
Abstract
Purpose:
Diminished reproductive function can be a major late effect of childhood cancer treatment. This study evaluates the changes, and occurrence of possible recovery, in gonadal function markers in children treated for cancer.
Methods:
Gonadal function markers were measured before (T0), directly after (T1), and 1 year after (T2) end of treatment of childhood cancer. Anti-Müllerian hormone (AMH) was measured in girls and inhibin B in boys and compared to reference populations. Repeated measures analysis of variance and t-tests were employed for data analysis.
Results:
Baseline gonadal function markers (T0) at diagnosis were available in 129 girls and 150 boys. Paired gonadal function markers were available in 49 girls and 54 boys for T0–T1, and in 27 girls and 32 boys for T1–T2. Gonadal function markers were significantly lower than the reference population at each time point (p < 0.001). Post-menarcheal girls showed a decrease in AMH between T0 and T1 (standard deviation scores [SDS] −0.72 to −1.32, p = 0.007), and in the boys cohort, a decrease in inhibin B (SDS −1.14 to −1.43, p = 0.045) was observed. Impaired gonadal function levels (<5th percentile) at T1 were observed in 15 of 27 (56%) girls and in 15 of 32 (47%) boys. However, gonadal function had recovered at T2 in seven girls and six boys.
Conclusion:
Our data suggest that gonadal function is already compromised at diagnosis and is further decreased by childhood cancer treatment. Nevertheless, about half of the children with gonadal impairment recovered over time. Evaluation of gonadal function markers before 1 year after end of treatment may therefore be unreliable.
Introduction
Childhood cancer survival (CCS) rates have improved significantly over the last decades, with 5-year survival rates averaging 80% in Western countries. 1 The increase in the absolute number of CCS has caused a concomitant increase in the incidence of complications related to cancer treatment.2,3 A well-known late effect of childhood cancer treatment is loss of gonadal function, which is especially observed after treatment with high doses of alkylating chemotherapeutics, stem cell transplantation, and/or after radiation on the gonads.4,5 In addition, we recently reported that already at diagnosis of childhood cancer, gonadal function markers were reduced in both boys and girls, indicating that gonadal function in children with cancer is affected not only by cancer treatment but also by the disease itself before treatment.6,7
Children with cancer and their parents consider fertility an important future health issue and are often anxious to find out if their treatment has caused gonadal impairment.8,9 To prevent unnecessary grief or unwarranted hope, knowledge on the trends of gonadal function and possibly the appropriate timing of analysis of gonadal status after childhood cancer would be valuable. However, longitudinal studies on the effects of cancer treatment on gonadal function in children are scarce.
In the assessment of gonadal function in men, semen analysis is considered the gold standard. 5 Inhibin B, mainly produced by Sertoli cells of the testis under influence of follicle-stimulating hormone (FSH), is a marker of spermatogenesis as it is positively correlated with sperm count and concentration in adulthood.10–12 Given the substantial patient burden or impossibility of obtaining semen samples from young boys (by masturbation or electroejaculation), inhibin B is considered a feasible and adequate surrogate marker for gonadotoxicity in young boys.5,13–15
To assess gonadal function in women, the gold standard combines endocrine measurements of FSH, luteinizing hormone (LH), estradiol, and progesterone with antral follicle counts and menstrual history. 16 In pre-pubertal girls, gonadotropins and antral follicle count are unreliable as the hypothalamic-pituitary-gonadal axis might still be dormant. A useful marker that reflects gonadal function is anti-Müllerian hormone (AMH). AMH is produced by the granulosa cells of the preantral and small antral follicles in the ovaries and reflects the quantitative status of the ovarian reserve in adult women.17–20 AMH levels rise during infancy until a peak in the mid-20s, after which the levels slowly decline in parallel with the gradual decline in ovarian reserve, until the end of reproductive age.21,22 Over the last decade, both AMH and inhibin B have been used in clinical settings, and previous studies demonstrated its clinical usefulness to evaluate gonadal function in children with cancer.14,23,24
The aim of this study was to study the direct effect of disease and cancer treatment on gonadal function markers and to assess the frequency of gonadal function impairment in children before and after childhood cancer treatment. Furthermore, potential recovery of gonadal function markers and its determinants were explored.
Materials and Methods
Patients
We included boys and girls newly diagnosed with cancer up and until 18 years of age between January 2010 and January 2014, who had available remnant serum after routine workup. Ovarian cryopreservation was not yet standard of care at that time. Patients with brain or germ cell tumors were excluded. Patients who received stem cell transplantation experienced a relapse or who died were only measured at diagnosis. Details on age, gender, pubertal stage, diagnosis, and treatment were retrieved from our local database. In boys, pubertal status was assessed clinically at diagnosis and classified as pre-pubertal (Tanner stage 1) or pubertal (Tanner stage 2–5). 25 Girls were classified according to status before or after menarche. Treatment was categorized as low or high risk for gonadal function impairment (high-risk treatment defined as radiation on the abdomen and/or a cyclophosphamide equivalent dose score >4000). 26
This study was approved by the Medical Ethics Committee Erasmus MC of Rotterdam, The Netherlands, with waiver of the requirement for patients' written informed consent (MEC-2018-1399).
Hormone level assessment
Remnant material was collected if available before start of treatment (T0), directly after treatment (T1, median 1 month, range 0–6 months after end of treatment), and later after end of treatment (T2, median 10 months, range 6–23 months). Blood samples were stored at −80°C until analysis. AMH and inhibin B levels were measured at the end of the study at the Erasmus MC laboratory, Rotterdam, the Netherlands. These data were supplemented with clinically measured AMH and inhibin B levels, which were available in ∼10% of the participants. In 2010, clinically measured AMH levels were obtained using an ultrasensitive enzyme-linked immunosorbent assay (ELISA) (Immunotech-Coulter, Marseille, France). These AMH values were batch by batch adjusted to allow comparison with the currently used ELISA (commercially available as the Gen II Beckman Coulter; Beckman Coulter, Inc., Webster, TX), which was employed at the end of the study enrolment. Intra-assay and interassay variation coefficients were <5 and <10%, respectively. 27 Age-matched reference values were based on a cohort with 250 healthy girls, whose samples were measured in the same laboratory using the same assays. 22 After the statistical analyses were performed, FSH, LH, and estradiol and progesterone levels were measured in available remnant plasma to assess our hypothesis of the recovery of gonadal function.
Inhibin B levels were measured using an ELISA (Inhibin B Gen II ELISA Kit; Beckman Coulter, Inc., Brea, CA). Intra-assay variation coefficient was <5% over the whole measuring range and inter-assay variation coefficient was 5% (at the average concentration of 195 ng/L) to <15% (at the average concentration of 22 ng/L), respectively. Inhibin B levels were compared with age-matched reference values from previously published literature. 13
Statistical analysis
To account for age dependency of the repeated gonadal function markers, standard deviation scores (SDS) were calculated using AMH and inhibin B reference values.13,22
The one-sample t-test was used to test a statistical difference between the mean SDS of the included participants at each time point compared to the reference population. Repeated measure analysis of variance (ANOVA) was used to test differences in AMH SDS (for girls) and inhibin B SDS (for boys) at the three time points. Greenhouse–Geisser's epsilon adjustment was used in all cases when Mauchly's test indicated that the sphericity assumption had been violated. When significance was demonstrated in the repeated measure ANOVA, the paired t-test was employed for any significant main effect.
To examine the associations between patient and treatment characteristics and the gonadal function markers, univariable linear regression was used. Variable groupings of the potential risk factors were selected based on clinical relevance and to assure adequate numbers of persons within groups for statistical power. Variables that were associated with the gonadal function maker with a p value <0.20 in the univariable analysis were included in the multivariable linear regression model with the gonadal function markers in SDS as outcome. Analysis was repeated with the crude AMH (μg/L) and inhibin B (ng/L) levels. Results of both analyses were similar and, therefore, only the analysis of the SDS is reported.
A small change in SDS, especially in the higher regions, is unlikely to be of clinical relevance and could obscure the results. We therefore classified the gonadal function markers as a likely sign of gonadal function impairment when the markers were on or below the 5th percentile (or below a SDS of −1.645, the corresponding z-score) of the reference values. Univariable logistic regression analyses were used to identify potential determinants for gonadal function impairment. Within the group with impaired gonadal function markers directly after treatment (T1), the Mann–Whitney U test was used to compare the groups that did and did not show recovery at T2. Statistical analyses were performed with the Statistical Package for Social Sciences version 24.0 (SPSS, Chicago, IL).
Results
Baseline gonadal function markers were available in 129 girls and 150 boys with newly diagnosed childhood cancer. In total, 49 girls and 59 boys had gonadal function markers available on at least two time points. The group with available longitudinal data was similar with respect to their baseline gonadal characteristics as the group without longitudinal data (Table 1). At diagnosis, the mean age of the girls was 7.6 years (range 0.9–17.4) and 75.5% of the girls were pre-menarcheal. Mean age at diagnosis of the boys was 7.3 year (range 0.6–16.2) and 79.7% of the boys were pre-pubertal (Table 1). Ovarian tissue cryopreservation was not offered in our hospital at this time yet to these newly diagnosed girls.
Baseline Characteristics of Included Children with Childhood Cancer with the Total Group of Children with Childhood Cancer
Data are expressed as mean (range) or frequencies (%). Radiation is depicted as n (range total dose in Gray).
Difference in SDS between cohorts with one gonadal marker and with available follow-up markers: p value 0.61 (boys) and 0.25 (girls).
ALL, acute lymphoblastic leukemia; AMH, anti-Müllerian hormone; AML, acute myeloid leukemia; B-NHL, B-cell non-Hodgkin lymphoma; CED, cyclophosphamide equivalent dose; LCH, Langerhans Cell Histiocytosis; T-NHL, T cell non-Hodgkin lymphoma; SDS, standard deviation score.
FSH, LH, and estradiol and progesterone serum concentrations were not correlated with AMH or inhibin B levels. None of the children had elevated FSH levels above 10.0 U/L (data not shown).
Girls
Before start of treatment (T0), AMH levels were below the 50th percentile in 43 girls (87.8%) and 1 (2.0%) was below the 5th percentile. After a median of 1 month after treatment (range 0–6 months, T1), AMH levels were below the 50th percentile in 44 girls (89.8%), and below the 5th percentile in 21 (42.9%) girls (Fig. 1).
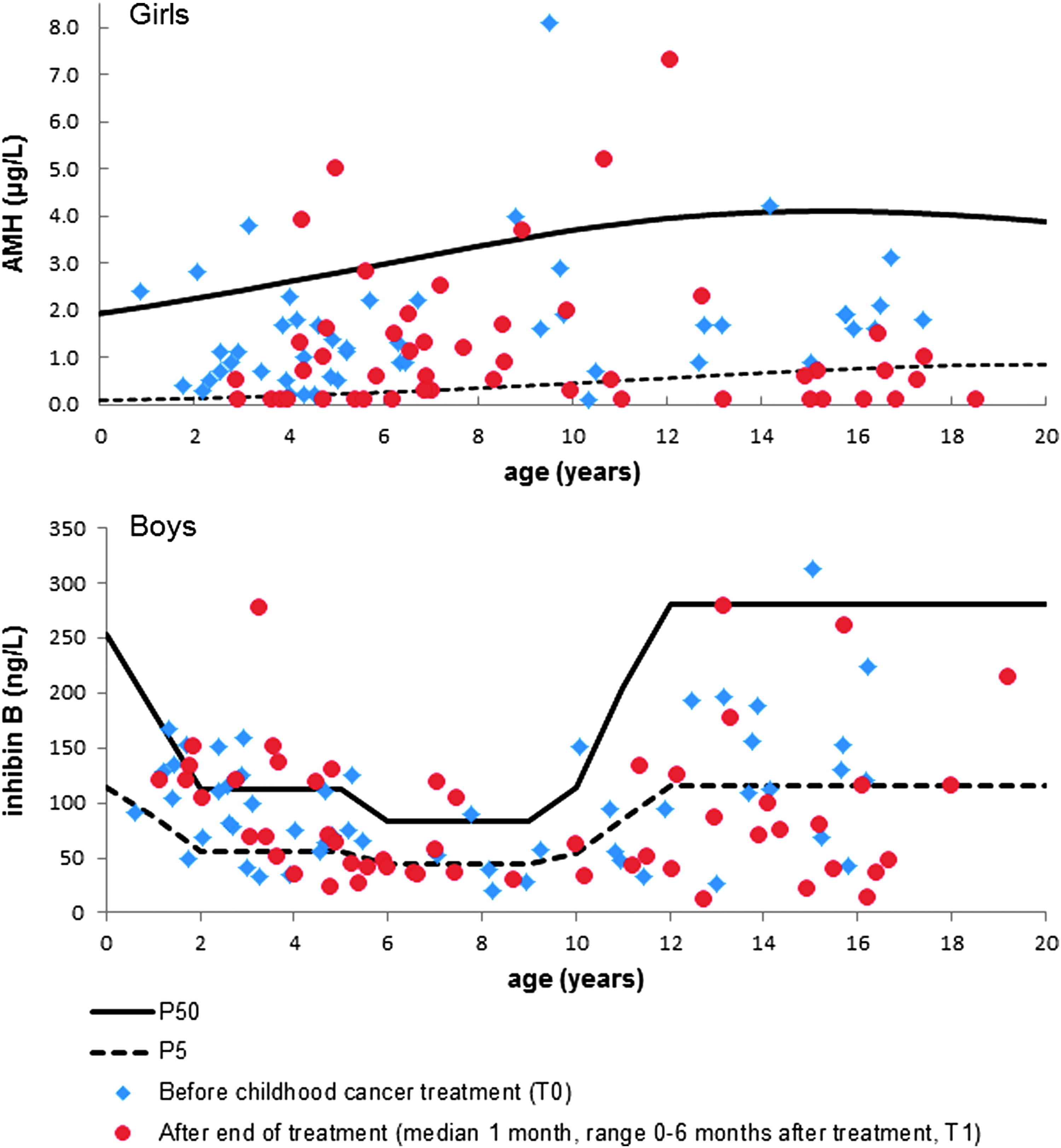
Girls' AMH and boys' inhibin B levels before and after cancer treatment. AMH (upper figure, in 49 girls) and inhibin B (lower figure, in 54 boys) levels before childhood cancer treatment (T0) and 1 month after childhood cancer treatment (T1; median 1 month, range 0–6 months). P50 and P5 refer to 50th and 5th percentiles of reference range populations.13,22 AMH, anti-Müllerian hormone.
Mauchly's test indicated that the sphericity assumption had not been violated (p = 0.077), with a Greenhouse–Geisser's estimate of sphericity (ɛ = 0.844). The repeated measures ANOVA showed a significant difference in AMH over time (p = 0.027). Paired analysis showed that the decrease in AMH levels in post-menarcheal girls between before treatment (T0: mean SDS −0.72) and 1 month after treatment (T1: mean SDS −1.32) was significant (p = 0.007; Table 2). However, in pre-menarcheal girls, this decrease was not significant (from mean SDS −1.00 to SDS −1.04, p = 0.766). The decrease was significant (p = 0.002) in the high-risk treatment group (from mean SDS −0.82 to SDS −1.44) (Table 2).
Paired Analysis of Gonadal Function Markers in Children with Cancer
Gonadal function markers (AMH and inhibin B) are reported in SDS from reference populations. Data are presented as mean (standard error) or mean (95% CI of the difference). CED score (Green et al. 26 ). High-risk radiation field (for iatrogenic hypogonadotropic or hypergonadotropic hypogonadism) is defined as radiation on the abdomen or cranium. High-risk treatment is defined as radiation on the abdomen and/or a CED score >4000.
p Value <0.001 (one-sample t-test).
^p Value <0.05 (paired samples t-test).
Analysis was not performed because of small number of patients.
95% CI, 95% confidence interval; CED, cyclophosphamide equivalent dose; T0, before start of treatment; T1, directly after end of treatment (median 1 month, range 0–6 months); T2, median interval after end of treatment, 10 months (range 6–23 months).
After treatment, between T1 and T2, AMH levels significantly increased from a mean SDS of −1.31 to a mean SDS of −0.87 (p = 0.018). This increase was specifically observed in the pre-menarcheal subgroup and in those not in the high-risk treatment group, but there was no significant change in AMH levels in post-menarcheal girls and girls in the high-risk treatment group (Table 2). Table 3 shows the univariable and multivariable linear regression models for AMH levels at T1 and T2. After multivariate linear regression, no determinants remained significantly associated with AMH levels at T1 or T2.
Association of Patient and Treatment Factors with Girls' Anti-Müllerian Hormone (in Standard Deviation) at T1 and at T2
Variables with p values <0.20 from the univariable linear regression analysis were included in the multivariable linear regression model. CED score (Green et al. 26 ). High-risk radiation field is defined as radiation on the abdomen or cranium. High-risk treatment is defined as radiation on the abdomen and/or a CED score >4000.
Of the 27 girls with paired data at T1 (1 month after end of treatment) and T2 (10 months after end of treatment), 15 girls (56%) had AMH levels below the 5th percentile at T1 (Fig. 2). Only 8 of these 15 girls still had AMH levels below the 5th percentile 10 months after end of treatment (T2) (positive predictive value 0.53). In the other seven girls, AMH levels increased to levels above the 5th percentile at T2. Of the 15 girls with gonadal impairment 1 month after treatment, 9 were pre-menarcheal and 7 of them showed recovery 10 months after end of treatment, while all 5 post-menarcheal girls remained below the 5th percentile. Of the 15 girls with gonadal impairment, 6 had been treated with high-risk treatment and 5 of these 6 girls remained below the 5th percentile (Supplementary Table S1).
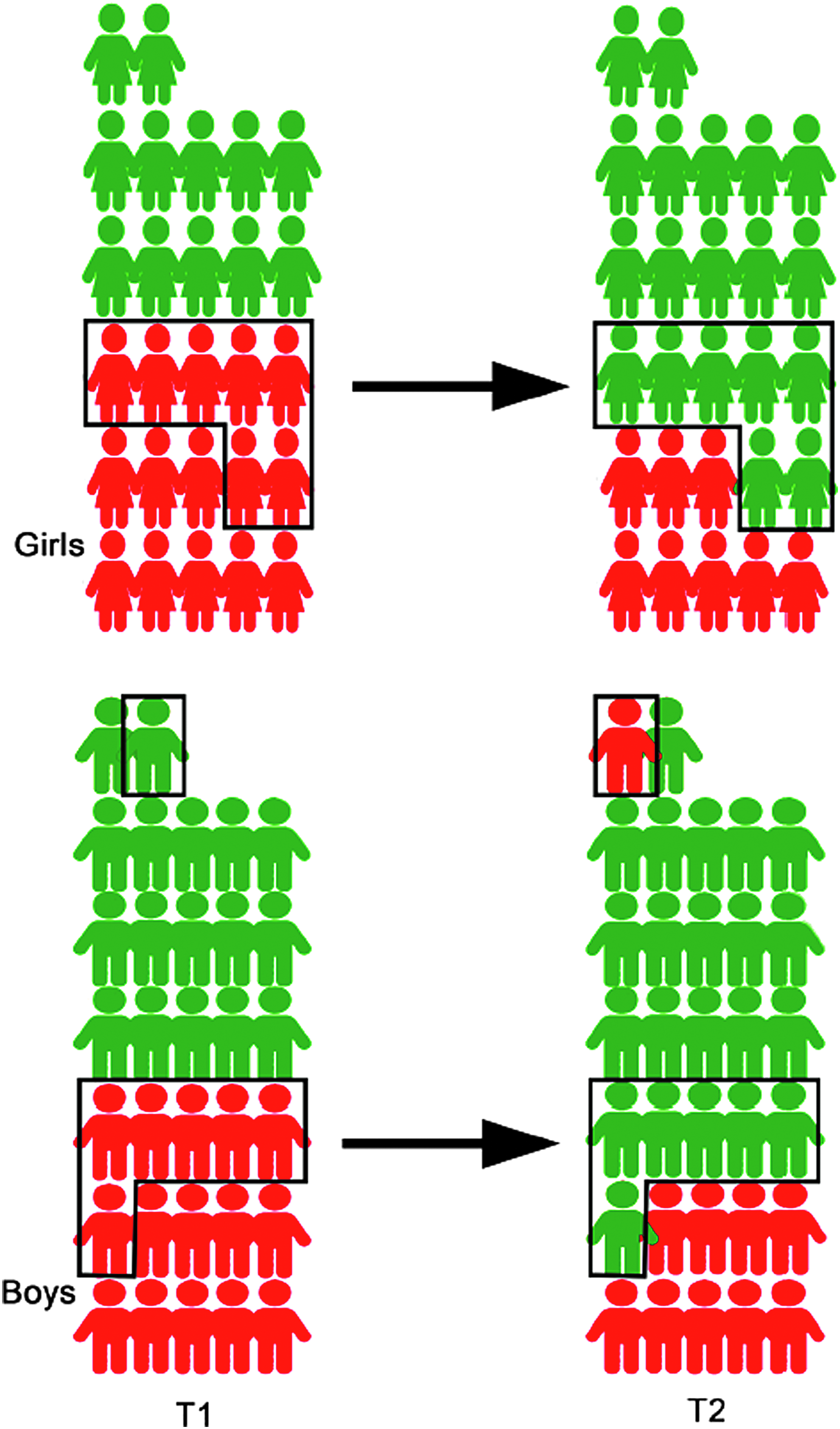
Recovery of gonadal function markers after cancer treatment. Infographic depicting the frequency of impaired gonadal function levels after childhood cancer treatment. Children with impaired levels (defined as ≤5th percentile of reference values)13,22 are depicted in red, and children without impaired markers are depicted in green. Children were evaluated directly after end of treatment (T1, median 1 month, range 0–6 months) and later after end of treatment (T2, median 10 months, range 6–23 months). Above: paired levels of AMH after treatment were available in 27 girls. Of the 15 girls with impaired markers at T1, 7 did not have impaired levels anymore at T2. Below: paired levels of inhibin B after treatment were available in 32 boys. Of the 15 boys with impaired markers at T1, 6 did not have impaired levels anymore at T2, while one of the boys without impairment at T1 did have an impaired inhibin B level at T2.
Boys
Inhibin B levels were below the 50th percentile in 45 (83.3%) boys with newly diagnosed cancer (at T0) and below the 5th percentile in 16 (29.6%) boys. One month after treatment (T1), inhibin B levels were below the 50th percentile in 46 (85.2%) boys and below the 5th percentile in 27 (50.0%) boys (Fig. 1).
Mauchly's test indicated that the sphericity assumption had been violated (p = 0.015), with a Greenhouse–Geisser's estimate of sphericity (ɛ = 0.777). The repeated measures ANOVA did not show a significant difference in inhibin B over the three time points (p = 0.168). Analysis of all paired samples available for T0 and T1 showed that the decrease in inhibin B levels between T0 (mean SDS −1.14) to T1 (mean SDS −1.43) was significant (p = 0.045) (Table 2). After multivariable linear regression, only initial inhibin B levels remained significant determinants of inhibin B levels at T1 (Table 4). No statistically significant change in linear inhibin B levels was observed during follow-up after end of treatment (Table 2). Multivariable analysis of inhibin B at T2 showed only a significant association with the inhibin B levels (in SDS) at T1 (Table 4).
Association of Patient and Treatment Factors with Boys' Inhibin B (in Standard Deviation Score) at T1 and at T2
Variables with p values <0.20 from the univariable linear regression analysis were included in the multivariable linear regression model. CED score (Green et al. 26 ). High-risk radiation field is defined as radiation on the abdomen or cranium. High-risk treatment is defined as radiation on the abdomen and/or a CED score >4000.
Of the 32 boys with longitudinal data after treatment, 15 boys (47%) had inhibin B levels below the 5th percentile at 1 month after treatment (T1) (Fig. 2). Nine of these 15 boys (positive predictive value 0.60) remained below the 5th percentile 10 months after treatment (T2). Of the 15 boys with gonadal impairment 1 month after end of treatment, 5 boys had been treated with high-risk treatment, and 4 of these 5 boys remained below the 5th percentile, while in the lower risk treatment group, 5 out of 10 boys recovered (Supplementary Table S1).
Discussion
The results of this longitudinal study of childhood cancer suggest that levels of gonadal function markers at the time of diagnosis are significantly lower compared to those in healthy age-matched controls. Moreover, treatment causes an additional decrease in gonadal function markers. However, gonadal function markers recovered in about half of the patients.
The finding of decreased gonadal function markers at the time of diagnosis, even before treatment has started, confirms findings in smaller cohorts.6,7,23,28–30 This indicates that gonadal function in children with cancer is affected not only by gonadotoxic treatment but also by the disease itself, as a possible effect of chronic disease. Similar findings were reported by Brougham et al. 23 in 22 pre-pubertal and post-pubertal girls with slightly lower AMH levels before treatment. The subsequent decrease in AMH levels during treatment is an expected finding that was also observed in other studies.28,29 In other longitudinal studies addressing AMH before and after childhood cancer treatment, high-risk groups did not show recovery, whereas the lower risk groups did recover.23,28,29 This is in line with the results of our study, where more than half of the female survivors with impaired AMH levels directly after the treatment recovered after 1 year. In fact, the positive predictive value of an AMH level below the 5th percentile for persistent impairment up to 10 months after treatment was very poor. Although this study was not powered to determine which groups have the highest odds for this recovery, our study confirmed the earlier findings of recovery in lower risk groups.23,28,29 Moreover, after treatment, girls in a high-risk treatment group were more likely to stay below the 5th percentile of age-adjusted AMH levels when compared to girls in a low-risk treatment group.
Our observations also suggest that gonadotoxicity occurs more often in post-menarcheal girls and that pre-menarcheal girls are more likely to recover from a very low AMH level than post-menarcheal girls. This corresponds with the hypothesis that gonadotropin-releasing hormone (GnRH) agonists are effective in preventing ovarian function loss in young adult women treated for breast cancer with chemotherapy. Although debate on this topic is still ongoing, large randomized controlled trials indicate a protective effect of GnRH analogues.31–34 Alternatively, the observation that pre-menarcheal girls seem to be less susceptible for long-lasting gonadotoxicity could also be due to the fact that ovaries from pre-menarcheal girls have a larger pool of follicles, making them more resistant to chemotherapy.
The increase or recovery of AMH levels after cancer treatment exemplifies the dynamic nature of the female gonad. The ovarian pool is determined before birth and cannot be replenished. Therefore, the observed increase in AMH levels must indicate restoration of folliculogenesis and the concomitant growth of follicles that produce AMH. In terms of physiological senescence, AMH can be referred to as a surrogate marker for quantitative ovarian reserve—although not of its qualitative status. 20 We feel that in the context of childhood cancer, however, the term “ovarian reserve” may be misleading and should be replaced by the more accurate “ovarian function.” This term allows for a better description of the dynamic nature of the gonads as well as of AMH after childhood cancer.
Our finding that inhibin B levels in boys were lower than the range of the reference population at all time points contrasts with the results of a previously reported longitudinal study. 14 In this study, chemotherapy had only limited effect on inhibin B levels in pre-pubertal boys. 14
Previously, we showed that normalization of mildly decreased inhibin B levels in very long-term adult survivors is possible, while a normalization in inhibin B levels did not occur in survivors who had levels below a critical level of 60 ng/L. 35 Although we here report a different cohort, it could be hypothesized that survivors with gonadal impairment, who have some recovery potential, demonstrate their recovery only shortly after end of treatment. If recovery does not occur at that time, it is unlikely that they will do so later in life.
Inhibin B is secreted from the Sertoli cells that seem more susceptible to alkylating agents than Leydig cells. This explains why earlier studies reported normal levels of testosterone, produced in the possibly more cytotoxic resistant Leydig cells, in cancer survivors who did show compromised inhibin B levels.5,36 The recovery of inhibin B levels could be a result of reactivation of Sertoli cell production of inhibin B, as a result of normalized gonadotropins, or of restored function of seminiferous epithelium.
Although the number of patients analyzed in this study is larger than those in previous studies on this topic and presents longitudinal data for both boys and girls, the number is still relatively small for statistical analysis in subsets in this heterogeneous cohort. Future replication in a larger independent prospective cohort of childhood cancer patients with follow-up beyond 2 years after end of treatment compared to a healthy control group is necessary.
Conclusion
Our results indicate that in children diagnosed with cancer, levels of AMH in girls and inhibin B in boys are compromised at the time of diagnosis and are further decreased directly after treatment. However, AMH as well as inhibin B levels recover after 1 year in a relatively large proportion of children, especially in the lower risk group and in pre-menarcheal girls. This has implications for how and when these children should be counseled regarding their future fertility. Evaluation of gonadal function markers within the first year after treatment may not be advisable.
Footnotes
Acknowledgments
The authors would like to thank Rolinda Stigter and Aleid van Noortwijk for their help in accrual of remnant plasma and Jesse H. Krijthe for his statistical advice. A.L.F.vdK. and S.M.F.P. have received funding from the European Union's Seventh Framework Programme for research, technological development, and demonstration under grant agreement no. 602030. S.M.F.P has been supported by grants of KOCR, KiKa, and Janivo Society.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.