
Abstract
Purpose:
As part of a programmatic educational initiative, we developed a personal narrative presentation, embedded with evidence-based data, to raise awareness of adolescents and young adults (AYAs) who have been diagnosed with cancer between the ages of 15 and 39 years among similarly aged university students. The narrative encompassed the cancer care continuum from signs of the disease through survivorship and incorporated psychosocial aspects of the experience.
Methods:
The presenter, diagnosed with lymphoma at the age of 25 years in 2007, interwove AYA data with her narrative in a series of 26 invited lectures given over 2 academic years, 2016–2017 and 2017–2018. Students were asked to provide anonymous open-ended feedback. Six hundred thirteen forms were collected and retrospectively dually coded and analyzed.
Results:
The majority of students (97%) referenced at least one of the presentation's three objectives: (1) build awareness of the AYA demographic; (2) encourage a personal health care focus; and (3) expand awareness of the far-reaching impact of cancer (i.e., psychological, social, and medical) both during and beyond the treatment phase. Format- and/or content-related suggestions and potential benefits of hearing the narrative also were reported.
Conclusion:
The use of personal narrative to raise awareness of the AYA cancer experience in an academic setting is both feasible and effective. Students demonstrated a new or enhanced understanding of AYA cancer and its biopsychosocial implications. We provide evidence to inform the design of awareness interventions directed at similarly aged university students.
Introduction
Adolescent and young adult (AYA) research was declared a priority area for several reasons, including that cancer is the leading cause of disease-related death in this age group. 1 Given the disease burden, the National Cancer Institute (NCI) 2 and American Cancer Society 3 urge the importance of education and prevention strategies with the general public. Cancer educational efforts geared toward AYAs have focused on the nascent 4 field of cancer prevention and awareness5–10 and the need for provider education.1,6,11–13
Targeting individuals in early adulthood is described by Holman et al. 14 as a window of opportunity for timely cancer prevention. This age span is characterized by lifestyle transitions that feature the quest for autonomy and increased social influences.15–17 Raising awareness of cancer in this prime developmental period provides an opportunity to affect AYA health at present, as well as throughout their life span.4,5,16,18–20 University students, who fall within the NCI designated AYA age range of 15–39 years, have been found to have less than optimal baseline knowledge about cancer21,22 and are underinformed about the connection between healthy behaviors and risks. 7 Many modifiable risk factors are common during this age (e.g., smoking, alcohol use, and obesity). 23 Estaville et al. 24 revealed that 59% of university students knew little to very little about cancer. Powe et al. 25 found that nursing students were no different from non-nursing students when it came to perceptions of breast cancer, and only 14% of the nursing students had identified learning about cancer in school.
As part of the education and outreach efforts of the Reid R. Sacco AYA Cancer Program (AYA Cancer Program) at Tufts Medical Center, 26 the program's manager shared her experiences as a young adult patient and survivor in the form of a personal narrative to raise awareness of cancer in AYAs in similarly aged university students, many of whom plan to enter the health care field.
The use of a personal narrative in academic courses that explore the illness experience and/or the American health care system can serve to connect students with biopsychosocial aspects of the disease experience to establish greater contextual links to course material. 27 When narrative-based learning is employed, abstract information becomes more concrete and immediate, creating an emotional response to which students can relate and therefore better remember. 27 A detailed firsthand cancer experience may influence behavior change through perceived identification with the narrator.28–30 Mullan, who shared his survival experience as not one condition, but many, 31 and is credited with coining the term cancer survivor, 32 proposed that firsthand stories are effective in transporting perspective and adding dimension to the issue at hand. 33 According to Ficklen, 34 a good narrative tells a compelling story that draws the listener in. It tells a full story that draws to a resolution and presents an insider's view that the audience would not otherwise know. It also conveys the big picture through the story.
To contribute to the field of AYA oncology, described by Shaw et al. 17 as in its late adolescence, we present a retrospective analysis of feedback collected from university students who heard a personal cancer narrative in one of their scheduled health-related courses. The objectives of the presentation based on experiential and data-driven reasoning and spanning the cancer care continuum are modeled in Figure 1: (1) build awareness of the AYA demographic; (2) demonstrate that healthy AYAs are potentially susceptible to a cancer diagnosis and should therefore have a personal health care focus; and (3) expand awareness of the far-reaching impact of cancer (i.e., psychological, social, and medical). Suggestions regarding the presentation and potential benefits of hearing the narrative are also reported.
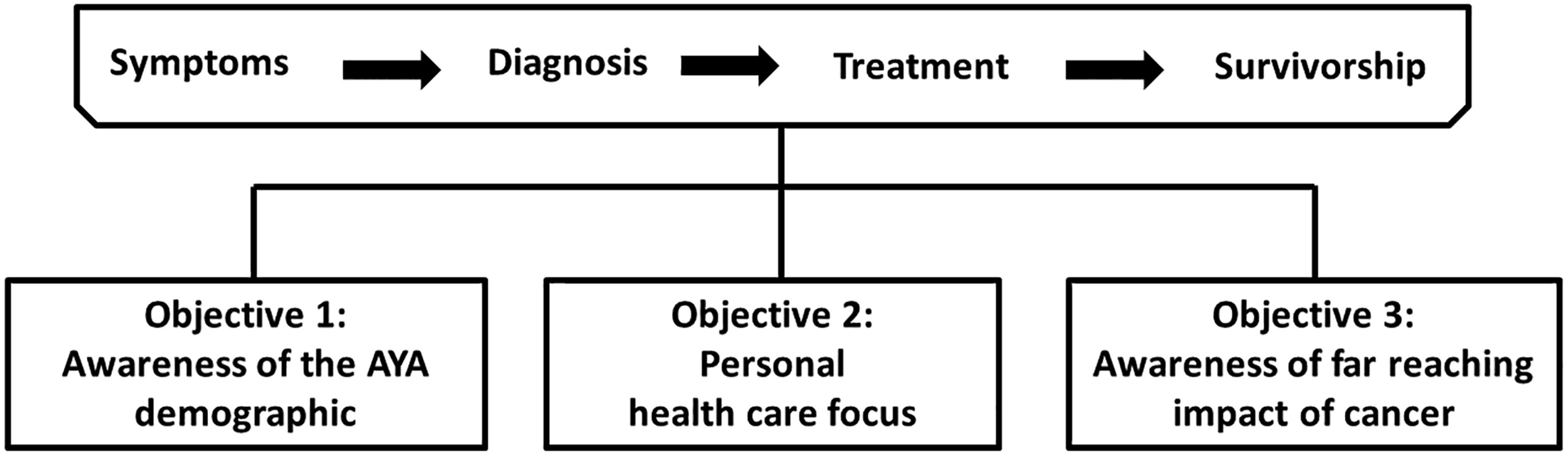
Presentation objectives interwoven across the cancer care continuum. AYA, adolescent and young adult.
Methods
Presentation audiences
Twenty-six invited lectures were given to more than 600 students over 2 academic years (14 in 2016–2017 and 12 in 2017–2018) at four universities and colleges. Invitations to speak varied from professor-initiated, presenter-initiated, or professor-to-professor referral. In total, the presenter (R.M.B.) worked with 10 professors (including coauthors D.B.H. and P.C.H.) and spoke in nine health-related courses within the disciplines of psychology, health sciences, public health, sociology, and literature (Table 1). The audiences ranged from 8 to 55 students, with a mean of 24 students in attendance per presentation.
Students' Connection to Presentation Objectives, Per Course
Each form collected is representative of one student.
Presentation given to multiple sections.
AYA, awareness of the AYA (adolescent and young adult) demographic; health care, personal health care focus; far reach, awareness of far reaching impact of cancer.
Presentation development
The presentation included essential elements of narratives about health care. 34 The PowerPoint opened with a travel photo of the narrator as she explained symptoms of Hodgkin lymphoma she was experiencing at the time, before the cancer had been discovered. The story arc spanned her diagnosis, treatment, and survivorship experiences. Recurrent AYA themes that have been identified in topical literature (e.g., lag time to diagnosis, need for psychosocial support, and unmet needs ranging from information to medical care across the cancer continuum)35–43 were interwoven in the narrative. In addition, evidence-based data were included, such as incidence and prevalence of cancer44,45 and late effect burden of therapy.46,47 By sharing her personal story, the presenter exposed listeners, many of whom have not had cancer or experienced cancer in their peer group, to the voice of an AYA survivor. Approximately 35 minutes were allotted for the delivery of the presentation, followed by time for questions from the audience.
Impact assessment
To assess the impact of these presentations, students were invited at the end of each class to voluntarily provide anonymous written feedback in response to four open-ended questions: (1) What will you take away from this presentation? (2) Has your perspective on (AYA) cancer/survivorship changed? (3) Do you have any suggestions for additional content? (4) Any additional thoughts? Feedback was shared with the AYA Cancer Program's medical director (S.K.P.) and the respective professor. Given the receipt of rich responses, we submitted a proposal to the Tufts Health Sciences Campus Institutional Review Board (IRB) to conduct a deidentified retrospective analysis and disseminate findings to the research community. The IRB determined that this activity did not constitute human subjects research, as defined by federal regulations.
Similar to Fereday and Muir-Cochrane, 48 the subjective perspective of the target population (nurses in the Fereday study and university students in the current study) was sought. A combined deductive and inductive approach was utilized.48,49 The codebook consisted of overarching a priori codes, which aligned with the presentation's objectives to determine if students grasped these themes: (1) awareness of the AYA demographic; (2) personal health care focus; and (3) awareness of the far-reaching impact of cancer (i.e., psychosocial and survivorship). Codes to (4) collect suggestions and (5) investigate how hearing a cancer narrative may have benefited the listener were also included. As noted previously, the objectives were based on the narrator's experience as well as themes identified in the literature. The latter two themes were identified from observational reading of the feedback.
Each of the overarching codes comprised subthemes, explored in detail below (Fig. 2). Constant comparison of responses led to data-driven generation, or expansion, of some subthemes.48,50 A total of 613 forms were collected and assigned a chronological number to assist with systematic coding and illustrative example identification. Two authors (L.B. who had not been previously exposed to the feedback forms and R.M.B.) independently coded each form and then worked together to reach a consensus on all identified themes. Care was taken to not force data into a predetermined code. 49 The broad-scope questions provided the opportunity to capture multiple takeaways of each student; comments were coded by subtheme with no priority given to any one theme. Two forms did not have comments that fit into the a priori themes and therefore were not coded, resulting in 611 usable forms. All consensus-based codes were summarized in an electronic spreadsheet for subsequent analysis. Narrative content from the lecture is included within summaries of themes along with illustrative examples from the students, to strengthen the validity of this analysis.48,49
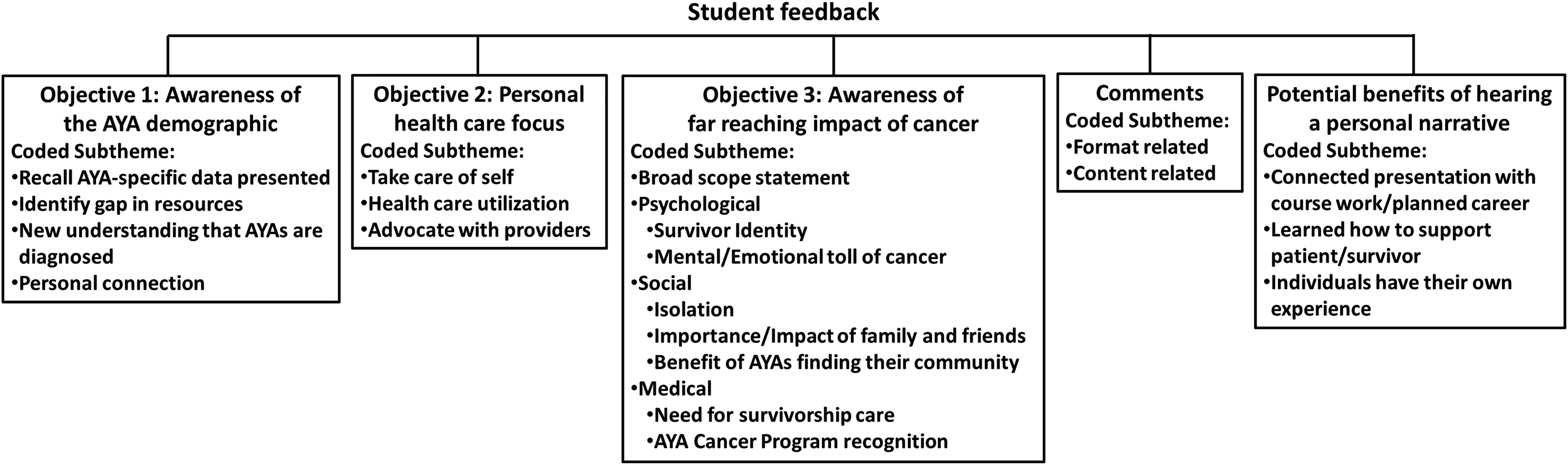
Student feedback by overarching a priori codes, with subthemes.
Results
Students’ feedback is outlined under the framework of the relationship with the presentation's objectives, format or content suggestions, and benefits of hearing a personal narrative (Fig. 2). Ninety-seven percent (n = 593) of students referenced at least one of the objectives, the remaining 3% (n = 18) had only a suggestion and/or referenced a potential benefit. The first and second objectives (i.e., awareness of the AYA demographic and personal health care focus) were clearly differentiated in the feedback. The analysis of the third objective (i.e., imparting awareness of the far-reaching impact of cancer) was found to have overlapping comments and multiple themes, which were categorized as broad-scope statements, psychological, social, or medical. Of the 593 students who referenced the objectives, 37% (n = 222) picked up on one theme, 53% (n = 313) picked up on two themes, and 10% (n = 58) mentioned all three themes (Table 2).
Student Takeaways of Objectives, Identified in Feedback
An overall analysis of the 611 coded forms showed that 58% (n = 352) remarked on the presentation's format, 39% (n = 239) had content suggestions, and 20% (n = 121) identified a benefit of hearing the presentation. Comments related to the presentation's objectives and potential benefits were primarily shared in response to the first two prompts (i.e., takeaways and change in perspective). Content and format suggestions were overwhelmingly provided in response to the last two prompts (i.e., suggestions and additional comments).
Awareness of the AYA demographic
Among the students who referred to an objective, 75% (n = 442) of students demonstrated an awareness of cancer in AYAs. The four subthemes aggregated were recall of the AYA-specific data presented (39%, n = 229), identification of the gap in resources/need for specialized care (32%, n = 188), stated new understanding that AYAs are diagnosed with cancer (17%, n = 100), and a personal connection with an AYA patient/survivor (12%, n = 67) (Fig. 2). Of the 442 students, 70% (n = 310) referenced one, 28% (n = 122) referenced two, and 2% (n = 10) referenced three of the four subthemes, resulting in 584 related comments. Data interspersed within the narrative included the prevalence of cancer as substantially greater in AYAs than in children 44 and an explanation of the American age-based health care system—pediatric and adult. 1 Illustrative responses included: “There is a gap in awareness of this age group. Pediatric cancer is a well-publicized (or perhaps just more publicized) topic, and I tend to associate cancer with grandparent age.” (Student (S) 347); “I am a cancer survivor and literally every other sentence I just kept thinking, that is so true!” (S281).
Personal health care focus
Thirty-two percent (n = 191) of students shared a comment related to the second objective—that of making one's health a priority. Three subthemes for this objective were identified (Fig. 2). The predominant subtheme was to reflect on one's own health (56%, n = 130). One student noted: “the importance of taking care of myself because I am not immune to disease, despite my age” (S204). Students referenced taking care of their physical and/or mental health to promote overall well-being or to prevent cancer or shared an appreciation for their current good health.
The second subtheme, perceived or planned health care utilization, was used to assess if students took-away a focus on personal health care (16%, n = 36); exemplified in the statement: “I'm definitely going to try to actually go to the doctor when I think something is actually wrong. I often just brush issues off and assume I'm ok, but obviously it's important to know that you're healthy when something feels off” (S207). The third subtheme, which 28% (n = 65) of students noted, was the need to self-advocate with health care providers, as demonstrated in the comment: “always ask questions to a health professional if I am worried about or do not understand something” (S84). Inclusion of the presenter's delayed diagnosis experience within the framework of a young adult cancer presentation may have contributed to these subthemes. The majority of students (79%, n = 151) referenced one of the subthemes, while the remaining 21% (n = 40) referred to two, resulting in 231 discrete comments.
Awareness of far-reaching impact of cancer
Sixty-six percent of students (n = 389) endorsed an understanding of the far-reaching impact of cancer, including psychological and social, as well as medical, implications, both during and after completion of therapy (Fig. 2). Nearly half of the respondents (44%, n = 223) offered a broad-scope statement, such as: “My biggest takeaway from this presentation was how the effects that cancer has on an individual's life go much deeper than just battling the disease” (S389) and “I usually wouldn't think about all the long-term impacts of cancer and its treatment. In my mind, it was like once you're cancer-free, you're good, but today helped me realize there is much more to it” (S537).
The remaining 56% (n = 282) responses fell into one of three distinct categories of psychological (11%, n = 53), social (22%, n = 113), or medical- (23%, n = 116) related impact. Comments related to development of a survivor identity51,52 or the mental or emotional toll of cancer 41 were categorized as psychological. The social category contained themes identified in AYA literature and experienced by the presenter, including social isolation, which may be a result of being the youngest/oldest person in the waiting room and/or separation or lack of understanding from peers,53–56 the importance of and impact on family and friends,41,43,56 and the benefit AYAs may feel from finding a community of other AYA patients/survivors. 41 Comments coded as medical related noted the need for long-term follow-up care or remarked on the AYA Cancer Program the presenter represented. Potential treatment-related late effects experienced by survivors correlated with the presenter's description of her survivorship care-related work. Seventy-three percent (n = 285) of these students referenced one subtheme, 24% (n = 92) referenced two, and 3% (n = 12) referenced three of the four subthemes, resulting in 505 related comments.
Format and content suggestions
Due to the potentially difficult and emotionally charged subject matter, consideration was given to the format and delivery, in addition to the content, of the presentation. Slides included a mixture of images (i.e., graphics and one photograph) and bullet-pointed text. The presenter spoke in a relaxed conversational style and engaged students with direct eye contact and facial expressions. Fifty-eight percent (n = 352) of students commented on how the presentation was delivered. The majority of comments expressed appreciation of the personal narrative aspect exemplified by the statement: “Being able to hear a first-person account of actually experiencing cancer was helpful in driving home messages” (S465). Additional comments are described in Table 3. Of the 611 forms coded, 39% (n = 239) included content suggestions. Suggestions, listed in Table 3, ranged from requests for more information about cancer to recommendations to include other patient testimonials.
Student Comments/Suggestions
A total of 352 students provided format-related comments or suggestions (n = 317 offered one, n = 34 offered two, and n = 1 offered three, resulting in 388 remarks).
A total of 239 students provided content-related comments or suggestions (n = 223 offered one, n = 15 offered two, and n = 1 offered three, resulting in 256 remarks).
Benefits of hearing a personal cancer narrative
Raising awareness of cancer in AYAs has multiple potential benefits, in addition to changes in personal health care explored earlier. Twenty percent (n = 121) of the students connected an aspect of the presentation to what they were learning in school and/or their planned career path. One student shared: “I'm learning about cancer in my cell biology class right now. This talk has really made me zoom out on to the personal/social level” (S154). Students also expressed feeling they would be a better supporter to someone with cancer (14%, n = 88), illustrated by the statement: “I took away from the presentation how to be there for a young friend (or anyone) who is going through cancer and how to make them comfortable” (S93). In an effort to minimize generalizations of the speaker's experience to all patients, students were reminded this was just one story, and while similarities may occur, each person has his/her own unique experience. 32 This sentiment appeared to resonate with the audience as 8% (n = 47) of students specifically commented on the individuality of the cancer experience.
Discussion
AYA advocates have called for studies that include off-treatment survivors, 39 pertain specifically to AYAs,40,57 and address quality of life and late effects experienced by these survivors.11,17,46 These concepts were featured in the personal narrative delivered as part of an educational initiative to raise awareness of cancer in AYAs in similarly aged university students. Student feedback reflected the presentation's objectives: (1) AYAs are not immune to cancer; (2) one's own health should be prioritized; and (3) cancer has far-reaching physical and psychosocial impacts across the cancer care continuum. Additionally, students provided suggestions and comments about the presentation that may be incorporated in future talks as well as indicated potential benefits of hearing a personal narrative (e.g., connecting the narrative with coursework or future career goals). A concrete benefit to the AYA Cancer Program has been participation of three student volunteers.
We acknowledge the study's limitations. First, the overarching objectives and broad open-ended prompts given to students provided the opportunity to capture any takeaway by the students, but may be seen as too generalizable to assess impact. Second, the presenter acted as one of the coders, which may result in some bias in interpretation of student comments. This potential shortcoming was addressed by adding an independent coder who had not been a part of the presentation. Third, the retrospective one-time assessment does not enable us to measure how long students retained their understanding or to link cause awareness to behaviors or other outcomes. Fourth, while the core narrative content remained the same in each course, slight modifications were made over time and/or in different courses, which may have influenced the student responses. Despite these limitations, strengths include the large sample size and extensive feedback collected from the students across multiple classes and institutions. Future inquiry should be extended to include an exploration of concrete outcomes from hearing the presentation (e.g., whether or not a student sought care from a health care provider) and the inclusion of diverse AYA perspectives (e.g., feature financial impact and university-aged diagnosis).
Embedding a personal AYA narrative presentation in combination with evidence-based data within health-related university courses is feasible, engaging, and beneficial. The students' feedback suggests that this innovative educational model has the potential to increase knowledge and awareness of the AYA cancer experience while also providing a more meaningful appreciation for the complexity of the health care system and biopsychosocial impact of cancer. One student shared: “This was a very powerful presentation of a topic that some might be hesitant to talk about openly. I believe presentations like this will help break down ‘the elephant in the room' for people who don't know how to talk to family and friends who have cancer and serve as a call to action for education and support for members of the AYA cancer community” (S127).
Footnotes
Acknowledgments
The authors wish to thank the engaged students and their professors who saw the benefit of including awareness of adolescent and young adult (AYA) cancer in the curriculum. The authors thank the members of the Reid R. Sacco AYA Cancer Alliance, in particular Lorraine and Gene Sacco, as well as Michael Marra, and Nadine Linendoll for their continued support.
Author Disclosure Statement
No competing financial interests exist for the authors.