Improved outcomes for children and AYAs enrolled onto COG trials have been reported, yet the underrepresentation of racial and ethnic minorities, AYAs, and uninsured patients into late phase clinical trials remains a reality. The UIC/Rush/Stroger COG Program was established to increase access to COG trials for all children and AYAs with cancer, crossing barriers of access, age, ethnicity, and insurance status.
International recognition of underrepresentation of AYAs in cancer trials has led to initiatives across the world to provide these patients with more equitable access to trials. 33 Furthermore, the NCI and the Institute of Medicine have strongly emphasized the need to increase enrollment and lessen disparities in outcomes through improved AYA participation.34,35 Accessibility to an available NCI-sponsored clinical trial, where the minority patient seeks cancer care, is necessary to reduce disparities. 24 Before the merger, Stroger was not a COG member and therefore patients at this major safety net county hospital serving mostly Hispanic and black patients as well as a significant immigrant population had no access to COG trials. Furthermore, a very limited number of COG trials were activated at UIC and Rush, due to a lack of research resources to manage regulatory affairs, enrollment, and data, all of which are vital to successful accrual.
Patient population served by these three hospitals represents a significant segment of lower income communities majority, of which are Hispanic or black on the South and West side of Chicago. Thus, the availability of COG clinical trials to these patients was severely restricted. After the merger, sharing of all research infrastructure, including IRB oversight and research personnel, allowed for a significant expansion of the COG palette of open trials. With greater engagement of medical oncologists and a unified research team, collaborative IRB oversight, and greater number of open COG trials, dramatic improvements in patient enrollments, including ethnic minorities and AYAs, were seen at all three sites.
The tri-institutional COG Program increased enrollment of disadvantaged groups into a wide variety of clinical trials, including registry, biology, and cancer control, and supportive care trials, diversifying the study population and the tumor specimens submitted, which impact research outcomes. Furthermore, the increased enrollment lends more opportunities for investigational studies as well as a better understanding of outcomes and toxicities.
UIC, Rush, and Stroger Medical Centers include both pediatric and medical oncology practices. This presents an opportunity to improve AYA enrollments. The increase in AYA accrual within the UIC/Rush/Stroger COG program resulted from a growing collaboration between pediatric and medical oncology teams, with dedicated personnel working with medical oncologists to successfully enroll patients and complete all research requirements. This was further enhanced with regular shared tumor boards and regular and deliberate communication between COG CRA's and medical oncology teams to ensure compliance with all study procedures and requirements. Relationship building with medical oncology colleagues is an ongoing and gradual process with one provider at a time and requires dedicated time and commitment of physicians from both sides of the aisle.
Other strategies for encouraging AYA accrual have been explored, including physician and community education, development of dedicated AYA programs, modifying referral patterns, and expansion of eligibility of cooperative group initiatives to include AYAs.36,37 Greater than 80% of AYA cancers in the United States are managed in community hospitals or clinics and not at major cancer centers. 37 One strategy that has been utilized is to connect community-based oncologists to major academic centers, and recent reports show community oncologists contribute up to one-third of the patients placed on investigational protocols. 37 Similarly, the success of the UIC/Rush/Stroger COG Program derives from the partnering of two academic institutions with a neighboring safety net hospital that cares for a large uninsured and underserved population.
Under enrollment remains a major challenge among ethnic minorities.2,21,22 Low socioeconomic status and rural residence contribute to underaccrual for this population. Limited research exploring the role of geographic proximity and racial disparities in participation of pediatric patients in cancer clinical trials is available.38–42 Place of residence and race are found to be significant predictors of participation.43,44 In this regard, lack of transportation to and from, and the travel distance to the site where a NCI clinical trial is open and available are important determinants of successful accrual. 45 The UIC/Rush/Stroger COG program is an example of a successful collaboration that brought COG clinical trials' resources to the patient's oncology service provider. This contributed to the dramatic increase in enrollments for underrepresented ethnic minorities, especially the Hispanic patients, many of whom were underinsured or uninsured.
Several national and regional consortia have implemented programs to increase ethnic minority participation in cancer clinical trials.45–47 NCI's Community Cancer Oncology Program was designed to increase minority participation in cancer clinical trials by community outreach efforts at institutions that serve large numbers of minority cancer patients. 44 The success of this program was attributed to opening trials that were tailored to the clinical characteristics of specific patient populations and successful collaborations with local physicians, which increased referral of minority patients to clinical trials. 47 Lack of adequate health insurance can present as a major barrier for patients with cancer, who are often recommended prolonged or expensive therapy. Klabunde et al. reported that self-pay adult enrollees were 60% less likely to participate in cancer clinical trials than privately insured patients. 48 A strong advantage of the UIC/Rush/Stroger program was the ability to offer clinical trials to uninsured patients.
There are data to suggest that, while opening clinical trials at minority-serving institutions lead to improved access to trials, achieving significant gains in enrollments may require further steps, such as providing appropriate institutional resources to be made available to support the complex process of clinical trial recruitment. Other institutional steps in this direction include modifying clinic structure to encourage physicians to enroll patients, building a multidisciplinary care team, improving continuity of care, and addressing the competing provider responsibilities. Sharing scarce research resources among institutions should also be considered.46,49
The UIC/Rush/Stroger COG Program is an effective model due to the full engagement by all pediatric oncology teams, the commitment to share resources, interinstitutional and interdepartmental collaborations, consistent long-term leadership, gradual and strong investment by institutional cancer centers, and the modest, but increasing philanthropic support. A cursory review of the tumor registries at each institution strongly suggests that the UIC/Rush/Stroger Program has further potential, and with COG support, financial investment, and local engagement, growth should continue.
In conclusion, it is known that disparities in oncology clinical trial participation are associated with disparities in outcomes. Enrollment into NCI-sponsored COG trials offers an important opportunity for young patients to receive the latest innovations in cancer care, and studies report that underrepresentation of minorities and AYAs negatively impacts equality of care. The UIC/Rush/Stroger COG Program is an example of a successful collaboration of neighboring institutions utilizing scarce research resources, which led to a dramatic improvement in enrollments into COG trials for underserved populations: most impressively for Hispanic and AYAs, and for blacks and uninsured or underinsured patients with pediatric malignancies. This program can be duplicated or modified to address various health disparities for patients with cancers in various communities.
Footnotes
Acknowledgment
The UIC-Rush-Stroger COG program has received funding support from St. Baldrick's Foundation from 2008–2018.
Author Disclosure Statement
No competing financial interests exist.